Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251115_002
Refractory In-Stent Restenosis: Lessons From a Never-Ending Battle
By Andrico Tobing
Presenter
Andrico Tobing
Authors
Andrico Tobing1
Affiliation
Murni Teguh Memorial Hospital, Indonesia1
View Study Report
CASE20251115_002
Coronary - Complex PCI - In-Stent Restenosis
Refractory In-Stent Restenosis: Lessons From a Never-Ending Battle
Andrico Tobing1
Murni Teguh Memorial Hospital, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
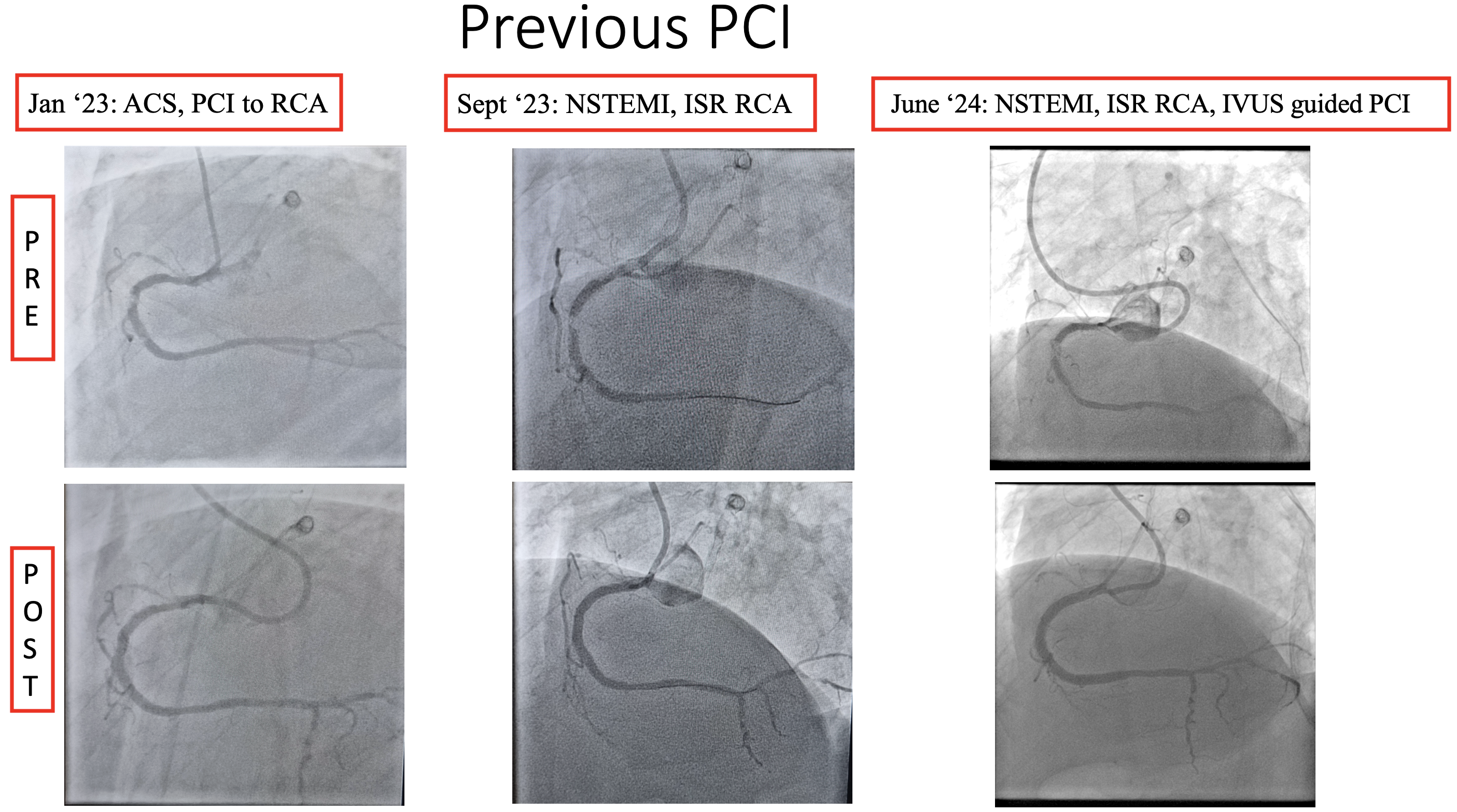
A 63-year-old male with a history of type 2 DM, hypertension, chronic kidney disease, and dyslipidemia was admitted with a NSTEMI. He had previously undergone PCI to the LAD and multiple PCIs to RCA a few months prior. The patient was a heavy smoker and had poorly controlled diabetes. His vital signs were stable on admission. Laboratory evaluation revealed hemoglobin 10.5 g/dL, estimated glomerular filtration rate (eGFR) 25 mL/min/1.73 m², and elevated troponin levels.
Relevant Test Results Prior to Catheterization
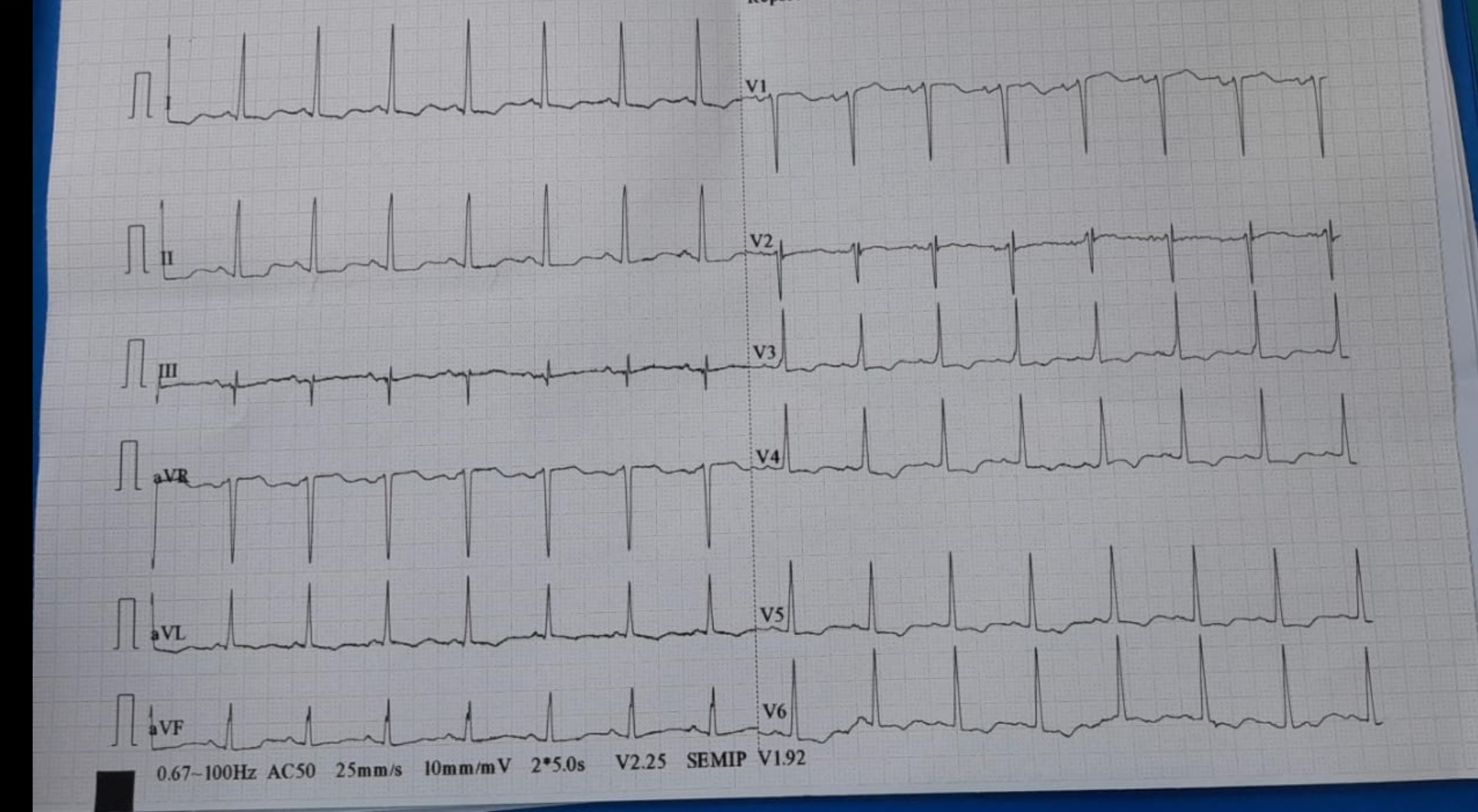
ECG showed Sinus rhythm and ST depression on inferolateral leads. Echocardiography showed EF 53 %, inferior wall hypokinetic, mild Mitral Regurgitation with LVH.
Relevant Catheterization Findings
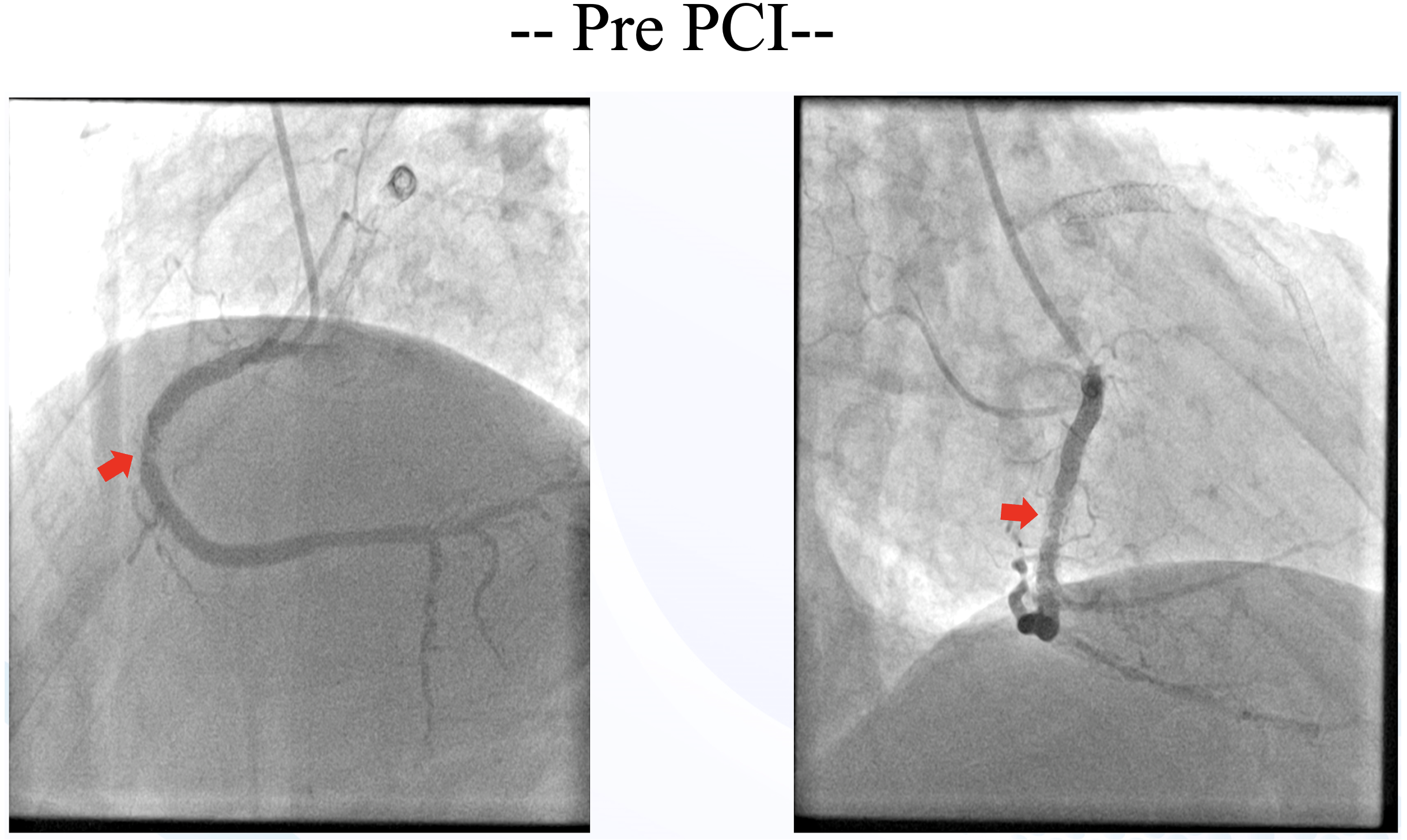
Just 6 months after last PCI, the patient was readmitted back with NSTEMI. Left coronary angiography showed patent LAD stent and diffuse non-significant stenosis of the LCx (consistent with prior angiography). Right coronary angiography showed significant recurrent In-stent restenosis (ISR) in mid RCA.
Interventional Management
Procedural Step
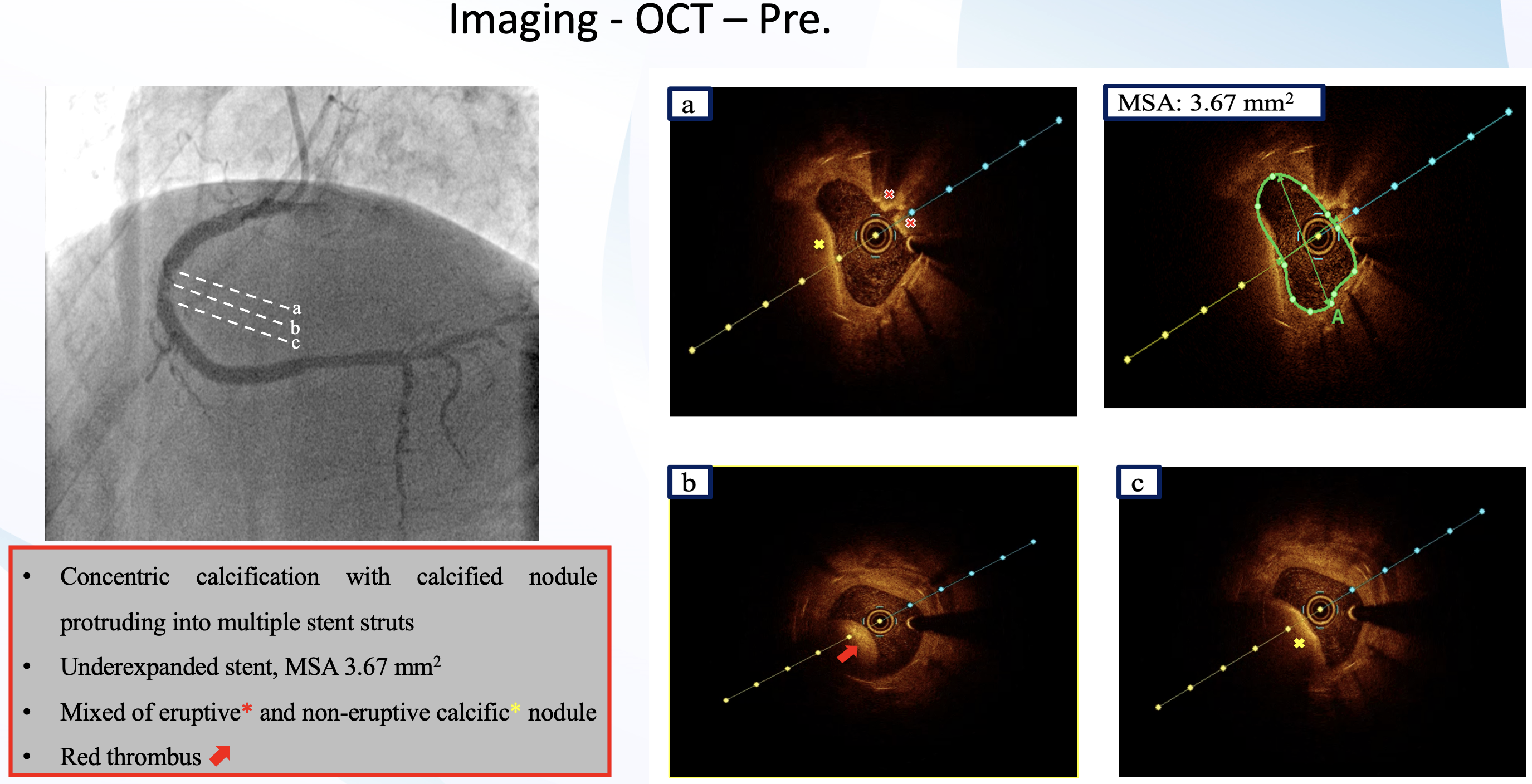
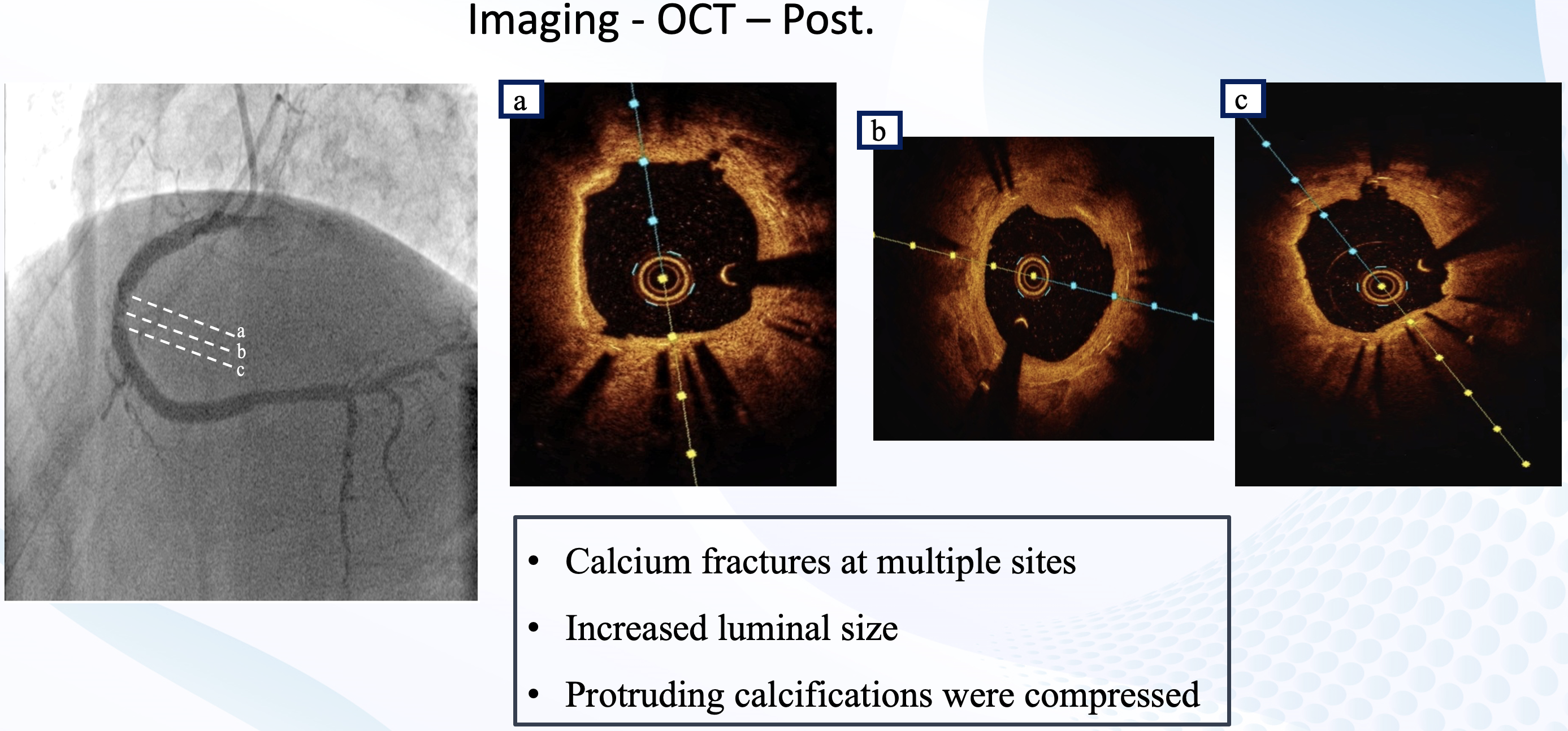
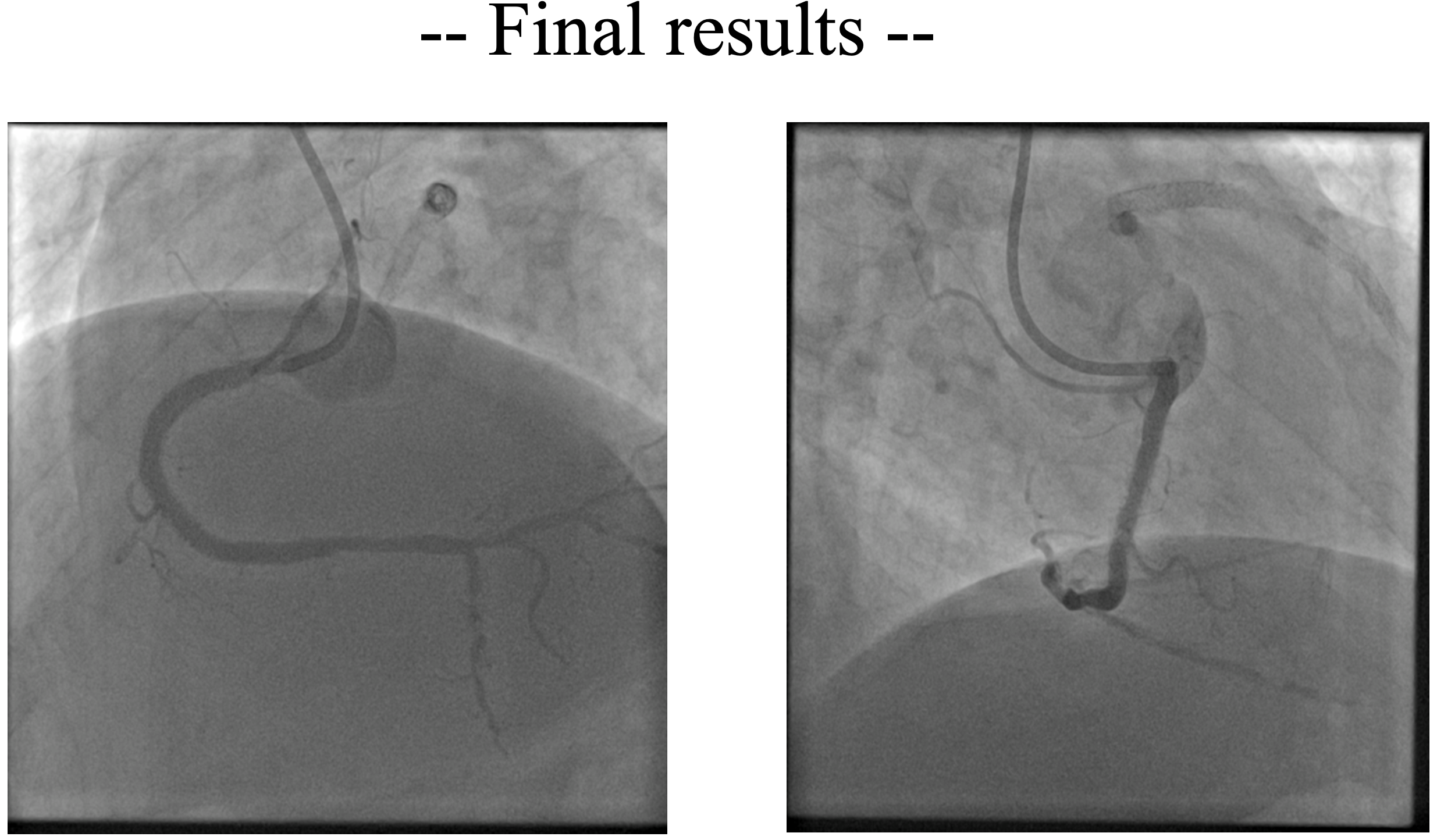
Right radial access was obtained, right coronary ostium was selectively cannulated with 6F Hockey stick guiding catheter. Runthrough NS wire was advanced into the distal RCA. Optical coherence tomography (OCT) using saline was performed to minimize the risk of worsening kidney function. OCT revealed concentric calcification with both eruptive and non-eruptive calcific nodules protruding through multiple stent struts, resulting in stent underexpansion (MSA 3.67 mm2). Red thrombus was also present around the lesion. Predilatation with a 3.5 x15 mm cutting balloon using controlled, prolonged inflation up to 12 atm was attempted; a persistent “waist” was observed, indicating inadequate lesion modification. For better lesion preparation, then we performed Intravascular Lithotripsy (IVL) using Shockwave 3.5 x12 mm C2 IVL balloon and 80 pulses were delivered at mid RCA. IVL balloon expansion was satisfactory at 6 atm, and no residual waist observed. OCT after IVL showed calcium fractures at multiple sites and compression of protruding calcifications, with increased luminal area. Further dilation was performed with 3.5 x 15 mm NC balloon. This was followed by delivery of a 4.0 x 20 mm paclitaxel-eluting balloon (DEB) at the mid RCA for 60 seconds. Final angiography and OCT evaluation showed excellent results, with MSA improved from 3.67 mm² to 7.71 mm².
Case Summary
Calcified nodules—defined as eruptive calcifications protruding into the coronary lumen with overlying thrombus—account for 2–8% of acute coronary syndromes and are associated with recurrent in-stent restenosis and worse outcomes after PCI. Imaging guidance and adequate lesion preparation are essential to improve procedural outcomes. Drug-eluting balloons (DEB) are a valid treatment option for ISR, as they avoid additional layers of metal or longer stents, which may increase the risk of late adverse events.