Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_052
Overcoming Guide Support Failure: LAD Rotablation via Right Femoral Access in Challenging Aortic Anatomy
By Sharimila Shanmugam
Presenter
Sharimila Shanmugam
Authors
Sharimila Shanmugam1
Affiliation
National Heart Institute, Malaysia1
View Study Report
CASE20251114_052
Coronary - Complex PCI - Calcified Lesion
Overcoming Guide Support Failure: LAD Rotablation via Right Femoral Access in Challenging Aortic Anatomy
Sharimila Shanmugam1
National Heart Institute, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
61 year old male with underlying dyslipidemia poor adherents to statin. He presents with chest pain on exertion and NYHA class II.He underwent CT coronaries that showed severe stenosis in the LAD with severe calcification.
Relevant Test Results Prior to Catheterization
Hbaic 5.4% LDL 1.4mmol/l
Relevant Catheterization Findings
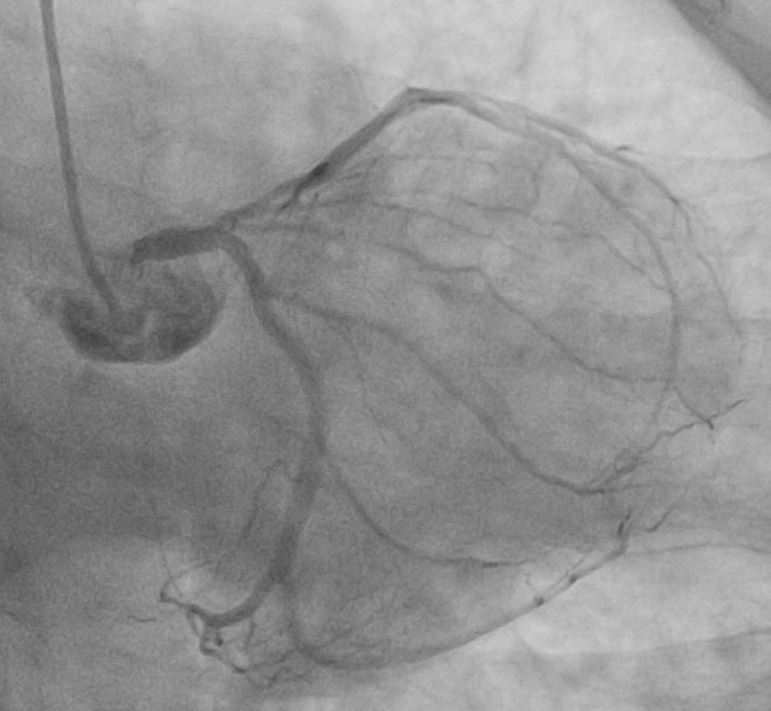
Coronary angiogram shows severe disease ostio-proximal LAD with severe calcification/calcium nodule , mild disease left circumflexsevere stenosis proximal and mid RCA -recessive

 angio3.avi
angio3.avi
angio4.avi
angio5.avi
Interventional Management
Procedural Step
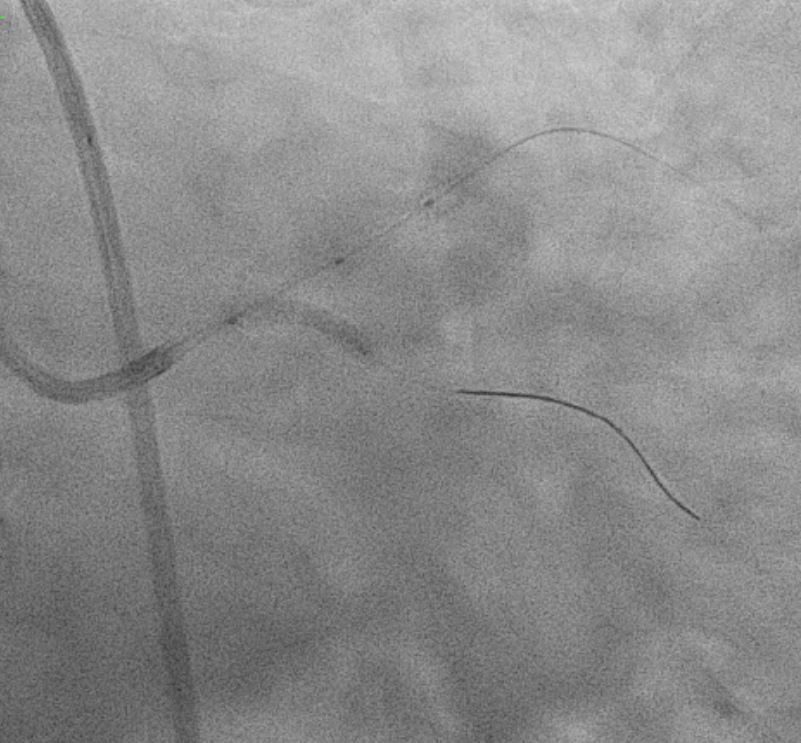
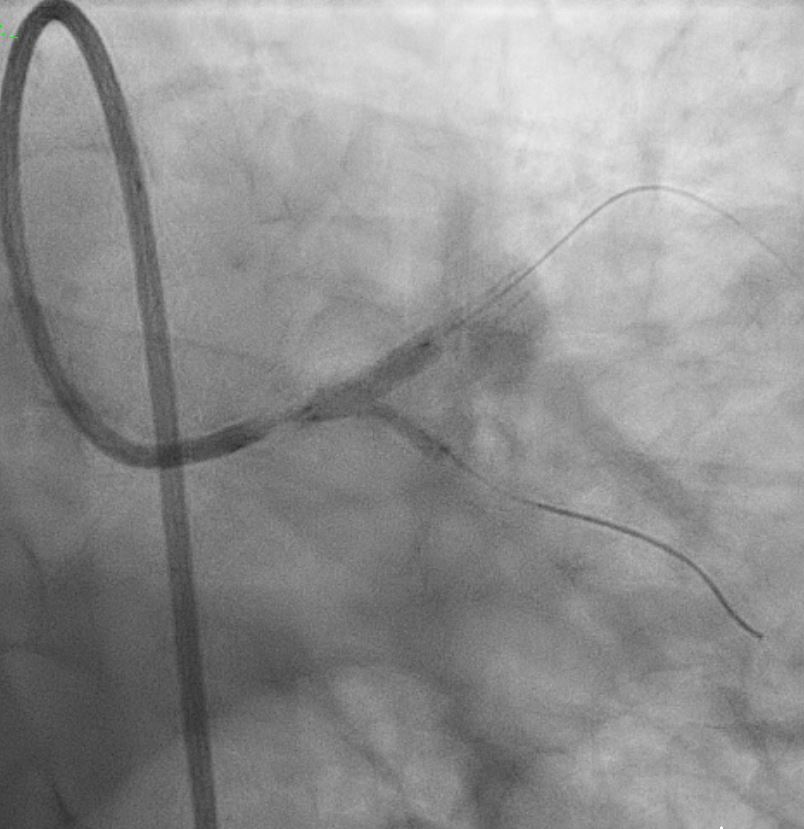
Right Radial approach, Slender 6/7Fr , EBU 3.5 7FR changedto EBU 3.0 7FR Sion blue to LCX, Run-through floppy to LAD IVUS run to LAD Fibro calcified lesion ostial LAD - calcium arc 180 degrees with calcium nodule, ostial LAD 3.48mm2 , tightest proximal LAD 2.31mm2 distallumen size 3.0mm and proximal 3.5mm and ostial 4.0mm ostial LM MLA 10.8mm Used microcatheter fine cross to LAD , Exchange with balloon trapping withRotaWireRotablator 1.5burr introduced- 2 runs high speed 180kph and2 runs at 80kph IVUS done post Rotablator - tightest proximal LAD 2.31mm2 -->3.22mm2 , ostial LAD 3.48mm2 -->4.51mm2 Guiding catheter slipped out and lost the system, tried to reengage but challenging thus decided to change to right femoral puncture to use EBU3.5/7fr ,post dilate LM-LAD NC 4.0/12mm 6atmOstial LCX pinched - decided for Kissing balloon inflation and DCB LCX ostium IVUS done stent well opposed, Ostial LAD MSA 8.25mm2Proximal MSA 5.64mm2

ar2.avi
ar6.avi
ar1.avi
Case Summary
In summary, this was a complex PCI for a severely fibro-calcified ostial and proximal LAD lesion with significant calcium arc and a calcium nodule confirmed on IVUS. Despite initial right radial access with a Slender 6/7 Fr system, guide support with EBU 3.5 and later EBU 3.0 remained suboptimal, ultimately necessitating conversion to a right femoral 7 Fr approach for adequate support. Overall, the case highlights the importance of adaptive access strategy, aggressive plaque modification, IVUS-guided optimization, and bifurcation management to achieve an excellent final physiological and angiographic result in a heavily calcified LM–LAD lesion.