Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_047
Cross-Strut Iliocaval Recanalization: Overcoming Stent-Induced IVC Occlusion in Complex Venous Anatomy
By Chang En Lin, Jen-Kuang Lee
Presenter
Chang En Lin
Authors
Chang En Lin1, Jen-Kuang Lee1
Affiliation
National Taiwan University Hospital, Taiwan1
View Study Report
CASE20251114_047
Endovascular - Venous Disease Intervention
Cross-Strut Iliocaval Recanalization: Overcoming Stent-Induced IVC Occlusion in Complex Venous Anatomy
Chang En Lin1, Jen-Kuang Lee1
National Taiwan University Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 84 year-old man with prior left-leg DVT treated by EKOS thrombolysis and iliac-femoral stenting, who had self-discontinued rivaroxaban for 6 months, and with comorbid hypertension, diabetes, CKD stage 3, and dyslipidemia, presented with acute right lower-limb pain, swelling, and erythema limiting ambulation. Vitals: BP 98/49 mmHg, PR 74, RR 18, SpO₂ 96%, BT 36.7 °C. Examination revealed right-leg edema and calf tenderness, concerning for recurrent DVT.
Relevant Test Results Prior to Catheterization
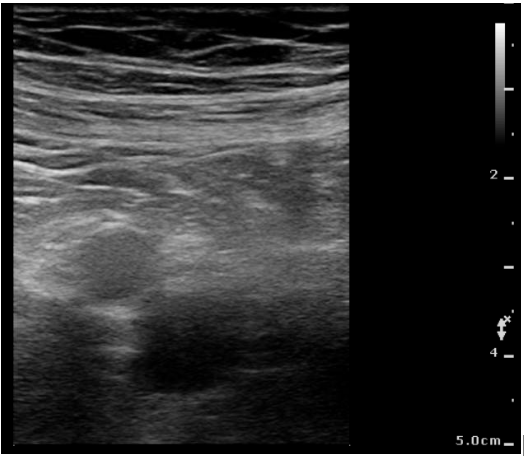
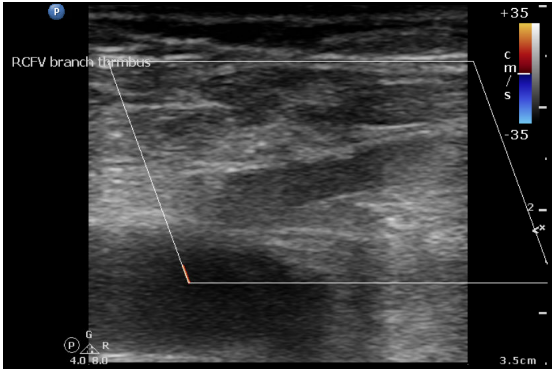
D-dimer was markedly elevated at 5.02 mg/L FEU. Laboratory data showed Hb 11.7 g/dL, PLT 167 K/μL, WBC 6.73 K/μL, and serum creatinine 2.10 mg/dL. Bedside POCUS demonstrated a non-compressible right femoral vein containing a floating thrombus. CT venography was deferred due to renal dysfunction. Right lower limb edema remained controlled under enoxaparin therapy.
Relevant Catheterization Findings
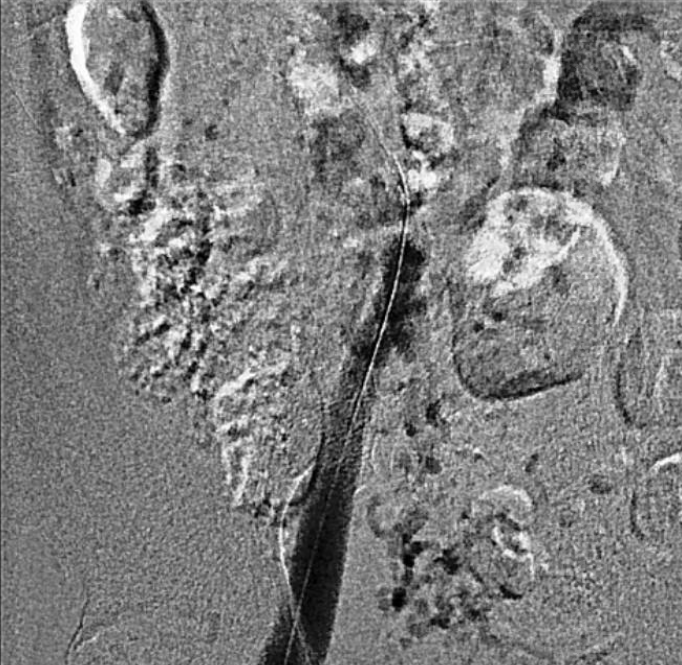
Carbon dioxide venography revealed patent right popliteal and femoral veins, with total occlusion of the right external and common iliac veins with collateral vein from femoral vein to IVC. The left iliac-femoral stent showed no in-stent restenosis but was positioned from the contralateral wall of the IVC, covering the right iliac vein ostium.

Interventional Management
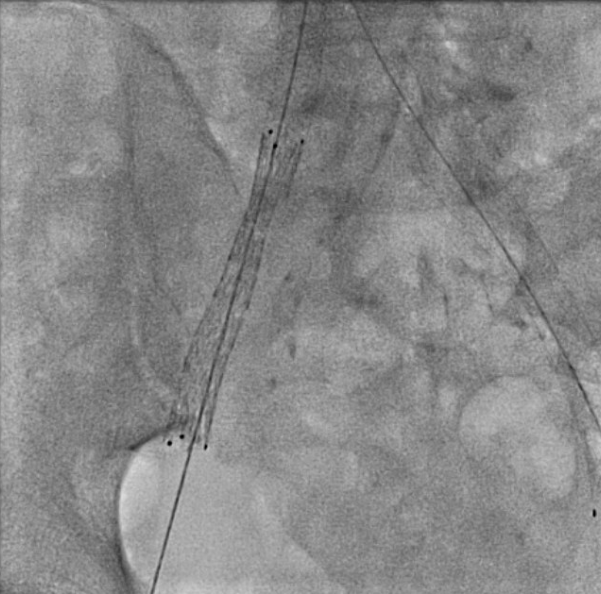
Procedural Step
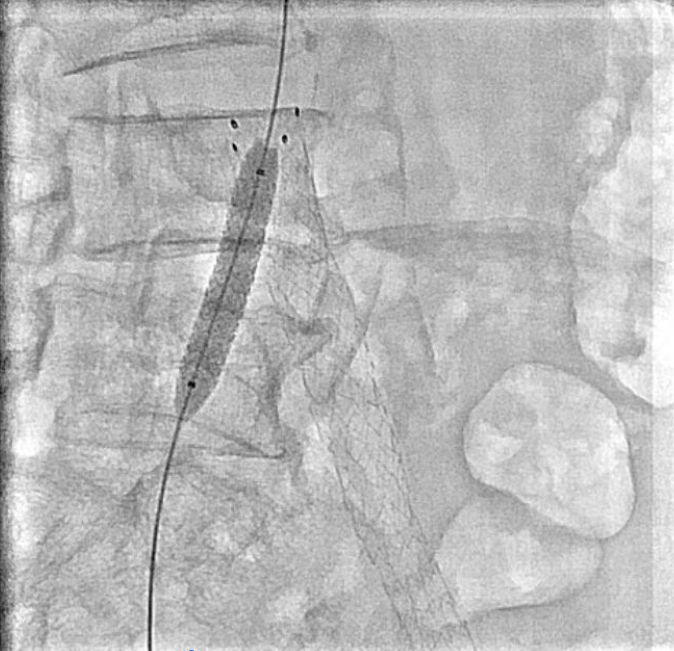
Venography showed occlusion of the right external and common iliac veins with collateral flow; popliteal and femoral veins were patent. A 6F sheath was placed in the right CFV, and a V-18 0.018 wire was advanced to the IVC. Attempts to traverse outside the prior left iliac-femoral stent for double-barrel reconstruction were unsuccessful, as the wire repeatedly entered the existing stent, likely due to complete apposition.The strategy was revised, and wiring into the IVC through a proximal stent strut was achieved. IVUS from the IVC to the RCFV confirmed severe compression at the right CIV ostium and proper wire position. A 10 × 39 mm Abbott Omnilink balloon-expandable stent was deployed at the RCIV ostium and dilated to 10 atm. A kissing-balloon angioplasty was then performed with a 12 × 40 mm Armada balloon from the LCIV and the RCIV balloon inflated simultaneously to 10 atm, restoring bifurcation geometry.A 14 × 60 mm Bard Venovo stent was placed from the RCIV to the REIV and post-dilated with a 12 mm balloon to 10 atm. Final angiography showed widely patent, well-expanded stents with brisk antegrade flow into the IVC and no residual stenosis or thrombosis. Hemostasis was achieved with manual compression, and the procedure concluded without complications.

Case Summary
The patient achieved rapid clinical improvement with resolution of limb edema and remained free of recurrence under oral anticoagulation at follow-up.This experience highlights that in cases where conventional double-barrel iliocaval reconstruction is technically unachievable due to prior stent endothelialization or anatomic limitation, cross-strut recanalization combined with balloon-expandable stent implantation and kissing balloon angioplasty provides a feasible and durable alternative for iliocaval revascularization.