Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_050
When the Guide Catheter Goes Too Deep: A Case of Procedural Stent Crush
By Mochamad Faisal Adam Adam, Fadhli Ramadhan
Presenter
Mochamad Faisal Adam Adam
Authors
Mochamad Faisal Adam Adam1, Fadhli Ramadhan1
Affiliation
Cardiology and Vascular Medicine Department, General Hospital Fatmawati, Jakarta, Indonesia1
View Study Report
CASE20251114_050
Coronary - Complication Management
When the Guide Catheter Goes Too Deep: A Case of Procedural Stent Crush
Mochamad Faisal Adam Adam1, Fadhli Ramadhan1
Cardiology and Vascular Medicine Department, General Hospital Fatmawati, Jakarta, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
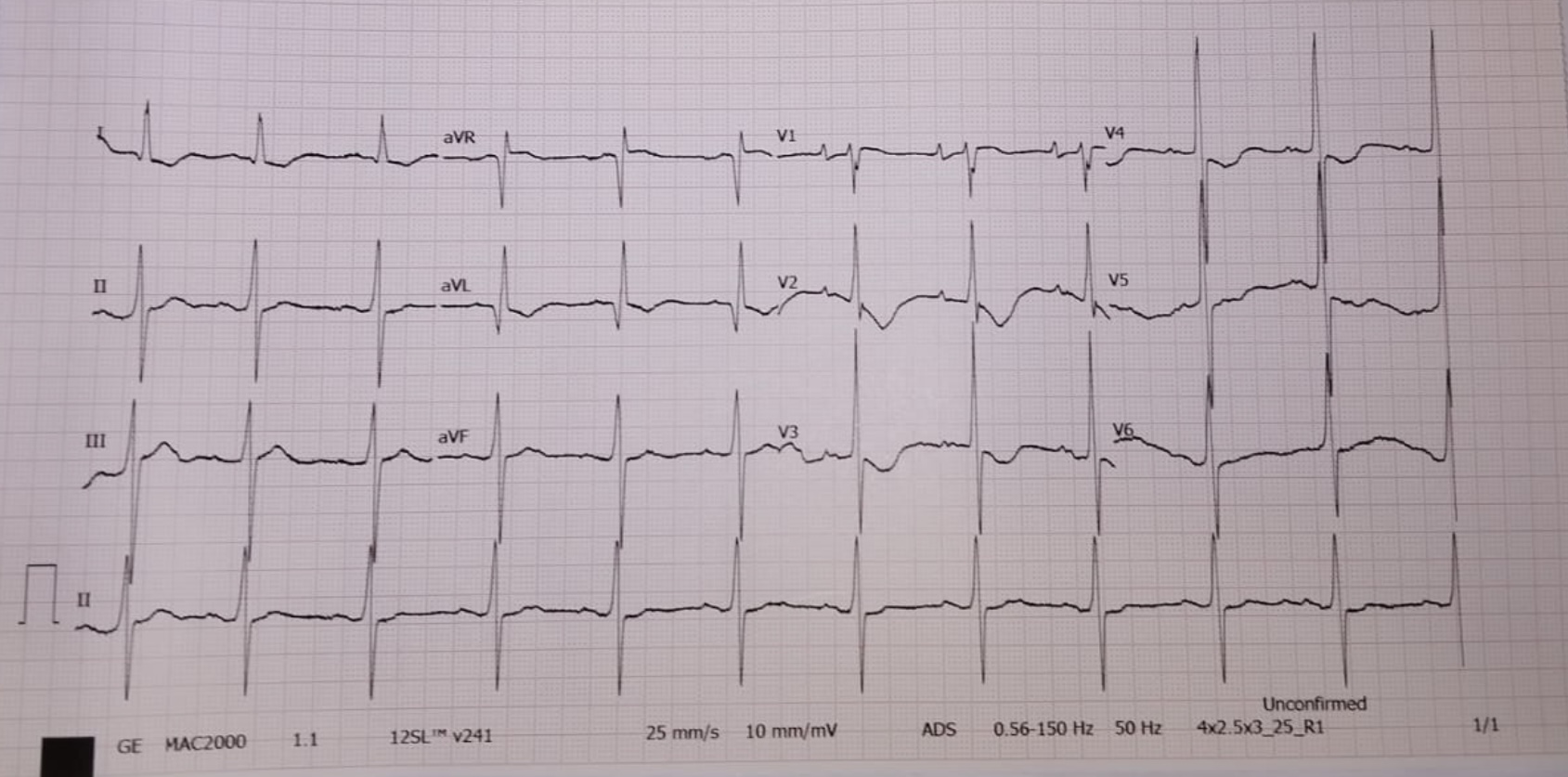
A 78-year-old woman presented to our emergency department with dyspnea on exertion and new-onset chest pain. She had a history of hypertension. Her hemodynamics were initially stable except for elevated blood pressure (156/76 mmHg), and physical examination was unremarkable. Electrocardiography (ECG) showed sinus rhythm with T-wave inversion in leads V2–V5 wtih ST segment depression.
Relevant Test Results Prior to Catheterization
Chest X-ray revealed cardiomegaly with no sign of pulmonary oedema. Other laboratory results were within normal limits, except for a high-sensitivity troponin-I level of 221 ng/mL. The patient was diagnosed with a non–ST-segment elevation myocardial infarction (NSTEMI), and early percutaneous coronary intervention (PCI) was planned.

Relevant Catheterization Findings
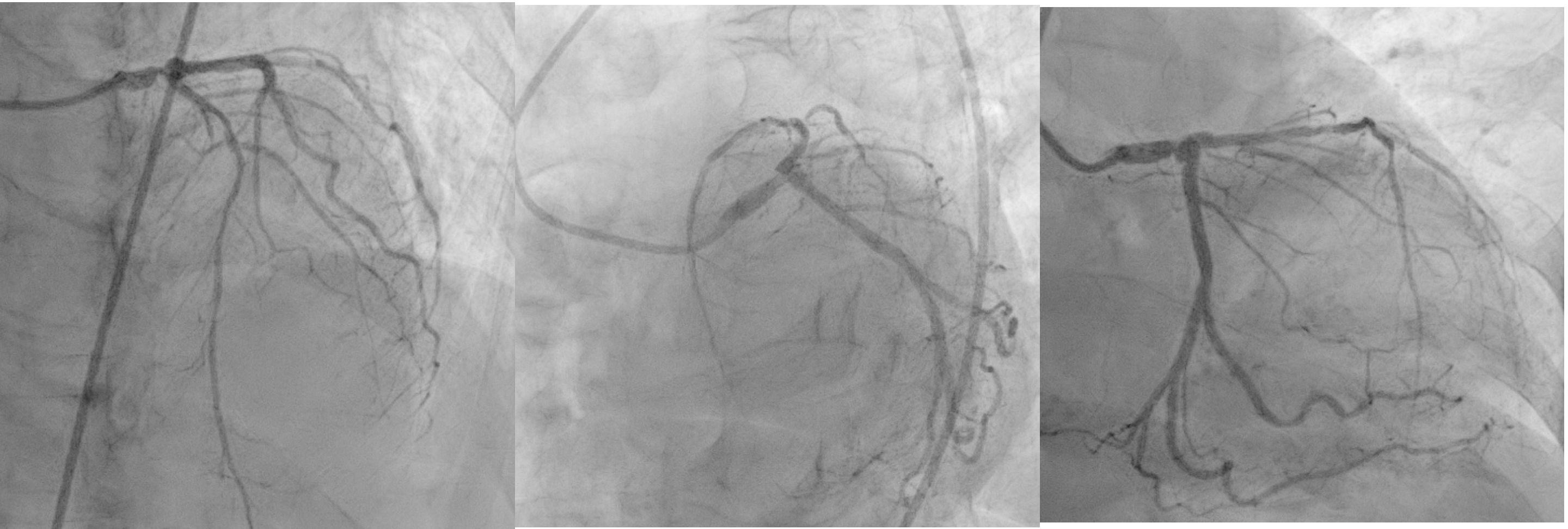
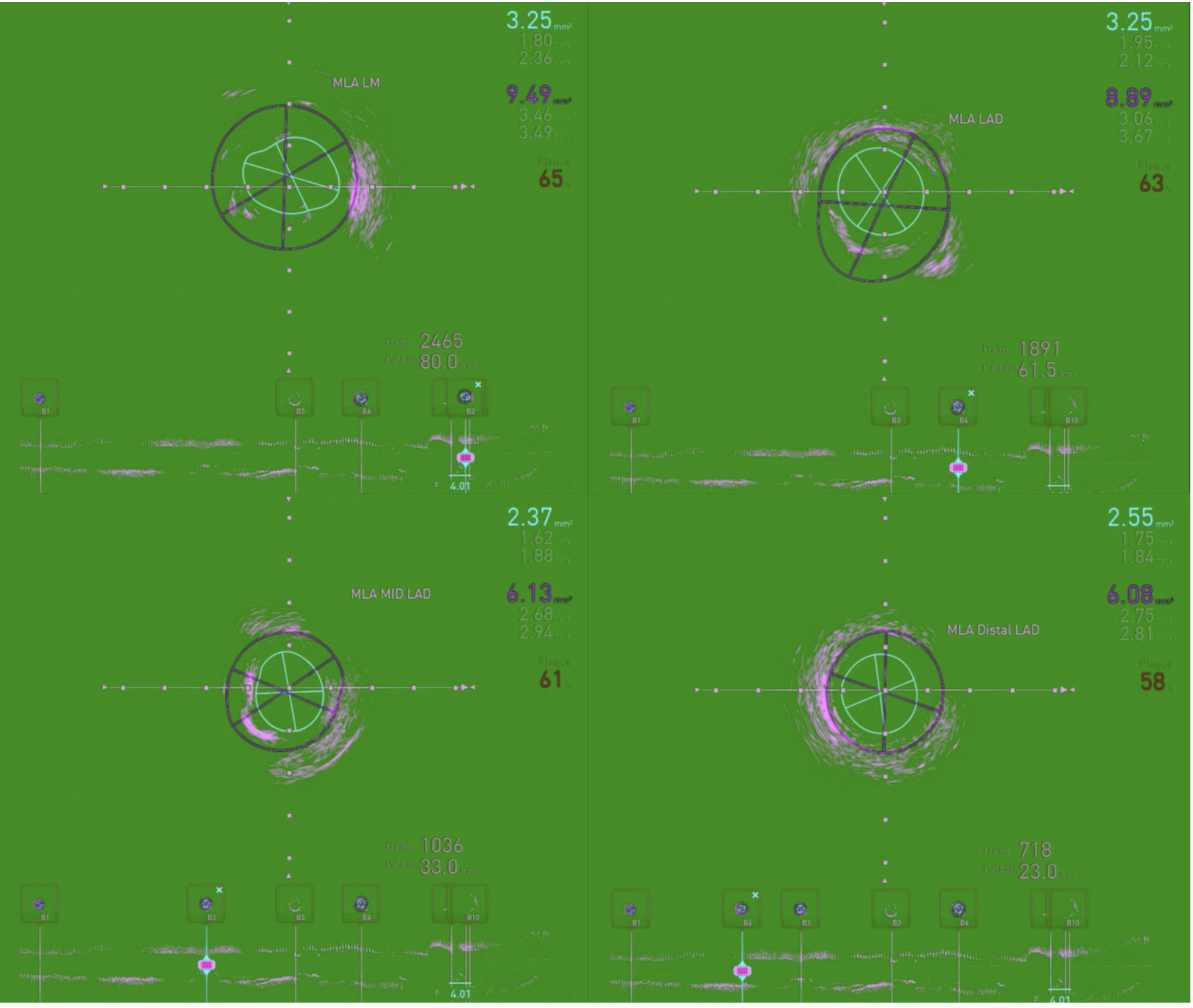
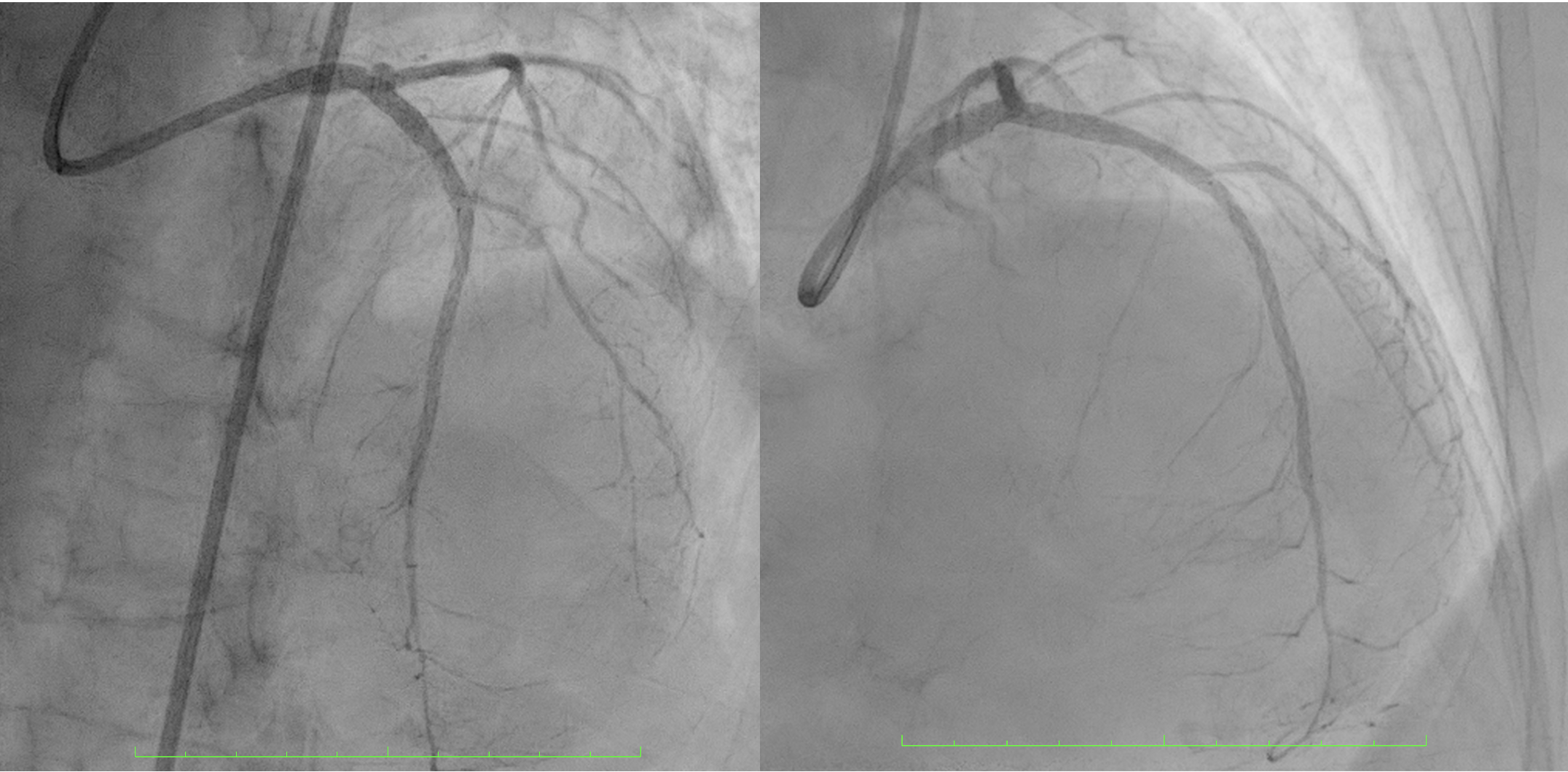
Angiography showed 80% stenosis in the distal LM, with diffuse disease in LAD and a maximum 85% stenosis in the mid-LAD. There was a moderately calcified lesion extending from the distal LM to the proximal LAD. The LCx was normal, and the RCA had a 50% ostial stenosis. An IVUS catheter was advanced over a floppy wire showed a 270° calcified arc, 4 mm in length from the distal LM to the ostial LAD. The MLA of LM, osteal LAD and distal LAD consecutively was 3.25 mm², 3.2 mm² and 2.37 mm²

 1. video LAO cranial .mp4
1. video LAO cranial .mp4
2. RCA video.mp4
IVUS2IVUS_2_2.mp4
Interventional Management
Procedural Step
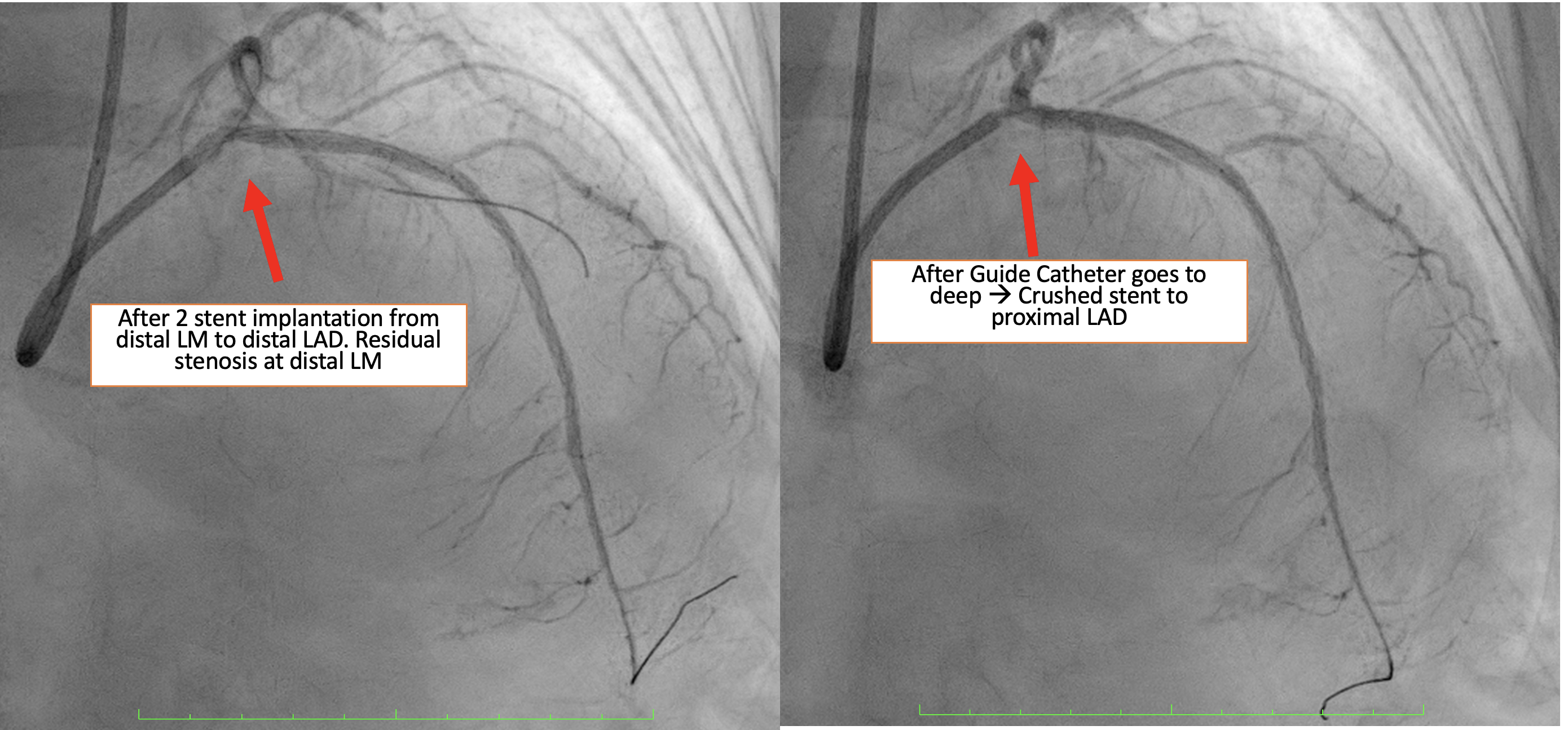
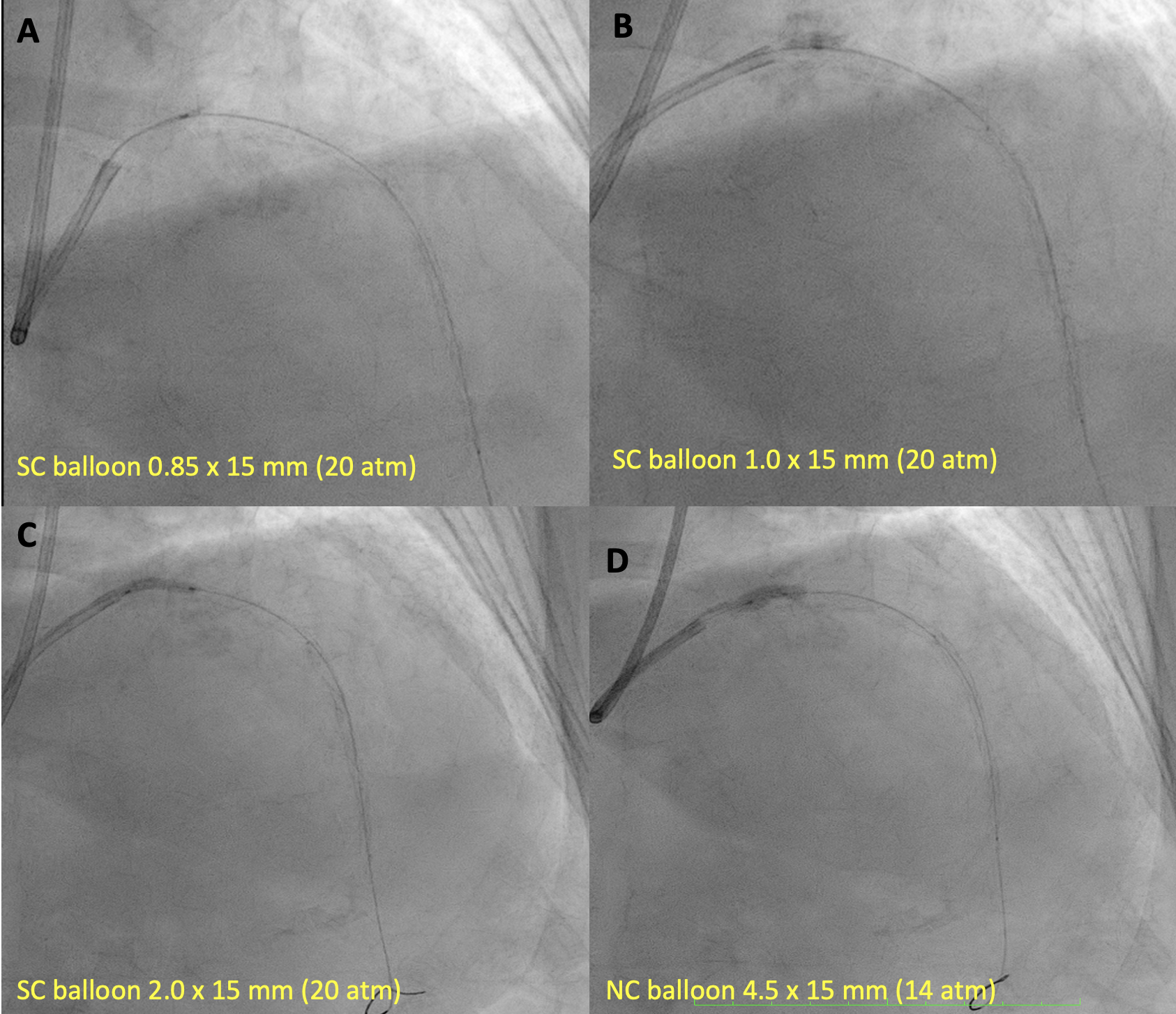
Based on angiographic and IVUS findings, the lesion was prepared using a scoring non-compliant (NC) balloon (ScoreFlex) 2.5 mm × 15 mm, inflated from the distal LAD to distal LM at a maximum of 18 atm. A first drug-eluting stent (DES) Cre8 2.75 mm × 46 mm was deployed from the proximal to distal LAD, followed by a second DES (Combo Plus) 3.5 mm× 38 mm from the distal LM to the proximal LAD with overlap. During withdrawal of the stent balloon, the guiding catheter (XB 3.5/ 7 Fr) advanced too deeply, resulting in crushing of the proximal portion of the Combo Plus stent. Angiography showed that the crushed stent no longer adequately covered the distal LM lesion. Attempts were made to reopen the crushed segment using a series of semi-compliant balloons (Sapphire II Pro): 0.85 mm × 15 mm, 1.0 mm × 15 mm, and 2.0 mm × 15 mm, each inflated to a maximum 20 atm. A non-compliant (NC) balloon 4.5 mm × 8 mm was then used to dilate the stent struts. A third DES (Ultimaster Tansei) 3.5 x 24 mm was deployed from the ostial LM to the proximal LAD, overlapping the previously crushed stent. Proximal optimization (POT) was performed in the LM using a 4.5 mm × 8 mm NC balloon inflated to 22 atm. Final angiography showed a satisfactory result with minimal residual stenosis in the distal LM. The final IVUS assessment could not be perfromed due to damage to the IVUS catheter
1. Crushed stent to proximal LAD.mp4
Predilated with NC ballon in crushed stent.mp4
Final angiography.mp4
Case Summary
Careful manipulation of the guiding catheter is essential, especially during balloon withdrawal from complex or calcified lesions. Maintaining wire position within the true stent lumen is crucial for successfully reopening or reconstructing a crushed stent and ensuring optimal procedural outcomes.