Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251115_006
Orbital Atherectomy in Balloon Uncrossable Lesions With Heavy Calcium
By Tanuj Bhatia
Presenter
Tanuj Bhatia
Authors
Tanuj Bhatia1
Affiliation
SGRRIH & MS, India1
View Study Report
CASE20251115_006
Coronary - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Orbital Atherectomy in Balloon Uncrossable Lesions With Heavy Calcium
Tanuj Bhatia1
SGRRIH & MS, India1
Clinical Information
Relevant Clinical History and Physical Exam
A 65 year post menopausal women came with history fo chest pain for 2 days, more for 12 hours. She had past history of angina. ECG revaled q waves with t inversion in inferior leads. Echo showed RWMA in inferior wall with EF of 40%.
 4_RCA_OCT.mp4
4_RCA_OCT.mp4
RCA_Pre.mp4
RCA_Pre_2.mp4
Relevant Test Results Prior to Catheterization
Hb = 11.3Cr = 0.9hsCRP = 3LDL= 97
Relevant Catheterization Findings
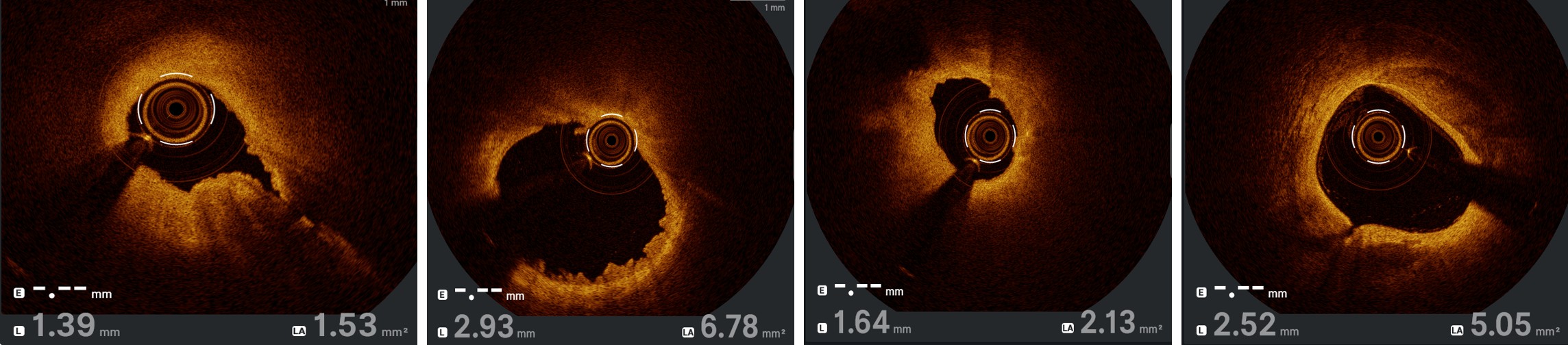
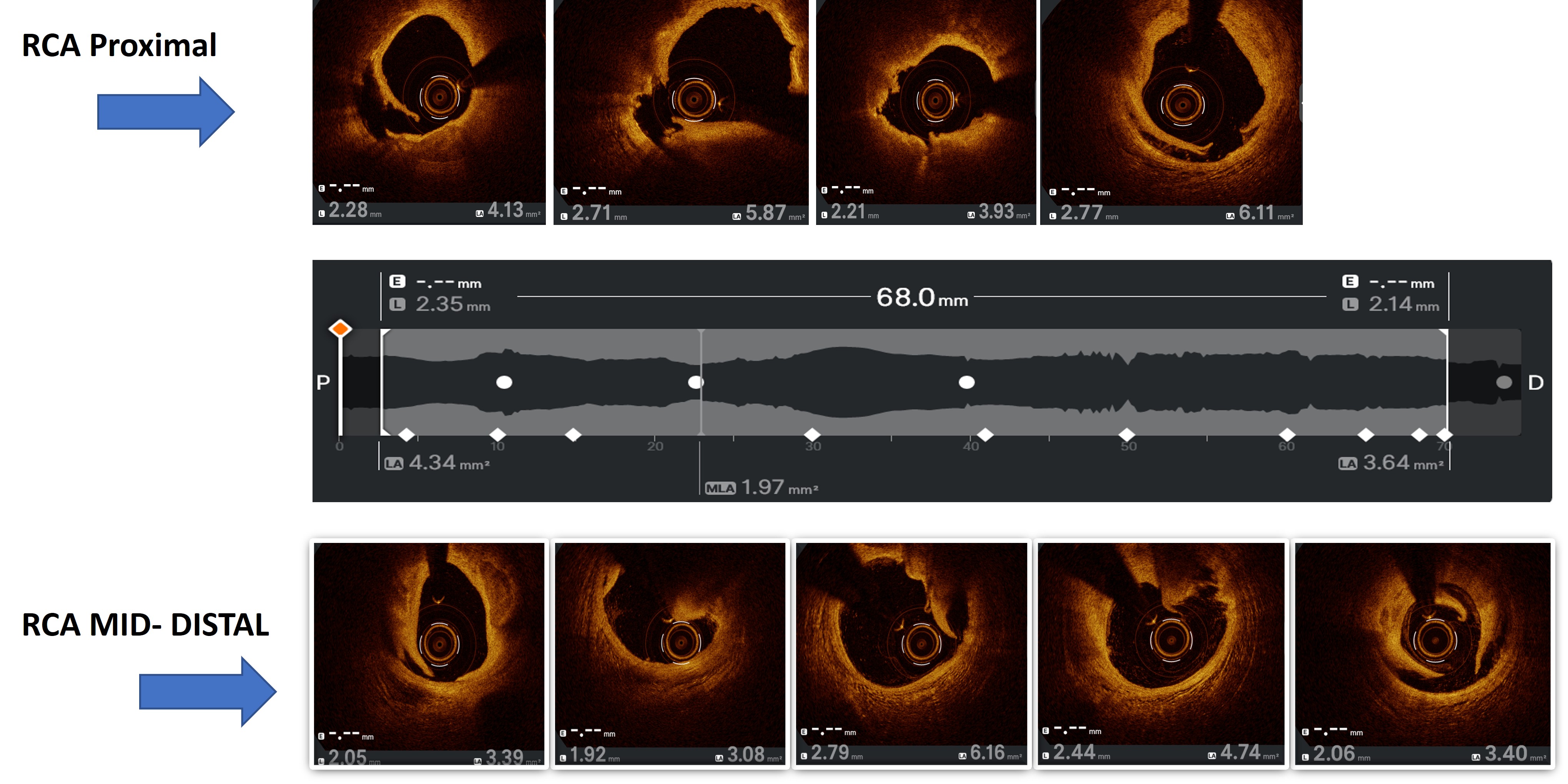
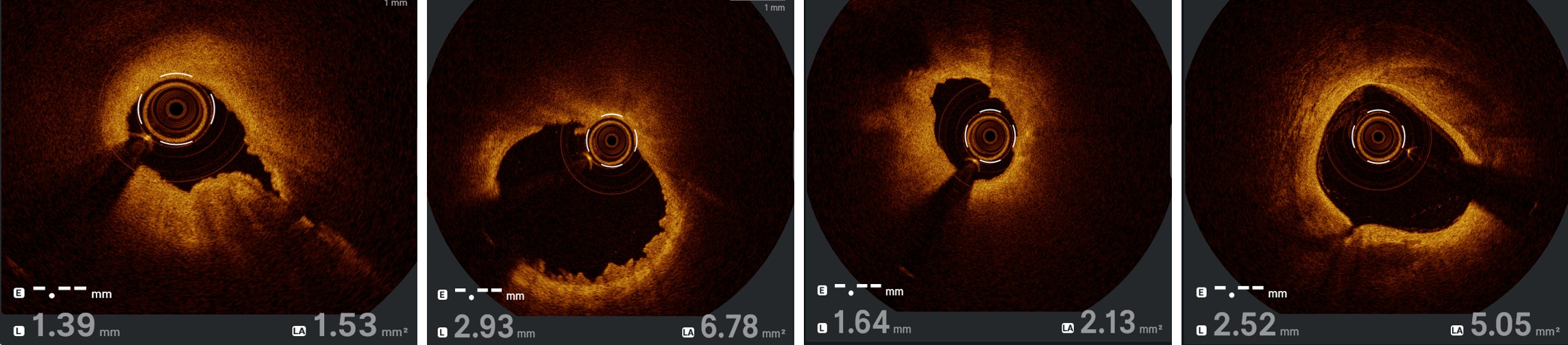
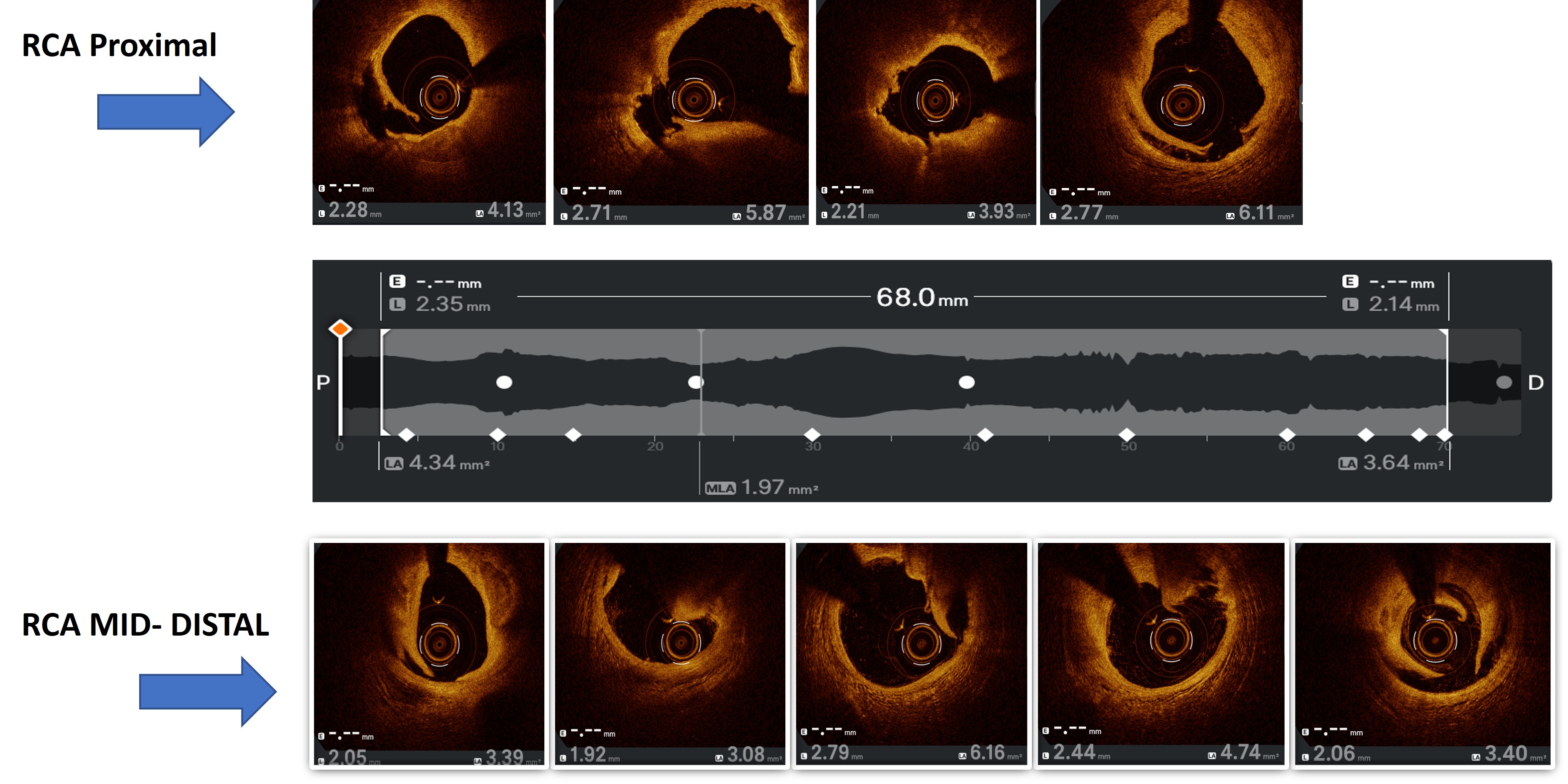
RCA lesion was difficult to cross and Fileder XT was crossed with microcatheter support. therafter, there was difficulty in negotiating the 1.0 mm balloon also. Fluroscopically, there was heavy calcium with nodular appearance (hump sign). The wire was exchanged for Viper wire and Orbital Atherectomy was initiated at 80,000 rpm for 160 seconds.
After patient sanding, OCT revealed significant reduction in the superficial clacium, and evidence of calcium fractures. Sato OCT score was reduced to 1.
RCA_OA.mp4
5_RCA_Post OA.mp4
8_RCA_Post_OCT.mp4
After patient sanding, OCT revealed significant reduction in the superficial clacium, and evidence of calcium fractures. Sato OCT score was reduced to 1.
Interventional Management
Procedural Step
Step 1 - Crossing the wire with Fielder XT wire, Microcatheter support, RAO view
Step 2 - Balloon Uncrossable
Step 3 - Upfront Orbital atherectomy
Step 4 - Fluroscopic as well as OCT downgrading of Calcium
Step 5 - OA again at 1,20,000 rpm & NC balloon
Step 6 - OCT documentation of differential sanding and fractures
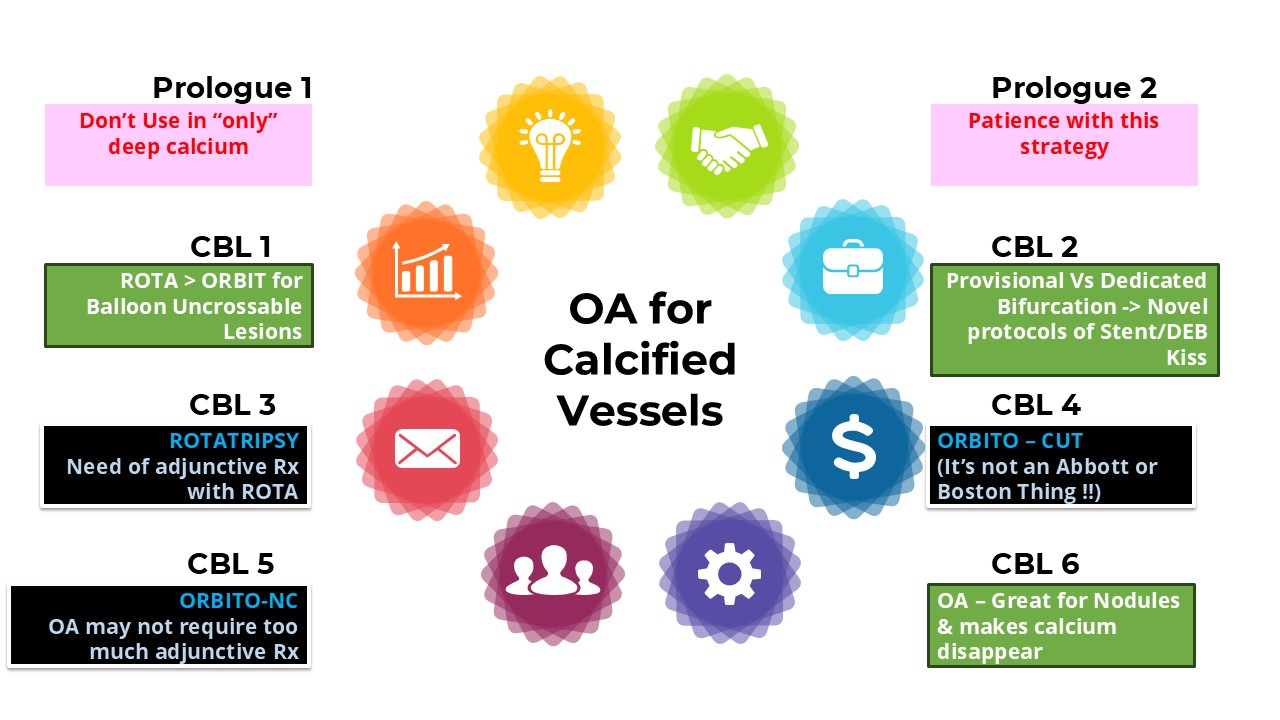
Orbital Atherectomy is a good alternative to rotablation for balloon uncrossable lesions. It affects both superficial as well as deep calcium, by ablative techniques, centrifugal force as well as pulsatile forces. But, requires patience as compared to rotablation. Possibly, best results start after 10 patient runs.
6_RCA_Final.mp4
Step 2 - Balloon Uncrossable
Step 3 - Upfront Orbital atherectomy
Step 4 - Fluroscopic as well as OCT downgrading of Calcium
Step 5 - OA again at 1,20,000 rpm & NC balloon
Step 6 - OCT documentation of differential sanding and fractures
Orbital Atherectomy is a good alternative to rotablation for balloon uncrossable lesions. It affects both superficial as well as deep calcium, by ablative techniques, centrifugal force as well as pulsatile forces. But, requires patience as compared to rotablation. Possibly, best results start after 10 patient runs.
Case Summary
Orbital Atherectomy is a good technique to manage both superficial as well as deep calcium, in combination, especially when there is wire crossability but no balloon crossability. However, needs more patience than rotablation. Chances of slow flow are lesser as compatred to rota. Its ability to ablate calcium in retrograde fashion is an additional feature and virtually eliminates the fear of Kokesi phenomenon that we had with rotablation.