Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_044
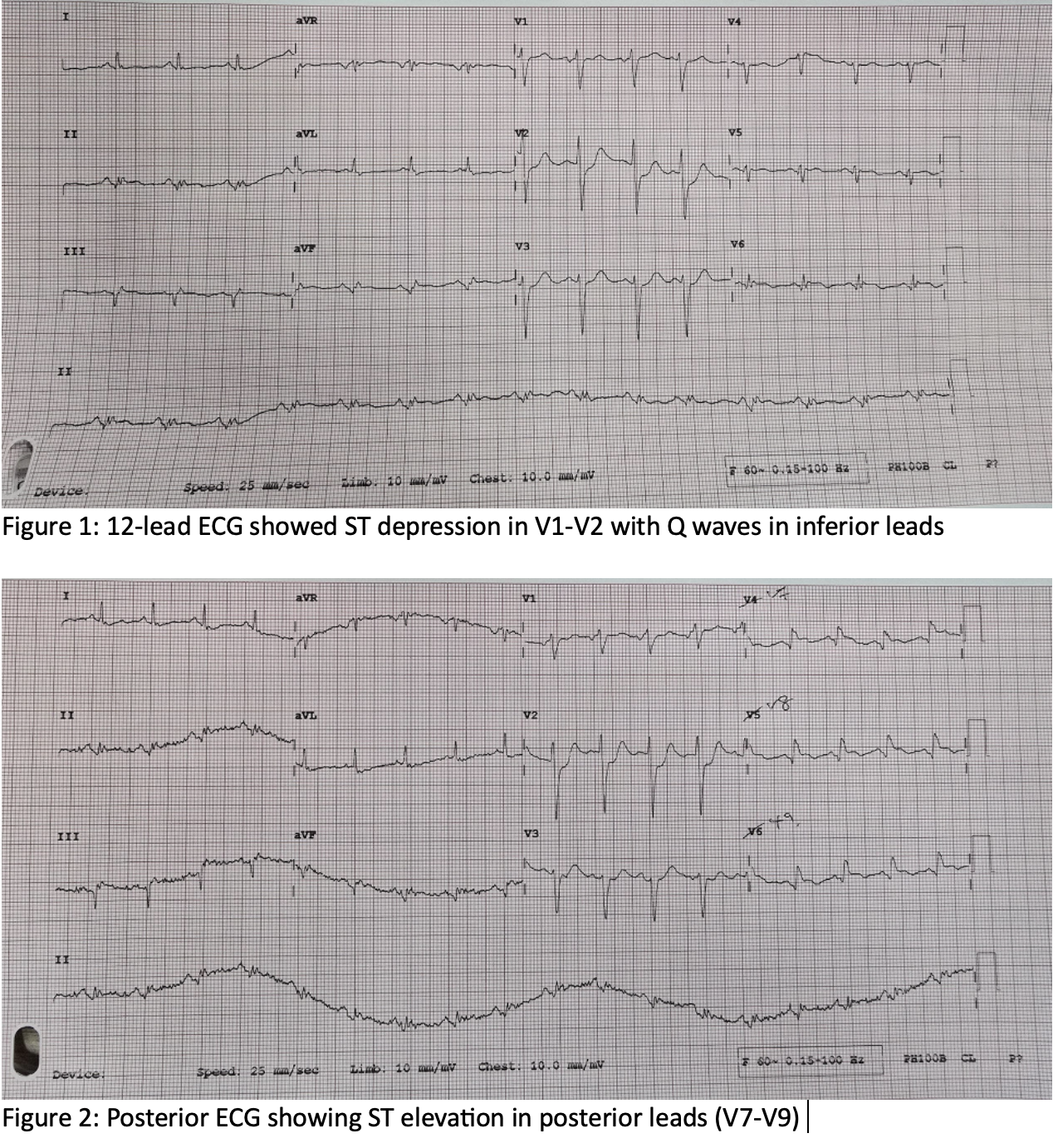
The Silent Culprit: Ramus Intermedius Unmasked as a Cause of Posterior ST-Elevation Myocardial Infarction
By Phang Kok Kit, Doreen Sumpat, Imran Zainal Abidin , Ahmad Syadi Mahmood Zuhdil, Toh Keat Yieng
Presenter
Phang Kok Kit
Authors
Phang Kok Kit1, Doreen Sumpat2, Imran Zainal Abidin 1, Ahmad Syadi Mahmood Zuhdil1, Toh Keat Yieng1
Affiliation
University Malaya Medical Centre, Malaysia1, University Malaysia Sabah, Malaysia2
View Study Report
CASE20251114_044
Coronary - ACS/AMI
The Silent Culprit: Ramus Intermedius Unmasked as a Cause of Posterior ST-Elevation Myocardial Infarction
Phang Kok Kit1, Doreen Sumpat2, Imran Zainal Abidin 1, Ahmad Syadi Mahmood Zuhdil1, Toh Keat Yieng1
University Malaya Medical Centre, Malaysia1, University Malaysia Sabah, Malaysia2
Clinical Information
Relevant Clinical History and Physical Exam
69-year-old gentleman with type 2 diabetes, hypertension and hyperlipidemia, with prior unstable angina and cardiac MRI showing near-transmural basal inferior and anterolateral infarcts, presented after two days of lethargy and fever with new onset chest pain. He was stable with no acute heart failure, but electrocardiogram showed posterior ST elevation with anterior (V1-V2) depression and inferior Q waves, consistent with posterior ST Elevation myocardial infarction (STEMI).
Relevant Test Results Prior to Catheterization
High Sensitivity Troponin I 18136.8 ng/L
Hb 15.5 g/L
WCC 12.3 x 109/L
Relevant Catheterization Findings
Coronary Catheterization findings:
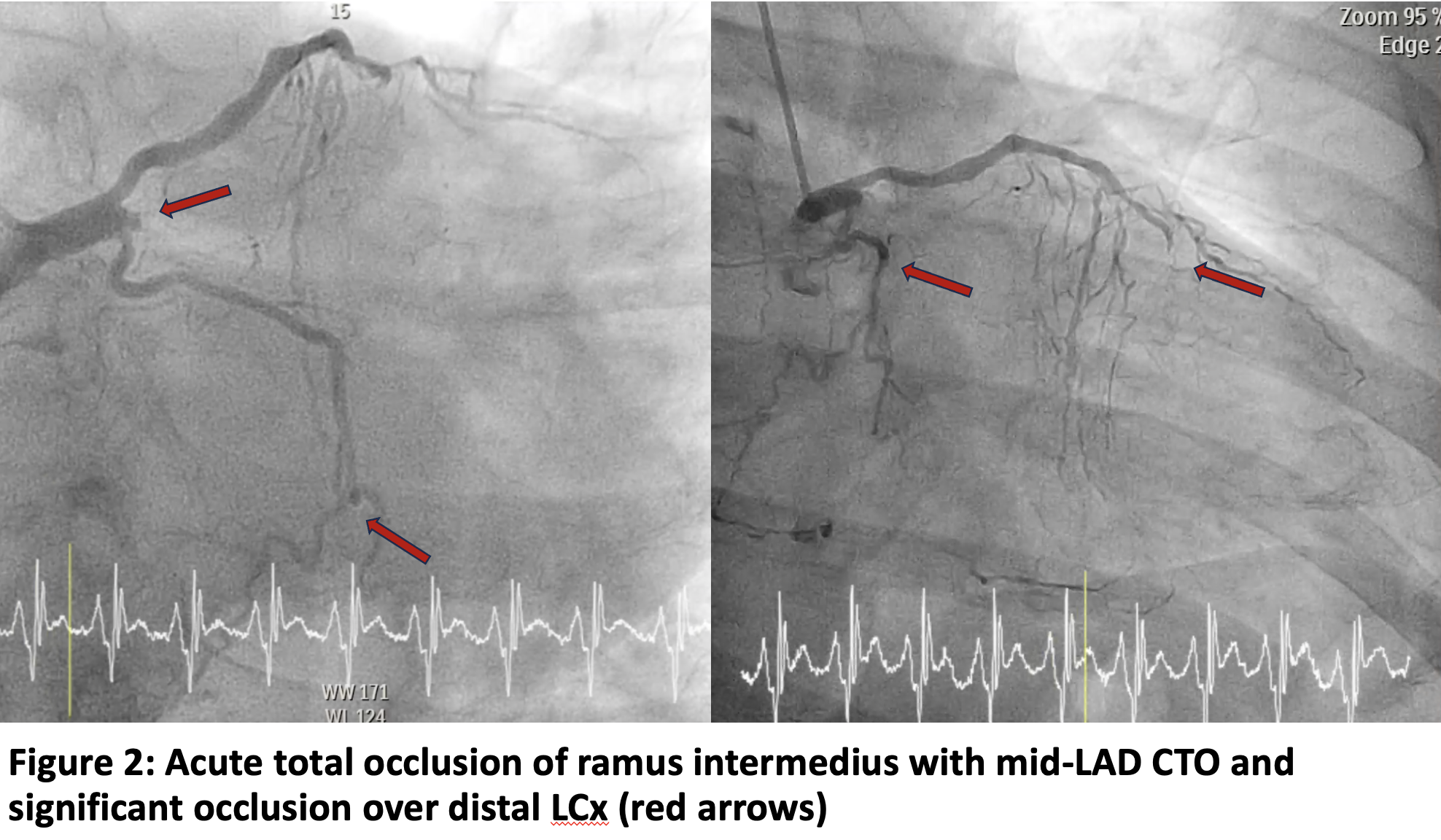
- LM - normal - LAD - mid-LAD chronic total occlusion (CTO)- LCx - Non-dominant with distal CTO- RCA - Dominant with ostial CTO- Ramus intermedius - ostial acute total occlusion (ATO)
 NK LAO CAU 4.mp4
NK LAO CAU 4.mp4
NK RAO CAU LAO CAU 1.mp4
NK RAO CRA 3.mp4
- LM - normal - LAD - mid-LAD chronic total occlusion (CTO)- LCx - Non-dominant with distal CTO- RCA - Dominant with ostial CTO- Ramus intermedius - ostial acute total occlusion (ATO)
Interventional Management
Procedural Step
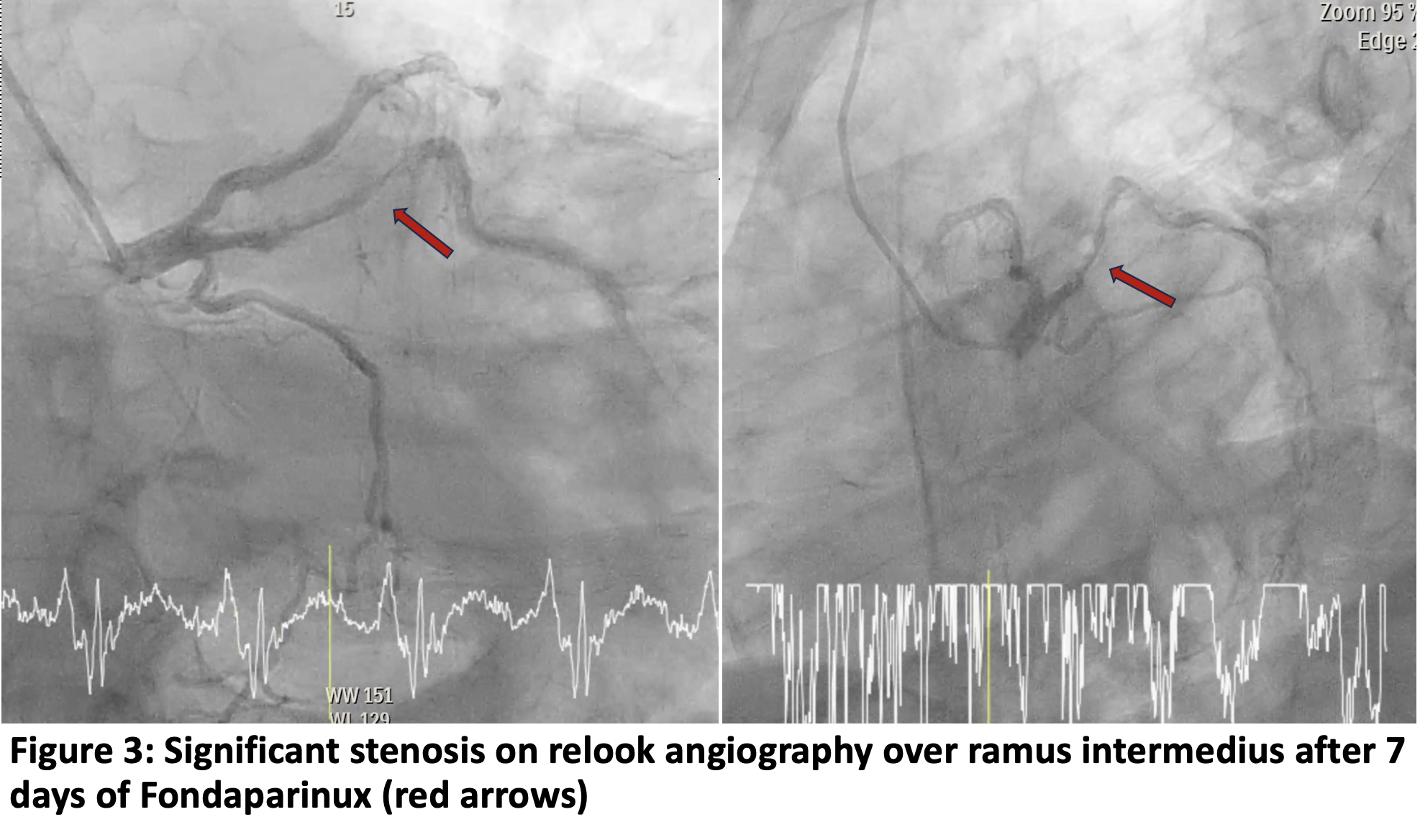
Coronary angiography of the left and right coronary arteries was performed via right radial artery using a 5 Fr Tiger catheter in multiplane views. Primary PCI to the ramus intermedius was attempted with a 6 Fr XB 3.0 guider with side hole and a Runthrough wire. The lesion could not be crossed, so the wire was exchanged with Fielder XT, which successfully crossed without perforation. Pre-dilatation with a MINI TREK 2.0 x 15mm non-compliant (NC) balloon at 14-16 atm. Thrombus aspiration was performed with a THROMBUSTER 6 Fr catheter retrieved white and red intracoronary thrombi, but TIMI flow remained 1. Additional NC balloon dilatation was done with a MINI TREK 2.5 x 15mm (proximal 10 atm, distal 4 atm). Repeat aspiration was done using GUIDEPLUS guide extension achieving TIMI 3 flow with no dissection and perforation. Patient remained stable and was transferred to the coronary care unit for monitoring and seven days of Fondaparinux with dual antiplatelet therapy.
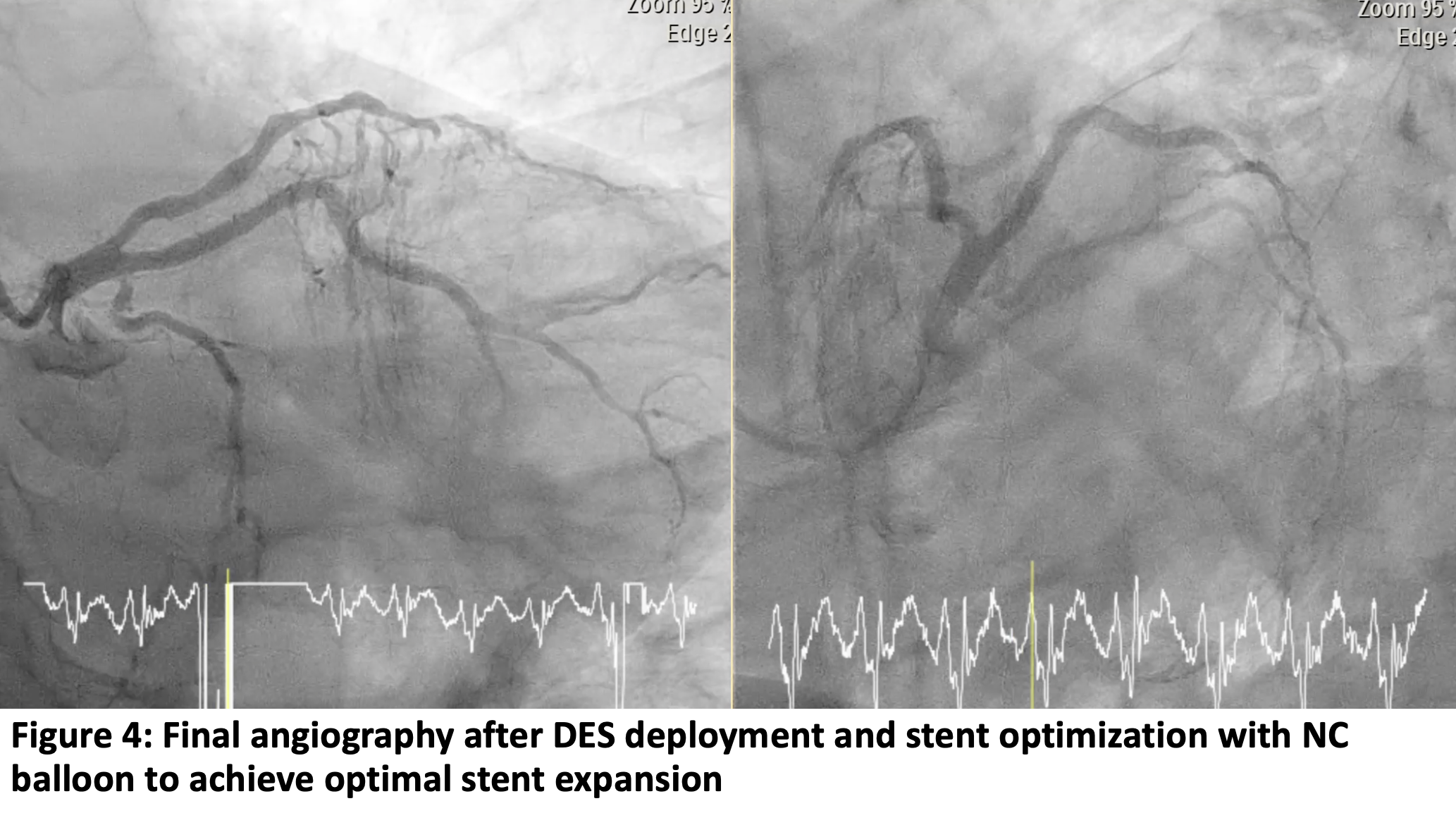
A relook coronary angiography was performed after seven days, followed by ad hoc PCI. A Runthrough wire was advanced via a 6 Fr XB 3.0 guider with side hole. Sequential pre-dilatation with NC Euphora 2.5 x 15mm balloon (8-12 atm) showed minimal recoil and no dissection. A drug-eluting stent (SMT Supraflex Cruz 3.0 x 48mm) was deployed from the ostial to mid ramus at nominal pressure, followed by post diltation with NC Sapphire 3.0 x 10mm at 24 atm. Final angiography: TIMI 3 flow, good expansion, no dissection.
NK2 RAO CAU LAO CAU Final Angio .mp4
NK2 LAO CAU Angio 3.mp4
NK2 RAO CAU DES 1.mp4
A relook coronary angiography was performed after seven days, followed by ad hoc PCI. A Runthrough wire was advanced via a 6 Fr XB 3.0 guider with side hole. Sequential pre-dilatation with NC Euphora 2.5 x 15mm balloon (8-12 atm) showed minimal recoil and no dissection. A drug-eluting stent (SMT Supraflex Cruz 3.0 x 48mm) was deployed from the ostial to mid ramus at nominal pressure, followed by post diltation with NC Sapphire 3.0 x 10mm at 24 atm. Final angiography: TIMI 3 flow, good expansion, no dissection.
Case Summary
Ramus intermedius occlusion can quietly masquerade as an isolated anterior ST depression concealing a true posterior STEMI. When this uncommon vessel supplies the posterolateral wall, its abrupt closure produces STEMI pattern easily missed without posterior leads. Recognizing this hidden culprit is critical, as early suspicion transforms an ambiguous ECG into a life-saving diagnosis and timely reperfusion.