Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_042
Rescue Intracoronary Streptokinase via Aspiration Catheter After Ventricular Fibrillation in ST-Segment Elevation Myocardial Infarction
By Polpat Euswas
Presenter
Polpat Euswas
Authors
Polpat Euswas1
Affiliation
Hua Hin Hospital, Thailand1
View Study Report
CASE20251114_042
Coronary - ACS/AMI
Rescue Intracoronary Streptokinase via Aspiration Catheter After Ventricular Fibrillation in ST-Segment Elevation Myocardial Infarction
Polpat Euswas1
Hua Hin Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
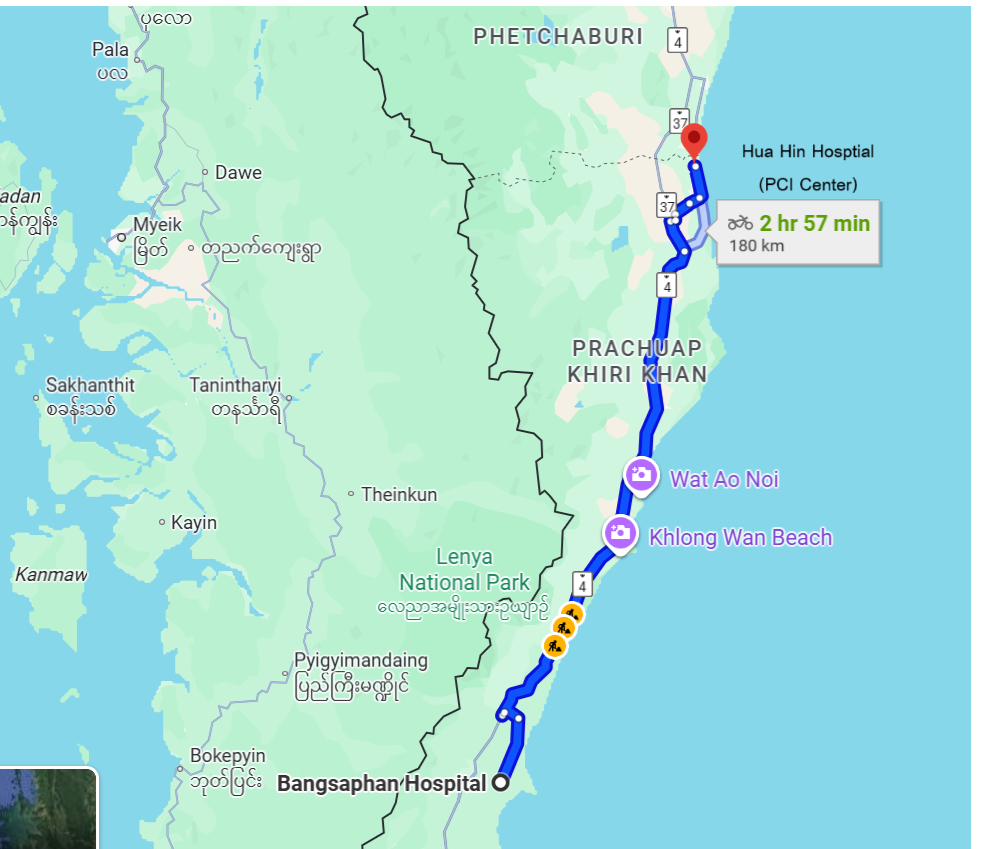
A 56-year-old man with a 40-year history of heavy smoking developed sudden severe central chest pain (10/10) 30 minutes before arriving at a community hospital. On arrival, he was alert with stable vital signs (blood pressure 116/68 mmHg, pulse rate 62 / minutes, respiratory rate 22 / minutes). Physical examination showed no pallor, no jaundice, clear lungs, normal heart sounds, and no peripheral edema.
Relevant Test Results Prior to Catheterization
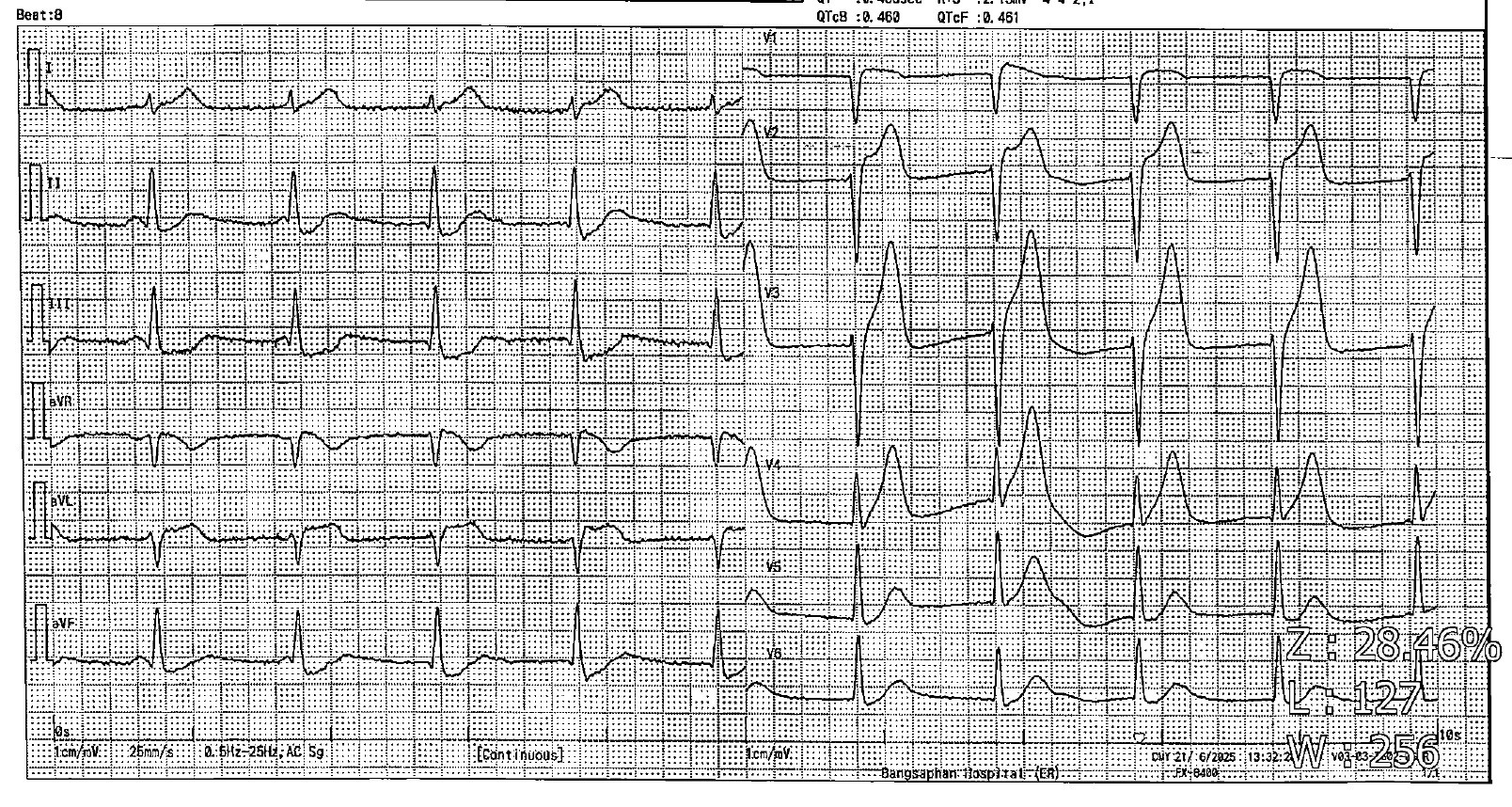
Initial ECG showed sinus rhythm with marked ST-segment elevation in V2–V3 and reciprocal depression in leads II and III. Because the hospital was 180 km from a PCI center (refer time 3 hours), streptokinase (1.5 million units) was initiated. Five minutes after infusion (~250,000 units), the patient developed ventricular fibrillation, successfully defibrillated, intubated, and transferred. CT brain showed no intracranial hemorrhage.
Relevant Catheterization Findings
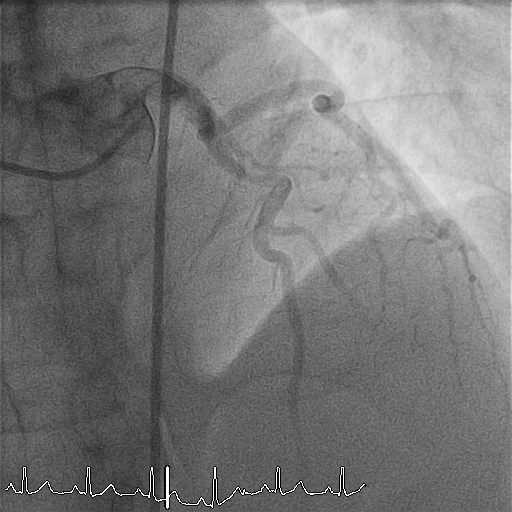
The patient arrived intubated with BP 110/62 mmHg and pulse 60/min. Echocardiography showed an LVEF of 30% with severe anterior wall hypokinesia. Coronary angiography revealed a right-dominant system with normal LMCA, LCX, and RCA (TIMI 3 flow). The proximal LAD demonstrated a subtotal thrombotic occlusion (95–99%) with a large thrombus burden and TIMI 1 flow.

 01.avi
01.avi
02.avi
03.avi
Interventional Management
Procedural Step
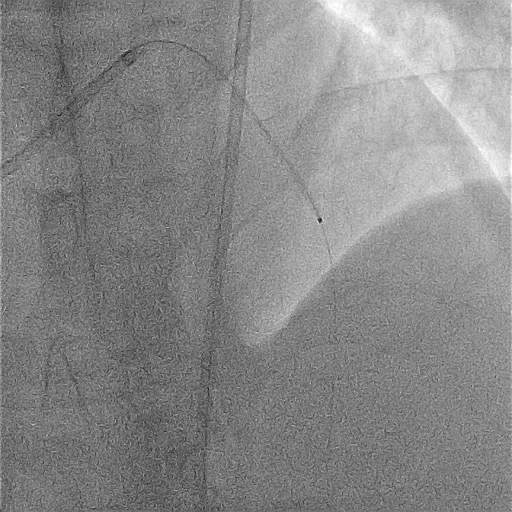
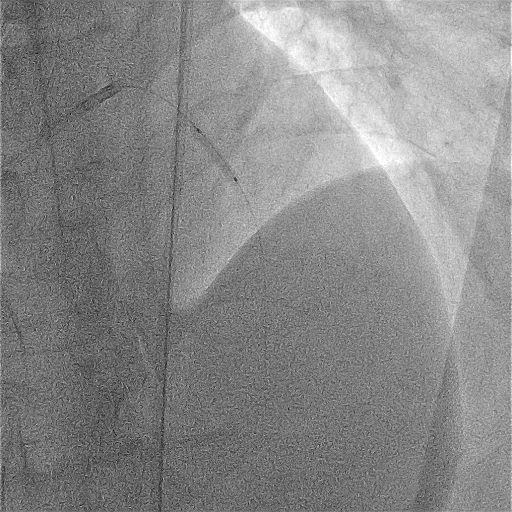
The patient arrived intubated and hemodynamically stable. Right femoral artery access was obtained with a 7 Fr sheath. Diagnostic angiography confirmed subtotal thrombotic occlusion of the proximal LAD with TIMI 1 flow and a large thrombus burden. PCI was initiated using a 7 Fr EBU 3.5 guiding catheter and a Sion guidewire. An ELIMINATE 7 Fr aspiration catheter was advanced, and multiple aspiration passes were performed, but significant residual thrombus persisted with high risk of no-reflow.
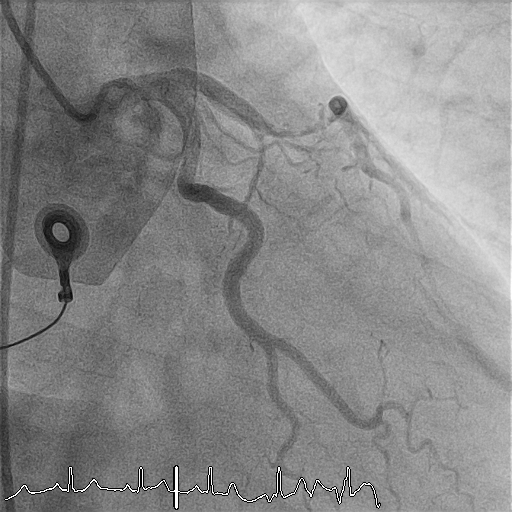
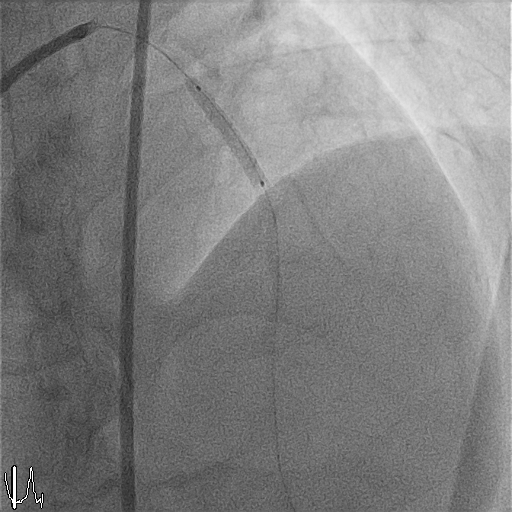
Pre-dilatation was performed with an IKAZUCHI ZERO 2.5 × 15 mm balloon at 9–12 atm. Given the massive thrombus burden and prior incomplete systemic streptokinase infusion, intracoronary streptokinase was administered via the aspiration catheter in 1-mL aliquots (15,000 IU each), slowly over 1–2 minutes per dose, to a total of 150,000 IU. Progressive improvement in thrombus dissolution was observed with restoration of distal flow.Following thrombus resolution, direct stenting of the proximal LAD was performed using a Xience PRO-A 3.0 × 23 mm drug-eluting stent, deployed at 9 atm. Post-dilatation was performed with a CONQUEROR NC 3.0 × 15 mm balloon at 12–20 atm achieving full stent expansion. Final angiography demonstrated TIMI 3 flow with no dissection or residual stenosis.Given reduced LV systolic function, an IABP was inserted via the right femoral artery for hemodynamic support. Total contrast volume was 120 mL, total fluoroscopy time 10.03
12 post balloon, large thrombus.avi
18 IC SK.avi
28 final.avi
Pre-dilatation was performed with an IKAZUCHI ZERO 2.5 × 15 mm balloon at 9–12 atm. Given the massive thrombus burden and prior incomplete systemic streptokinase infusion, intracoronary streptokinase was administered via the aspiration catheter in 1-mL aliquots (15,000 IU each), slowly over 1–2 minutes per dose, to a total of 150,000 IU. Progressive improvement in thrombus dissolution was observed with restoration of distal flow.Following thrombus resolution, direct stenting of the proximal LAD was performed using a Xience PRO-A 3.0 × 23 mm drug-eluting stent, deployed at 9 atm. Post-dilatation was performed with a CONQUEROR NC 3.0 × 15 mm balloon at 12–20 atm achieving full stent expansion. Final angiography demonstrated TIMI 3 flow with no dissection or residual stenosis.Given reduced LV systolic function, an IABP was inserted via the right femoral artery for hemodynamic support. Total contrast volume was 120 mL, total fluoroscopy time 10.03
Case Summary
Catheter-directed intracoronary fibrinolysis represents an innovative extension of contemporary STEMI management, offering targeted thrombus dissolution when large clot burden threatens PCI success. Delivering streptokinase through an aspiration catheter enhances microvascular reperfusion, reduces no-reflow risk, and supports safe stent deployment. This strategy underscores a flexible, globally applicable approach that can elevate reperfusion outcomes, particularly in regions facing delayed access to primary PCI.