Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_054
From CTO to Dissection: Managing Catheter-Induced Aorto-Ostial Dissection in a Complex RCA PCI
By Wasan Udayachalerm, Chii Koh Wong, Houng Bang Liew
Presenter
Chii Koh Wong
Authors
Wasan Udayachalerm1, Chii Koh Wong2, Houng Bang Liew2
Affiliation
King Chulalongkorn Memorial Hospital, Thailand1, Hospital Queen Elizabeth II, Malaysia2
View Study Report
CASE20251114_054
Coronary - Complication Management
From CTO to Dissection: Managing Catheter-Induced Aorto-Ostial Dissection in a Complex RCA PCI
Wasan Udayachalerm1, Chii Koh Wong2, Houng Bang Liew2
King Chulalongkorn Memorial Hospital, Thailand1, Hospital Queen Elizabeth II, Malaysia2
Clinical Information
Relevant Clinical History and Physical Exam
A 70-year-old male with background hypertension and dyslipidemia presented with sudden onset presyncope while seated, without accompanying chest pain or palpitations. Initial assessment showed 174/80mmHg, 73bpm, unremarkable physical examination. He was diagnosed with NSTEMI. Patient declined CABG and adamant for high-risk PCI.
Relevant Test Results Prior to Catheterization
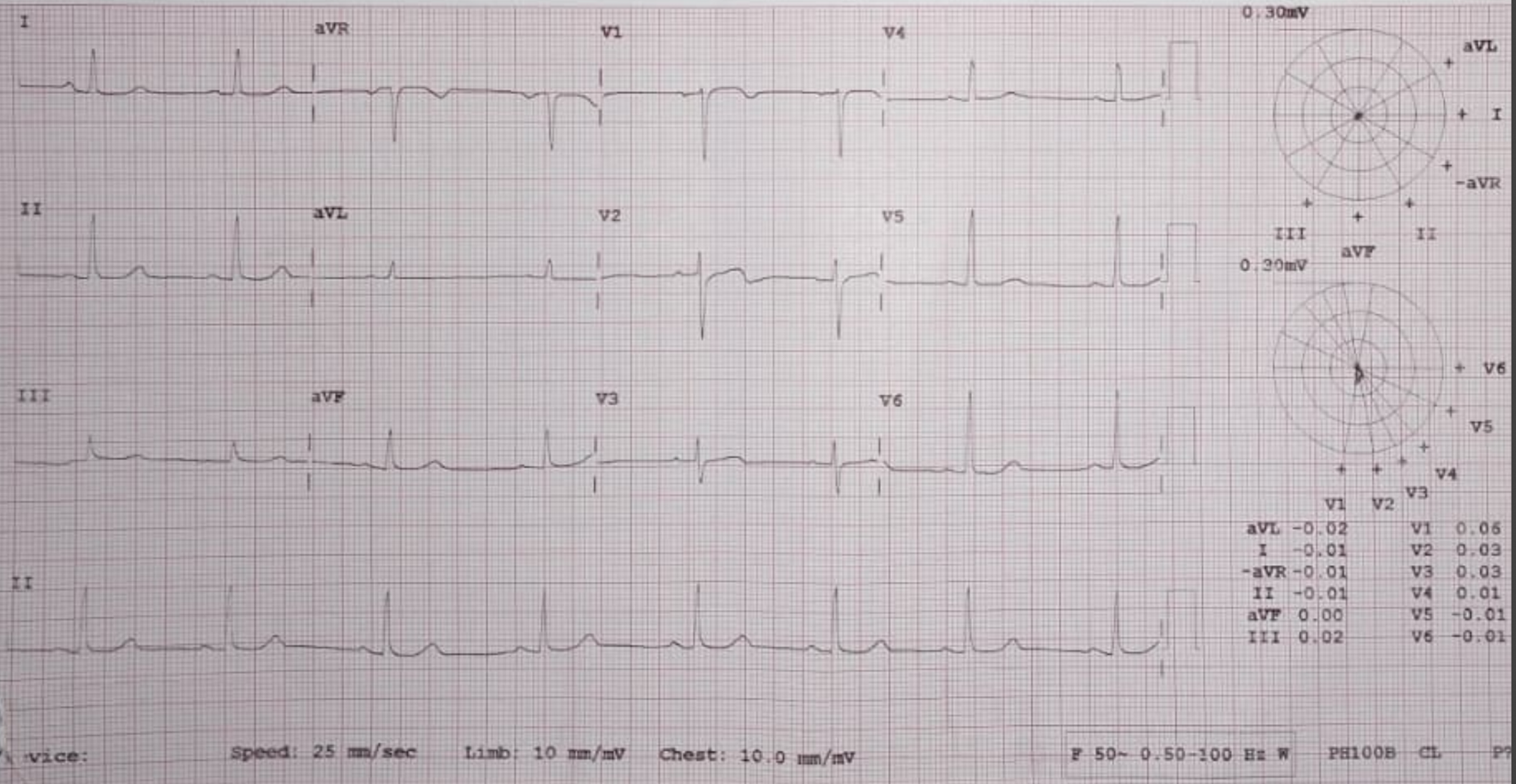
ECG no dynamic ischemic changes. ECHO: LVEF >55%, mild AR. hsTropI 421 pg/mL, creatinine 100 µmol/L.
Relevant Catheterization Findings
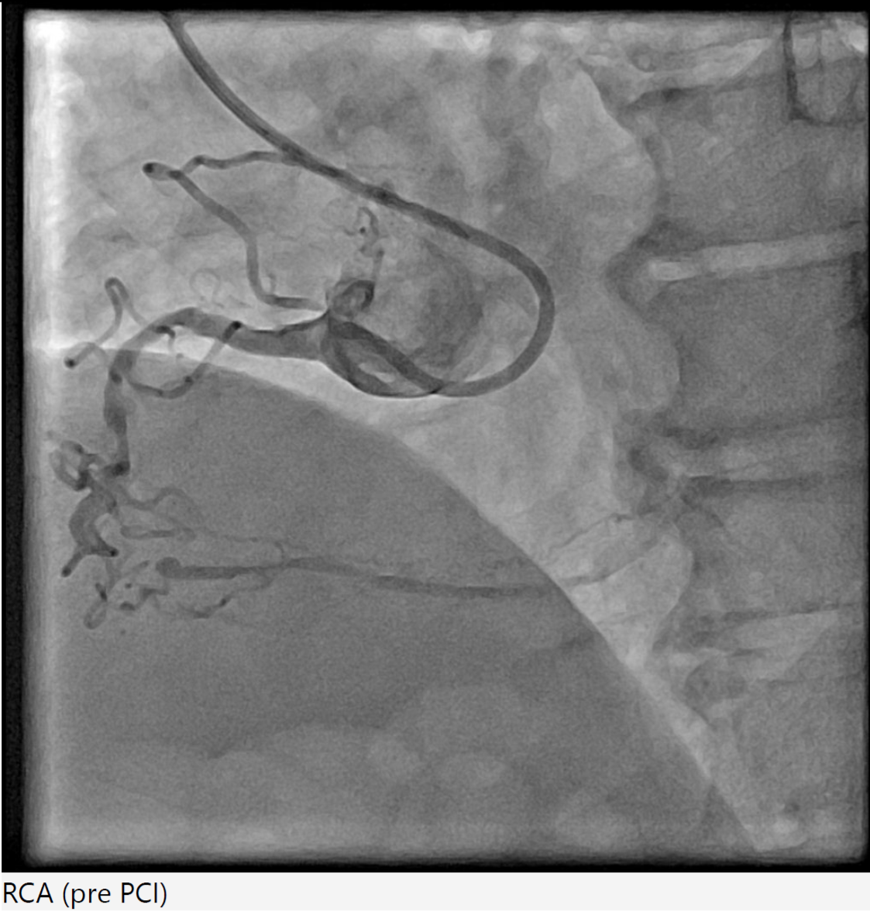
Coronary angiography revealed triple-vessel disease with distal left main involvement, 80% ostial LAD stenosis, 99% ostial LCx stenosis, and a chronic total occlusion of the mid RCA supplied by septal-septal collaterals from the LAD.
Interventional Management
Procedural Step
Right radial 6Fr JR 4.0 initially for antegrade RCA CTO attempt, subsequent switched to AL 1.0 for better support. CTO lesion crossed using Gaia Next 3 wire with Finecross microcatheter support, pre-dilatation using SC Sapphire 1.0 × 8 mm balloon. However, guide catheter induced aorto-ostial dissection (Dunning Class II) occurred during catheter manipulation and contrast injection. The dissection was promptly recognized and proceed strategy of seal the dissection via ping pong technique. Second access via right femoral 6Fr long sheath due to tortuous iliac artery with JR 4.0, Sion Blue wire crossed to distal RCA. The ostial-proximal lesion is predilated with NC Trek 3.5 × 12 mm balloon, then stented with Biofreedom 3.5 × 24 mm and post dilate with NC Trek 3.5 × 12 mm balloon. The mid to distal RCA lesion is prepared using SC Euphora 2.0 x 15 mm balloon with AL 0.75 catheter and Telescope guide extension support. Further predilate with Lacrosse Aperta 3.0 x 13 mm and NC Sapphire 3.0 x 10 mm balloon. Distal RCA treated with DCB Essential Pro 3.0 × 40 mm. Proximal to distal RCA stented with Biofreedom 3.5 × 24 mm and Biofreedom 3.5 × 36 mm (overlapping from ostial to distal). Final post-dilatation with NC Trek 3.75 × 8 mm (mid–distal) and NC Sapphire 4.5 × 8 mm (proximal). Final IVUS guidance via AL 0.75 guiding catheter and Telescope guide extension showed good result without hemodynamic compromise. Total contrast 240 mL, fluoroscopy 132 mins.



 mov-series-002 road map RCA.wmv
mov-series-002 road map RCA.wmv
mov-series-018 aorto ostial RCA dissection.wmv
mov-series-105 final RCA.wmv
Case Summary
This case highlights a rare but significant complication of catheter-induced RCA aorto-ostial dissection during PCI for chronic total occlusion. RCA CTO lesions pose technical challenges due to heavy calcification, tortuous course, and limited guide support. In this case, deep seating of the guiding catheter during contrast injection likely precipitated an aorto-ostial tear. Timely recognition and immediate sealing with overlapping DES — guided by IVUS — prevented progression into the ascending aorta and avoided emergent surgical conversion.