Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_056
Salvaging the Nightmare – Percutaneous Retrieval of the Unraveled Trapped Wire
By Chin Wai Lai
Presenter
Chin Wai Lai
Authors
Chin Wai Lai1
Affiliation
United Christian Hospital, Hong Kong, China1
View Study Report
CASE20251114_056
Coronary - Complication Management
Salvaging the Nightmare – Percutaneous Retrieval of the Unraveled Trapped Wire
Chin Wai Lai1
United Christian Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
A 49year-old man with long standing smoking history and diabetes presented with non ST elevation myocardial infarction and acute pulmonary edema. He had on and off exertional angina but did not seek medical attention before.

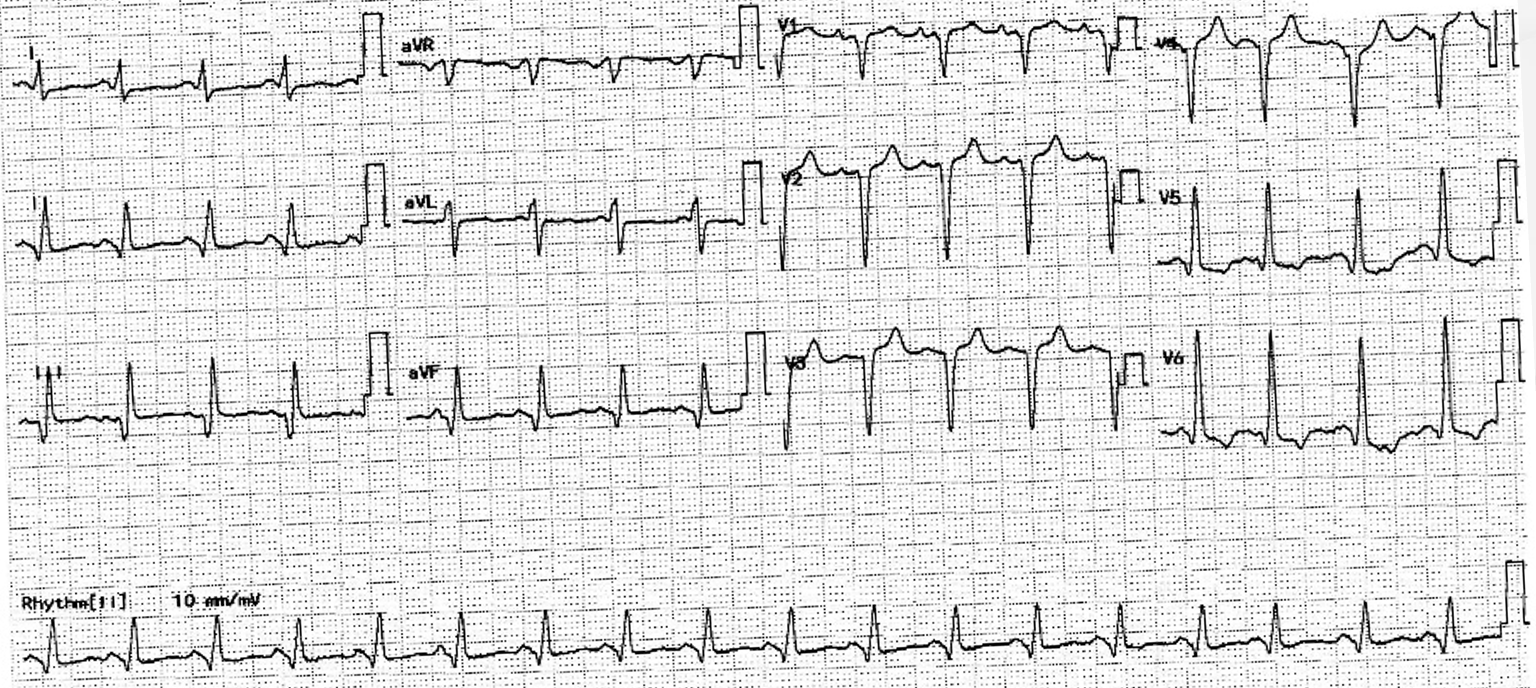
Relevant Test Results Prior to Catheterization
Electrocardiogram showed poor R wave progression and inferior leads Q wave. Cardiac enzymes were elevated. Echocardiogram showed severely impaired LVEF at 20% with multiple regional wall hypokinesia.
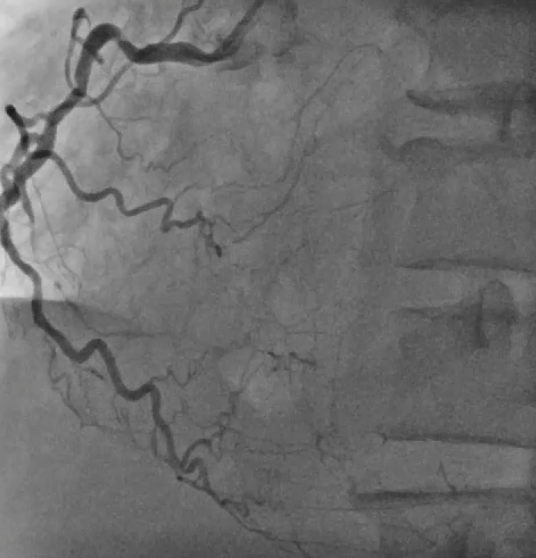
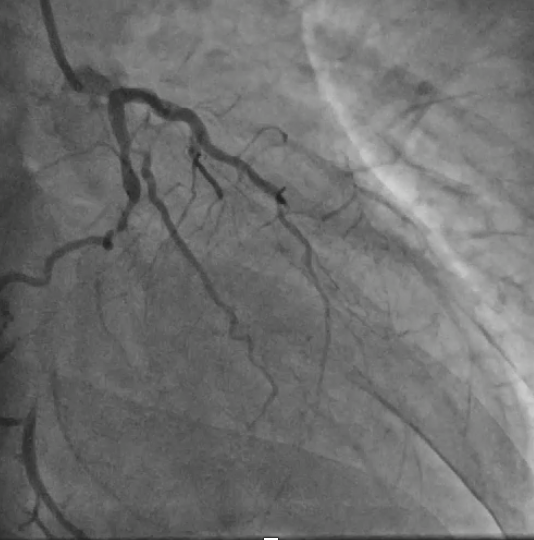
Relevant Catheterization Findings
Coronary angiogram showed CTO in all 3 vessels. Impella assisted PCI was suggested in combined HEART team meeting in view of high surgical risk (STS score >8). Antegrade approach was adapted. LAD CTO was successfully crossed with Gaia Next 1 with Turnpike support. A 2.25x40mm stent was deployed to mid LAD and an overlapping 3.5x28mm stent was deployed to LM-LAD across wire protected LCx. Post dilatation was performed. Final IVUS and angiogram showed satisfactory result.
 002LAD.mp4
002LAD.mp4
Interventional Management
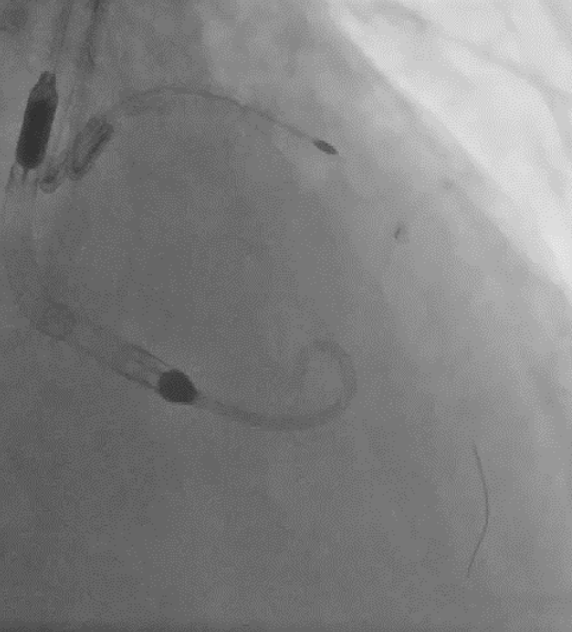
Procedural Step
Upon removal of the workhorse wire from distal LAD, an unforeseen nightmare started. The wire tip entangled with the distal stent edge. Turnpike microcatheter was used to retrieve the stuck wire. Unfortunately, upon pullback, the wire fractured and only its proximal part was retrieved. The distal part remain stuck in the distal stent edge and uncoiled with filaments extending from stent edge into aorta. PingPong guiding was immediately set up. ClearStent showed distal stent edge deformity which rendered passage of any device including 1.0mm balloon impossible. In order to modify the obstructing stent struts at distal edge, it was decided to use rotablation. Direct wiring across the deformed distal stent edge with rota wire was successful. Pecking motion of rotablation was performed with the aim to clear the obstructing scaffolds. After 25 runs at high speed with 1.5bur, the deformed distal stent was successfully crossed. The trapped wire tip was unexpectedly released and fell into the septal branch. The fractured filaments were assessed with IVUS and ClearStent. Subsequently, the filaments were all retrieved with 2 twisting wires. IVUS confirmed complete clearance of any filament. The LM-LAD stent was again post dilated and optimized. Final angiogram and follow up restudy 4months later both showed satisfactory result with patent stents.


18twitchwire.mp4
Case Summary
In this case, combined use of rotablation atherectomy and twisting wires successfully salvaged a nightmare and saved the patient from extremely high risk open heart surgery. Staying calm, using essential PCI techniques, different devices and imaging are the keys in tackling potential life threatening complications.