Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251115_010
Coronary-Cusp Balloon-Assisted Laceration and Transcatheter Aortic Valve Implantation
By John Jose Erungaren
Presenter
John Jose Erungaren
Authors
John Jose Erungaren1
Affiliation
Christian Medical College Hospital Vellore, India1
View Study Report
CASE20251115_010
Structural - Aortic Valve Intervention - Complex TAVR
Coronary-Cusp Balloon-Assisted Laceration and Transcatheter Aortic Valve Implantation
John Jose Erungaren1
Christian Medical College Hospital Vellore, India1
Clinical Information
Relevant Clinical History and Physical Exam
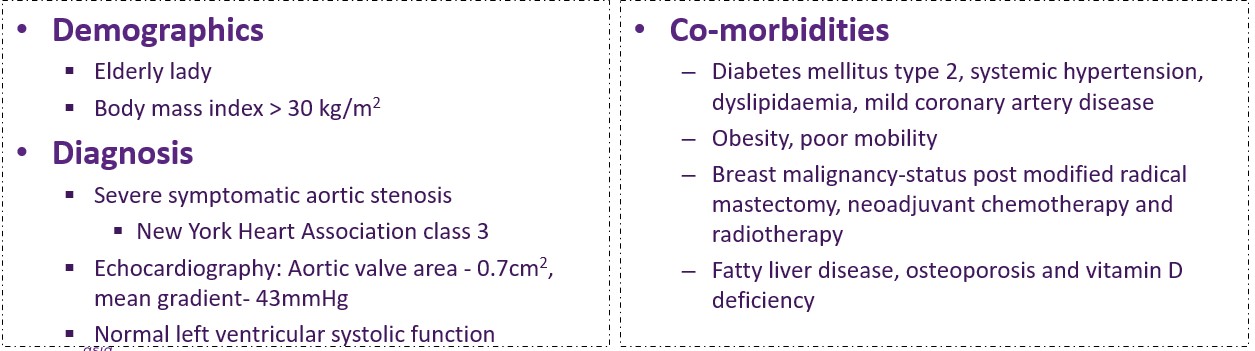
Elderly lady with severe symptomatic aortic stenosis
Co-morbiditiesDiabetes mellitus type 2,systemic hypertension, dyslipidaemia, mild coronary artery diseaseObesity, poor mobilityBreast malignancy-status postmodified radical mastectomy, neoadjuvant chemotherapy and radiotherapyFatty liver disease, osteoporosisand vitamin D deficiency
Relevant Test Results Prior to Catheterization
CAG- Minor disease. Separate origin of LAD and LCX from left sinus.High-risk CT features for coronary obstruction by sinus sequestration post-TAVI :
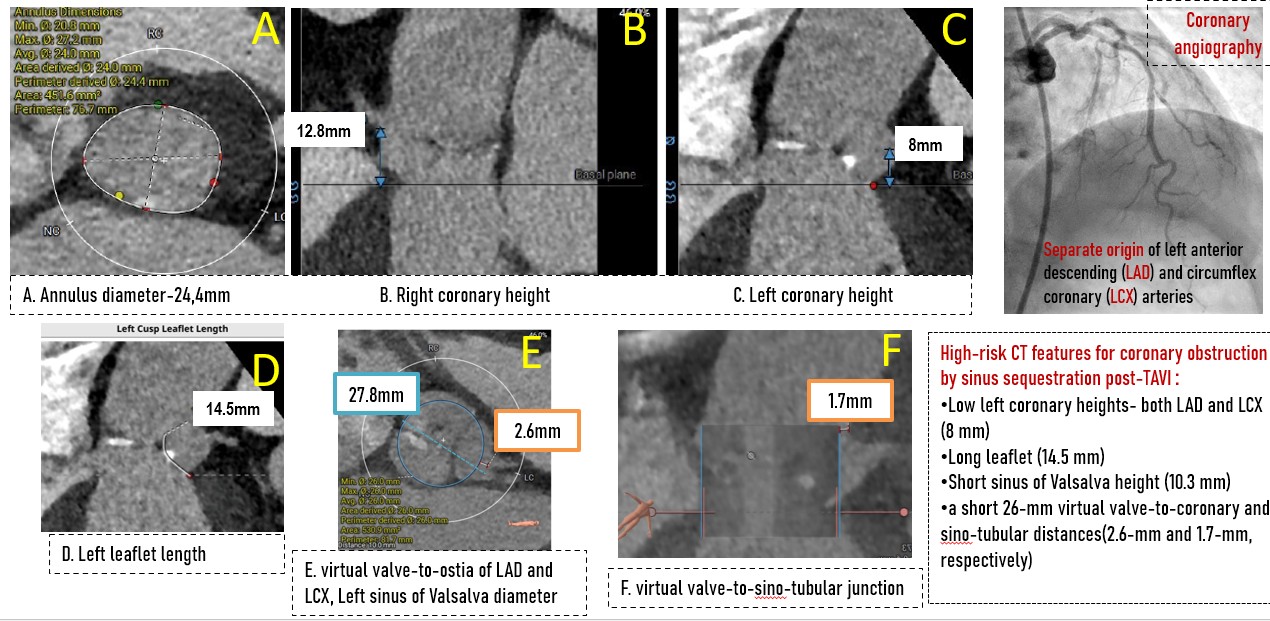
•Lowleft coronary heights- both LAD and LCX (8 mm)
•Longleaflet (14.5 mm)
•Shortsinus of Valsalva height (10.3 mm)
•ashort 26-mm virtual valve-to-coronary and sino-tubulardistances(2.6-mm and 1.7-mm, respectively)
Relevant Catheterization Findings
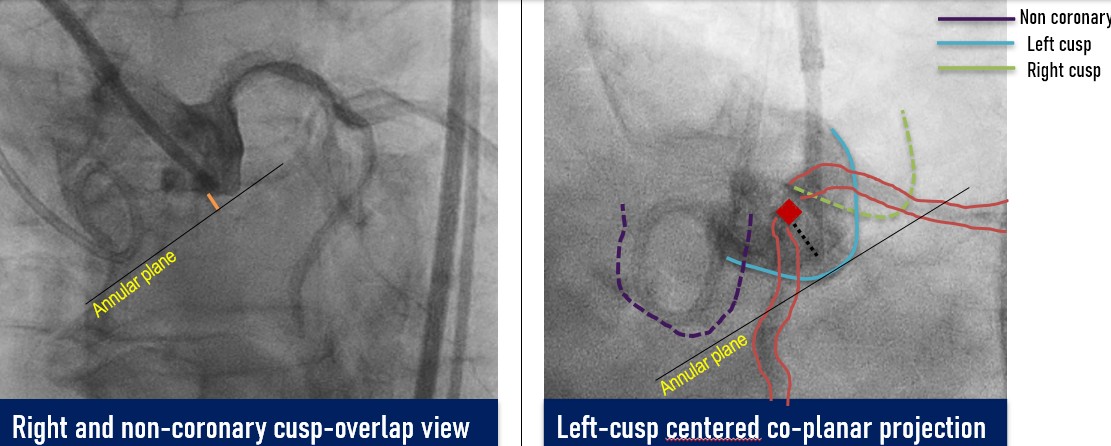
Coronary angiogram showed minor disease. Root angiography done to identify and isolate views for procedure
Interventional Management
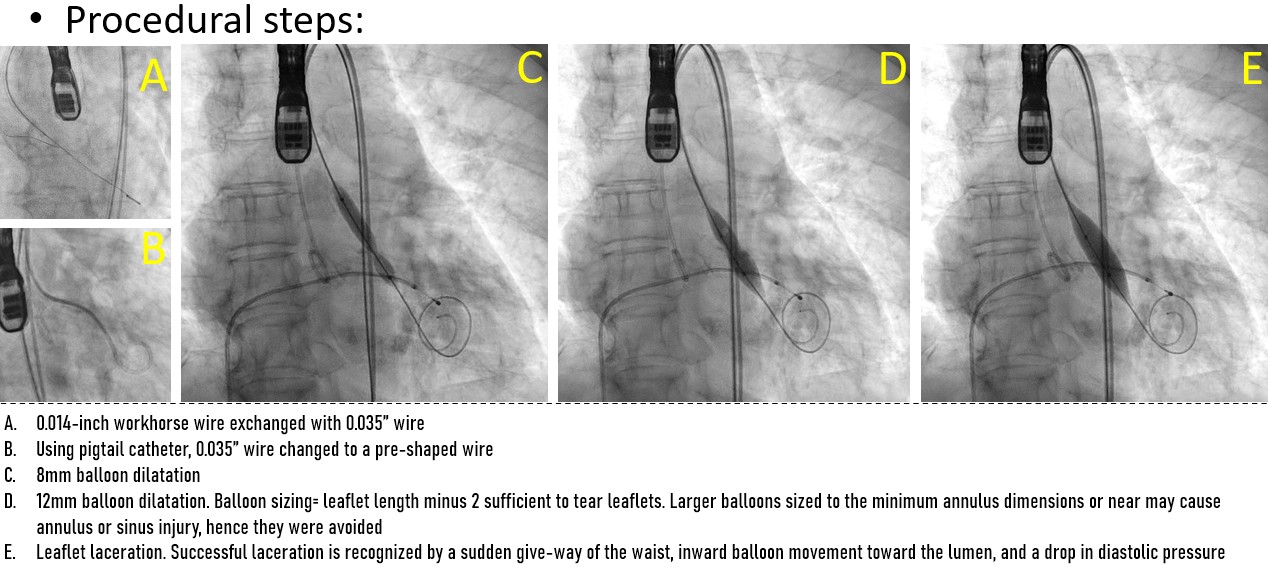
Procedural Step
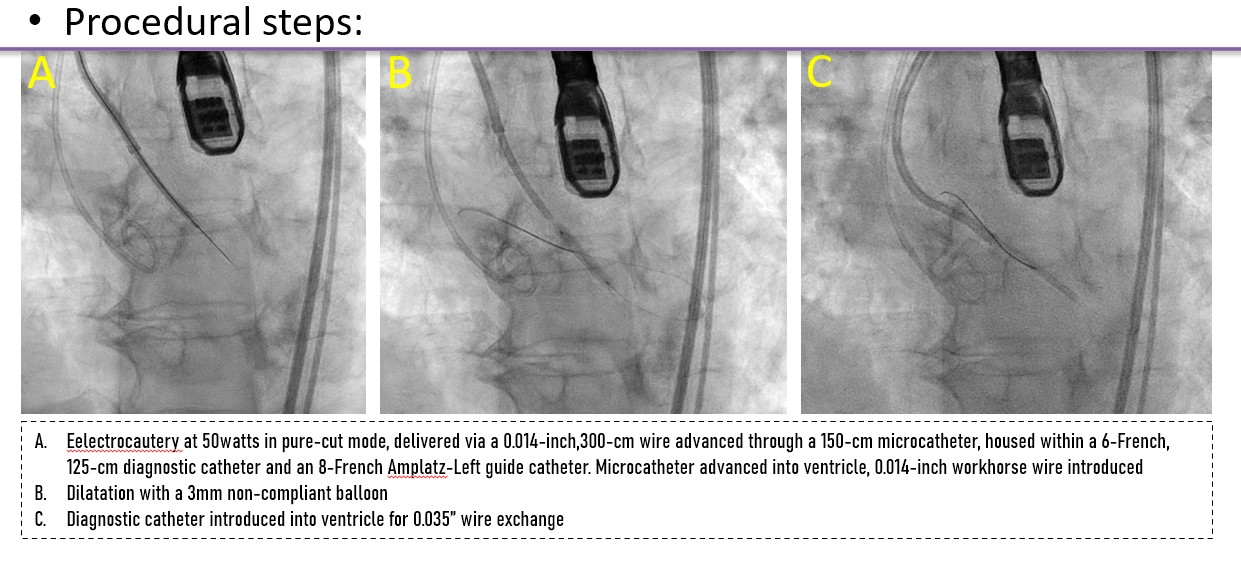
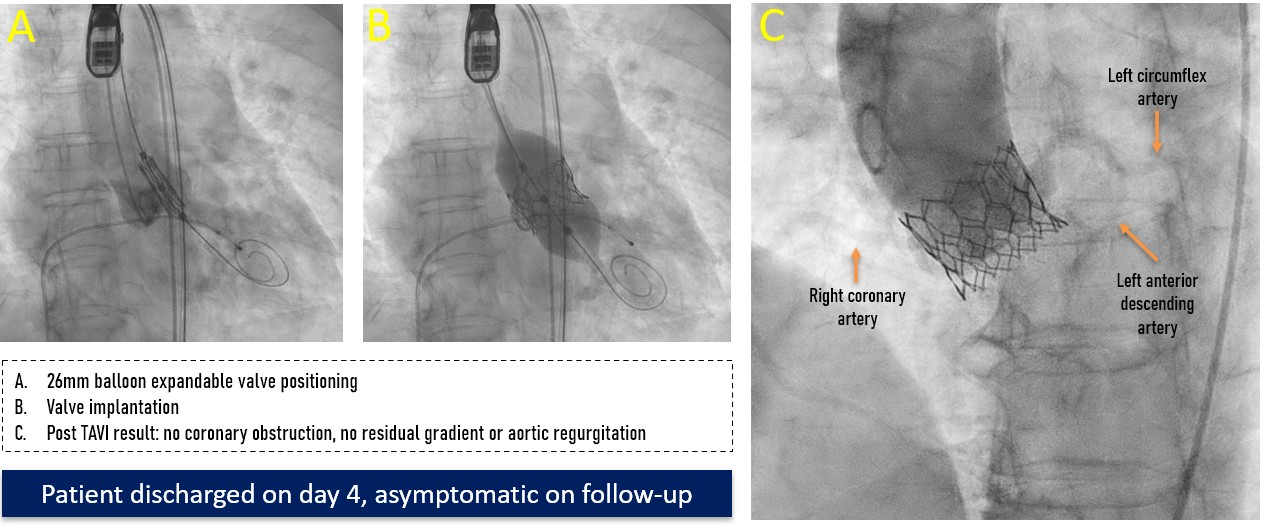
A controlled laceration of the native left coronary cusp was planned under general anaesthesia. A puncture point 2 mm above the cusp base, aligned with the coronary ostium, was selected to ensure optimal leaflet splay and minimise recoil risk following laceration. Leaflet traversal was performed using electrocautery at 50 W in pure-cut mode, delivered through a 0.014-inch, 300-cm Astato wire (ASAHI) advanced via a 150-cm Finecross microcatheter (Terumo), housed within a 6-French, 125-cm multipurpose diagnostic catheter and an 8-French Amplatz Left guide catheter. After advancing the microcatheter into the left ventricle, the Astato wire was exchanged for a 0.014-inch Fielder wire. Initial dilatation was performed using a 3 mm non-compliant Apollo balloon (BrosMed Medical). The Fielder wire was then exchanged for a 0.035-inch, 260-cm J-tip wire, and subsequently for a pre-shaped Safari wire (Boston Scientific). Based on procedural planning, a balloon size equal to or up to 2 mm shorter than the leaflet length was deemed adequate to achieve effective laceration while avoiding sinus or annular injury. Controlled leaflet laceration was performed using sequential balloon dilatations with an 8-mm Armada balloon (Abbott Cardiovascular) followed by a 12-mm Mustang balloon (Boston Scientific). Successful laceration was indicated by a sudden give-way of the balloon waist, inward balloon shift toward the lumen, and a drop in diastolic pressure. A balloon-expandable valve was implanted.
 Media5.mp4
Media5.mp4
Case Summary
•The COBALT technique (Coronary-cuspballoon-assisted controlled laceration and TAVI)
§Anovel modification designed for native valve TAVI in patients with highcoronary obstruction risk
§Steps: systematic strategy
•Careful CT planning for coronaryobstruction risk stratification
•Point of puncture : 2mmabove the base of the cusp
•Controlled leaflet lacerationusing sequential balloon dilatation of 4-5mm increments
•Final Laceration balloon size= leafletlength minus 2mm
•Immediate valve deployment withno coronary obstruction or paravalvular leak
•Step-wise, adaptable to nativevalves as well as valve in valve TAVIs, and technically simpler than BASILICA