Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_041
Overcoming LAD-Diagonal Bifurcation Challenges: IVUS-Assisted Antegrade CTO Recanalization
By Yuyu Lu, Tsai Chuan-Tsai
Presenter
Yuyu Lu
Authors
Yuyu Lu1, Tsai Chuan-Tsai1
Affiliation
Taipei Veteran General Hospital, Taiwan1
View Study Report
CASE20251114_041
Coronary - Complex PCI - CTO
Overcoming LAD-Diagonal Bifurcation Challenges: IVUS-Assisted Antegrade CTO Recanalization
Yuyu Lu1, Tsai Chuan-Tsai1
Taipei Veteran General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
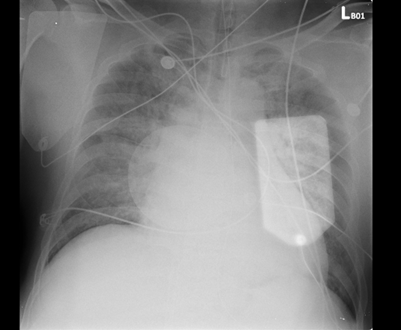
A 60-year-old man with poorly controlled hypertension and a history of cigarette smoking suffered a witnessed out-of-hospital cardiac arrest. The initial rhythm was ventricular fibrillation requiring CPR and multiple defibrillations, with ROSC after ~40 minutes. On arrival, he was intubated and in cardiogenic shock with pulmonary edema. He was stabilized with VA-ECMO, IABP, and mechanical ventilation before coronary angiography.
Relevant Test Results Prior to Catheterization
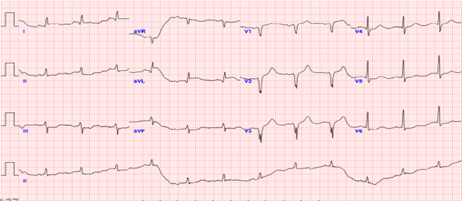
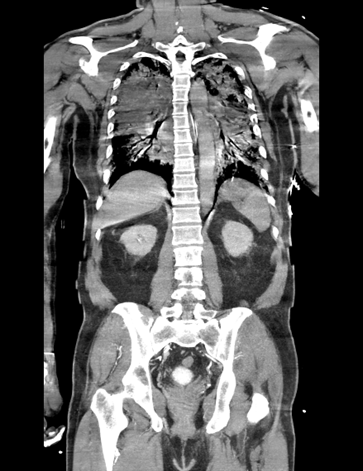
ECG showed sinus rhythm with ST-segment elevation in V1–V3 and aVL, consistent with anterior STEMI. Brain CT excluded intracranial hemorrhage. Chest CT ruled out aortic pathology but revealed diffuse ground-glass opacities suggesting pulmonary edema. Echocardiography showed severe LV dysfunction with EF 18% and diffuse hypokinesis. Cardiac enzymes were markedly elevated.
 AP2C.mp4
AP2C.mp4
AP4C.mp4
PLAX.mp4
Relevant Catheterization Findings
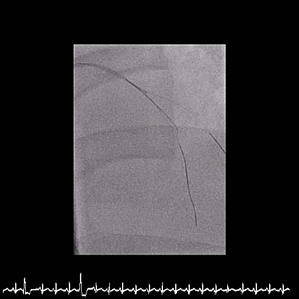
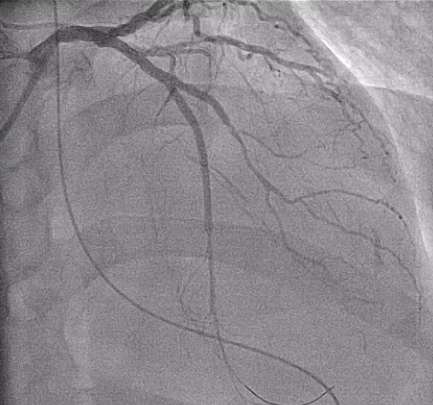
The left main was patent. The LCX had a diffuse long lesion with up to 95% stenosis. The LAD showed a proximal CTO with a blunt stump and well-developed collaterals supplying the distal vessel, giving TIMI 2 flow. The RCA demonstrated TIMI 1 flow with distal critical stenosis, haziness suggesting thrombus, and poor collaterals, identifying it as the culprit for ST elevation and shock.
診斷CAUD.mp4
診斷CRAN.mp4
診斷LAO.mp4
Interventional Management
Procedural Step
Inrefractory VT/VF arrest and cardiogenic shock, emergent culprit RCA PCI wasperformed under VA-ECMO and IABP. A Conquest Pro 12 GW crossed the distal RCACTO after failed attempts with Fielder FC and Gaia 2nd. Sequential POBA wasdone, followed by three BMS from RCA-M to RCA-PL, achieving TIMI 3 flow. Abrief attempt to wire LAD-P CTO with a Fielder XT-R failed, suggesting achronic occlusion, and the procedure was stopped due to instability.
Case Summary
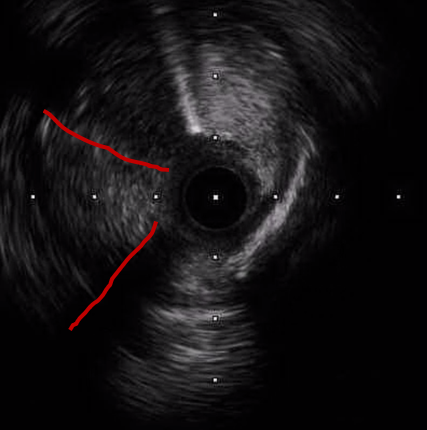
Earlyrecognition of the true culprit vessel in cardiogenic shock enabled timely RCArevascularization and hemodynamic stabilization. Staged LAD CTO PCI wassubsequently performed using an image-assisted strategy, incorporating IVUSinterrogation from both septal and diagonal branches to clarify the complexproximal cap and employing an IVUS-guided parallel-wire technique to achievetrue-lumen crossing. These imaging-directed decisions, combined with meticulousbifurcation optimization, were essential to achieving complete and saferevascularization in this extreme-risk clinical scenario.