Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_036
Calcified Left Main Disease In Patient With Poor LV Function
By Hei Yu Zoe Chu
Presenter
Hei Yu Zoe Chu
Authors
Hei Yu Zoe Chu1
Affiliation
Tuen Mun Hospital, Hong Kong, China1
View Study Report
CASE20251114_036
Coronary - Complex PCI - Calcified Lesion
Calcified Left Main Disease In Patient With Poor LV Function
Hei Yu Zoe Chu1
Tuen Mun Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
This is a 78 year old patient with history of ischaemic stroke, hypertension, diabetes mellitus on insulin injection. He was admitted to our unit for severe pneumonia and NSTEMI. He was intubated for respiratory distress shortly after arrival to hospital, he was haemodynamically unstable requiring Dopamine and Noradrenaline infusion. He was treated with antibiotics and gradually stabilised.

Relevant Test Results Prior to Catheterization
His ECG on admission shows no acute ST changes and no serial changes, and high sensitive Troponin on admission was greater than 50,000ng/L (n</= 34.2). His echo showed ejection fraction of 30% with moderate MR.
Relevant Catheterization Findings
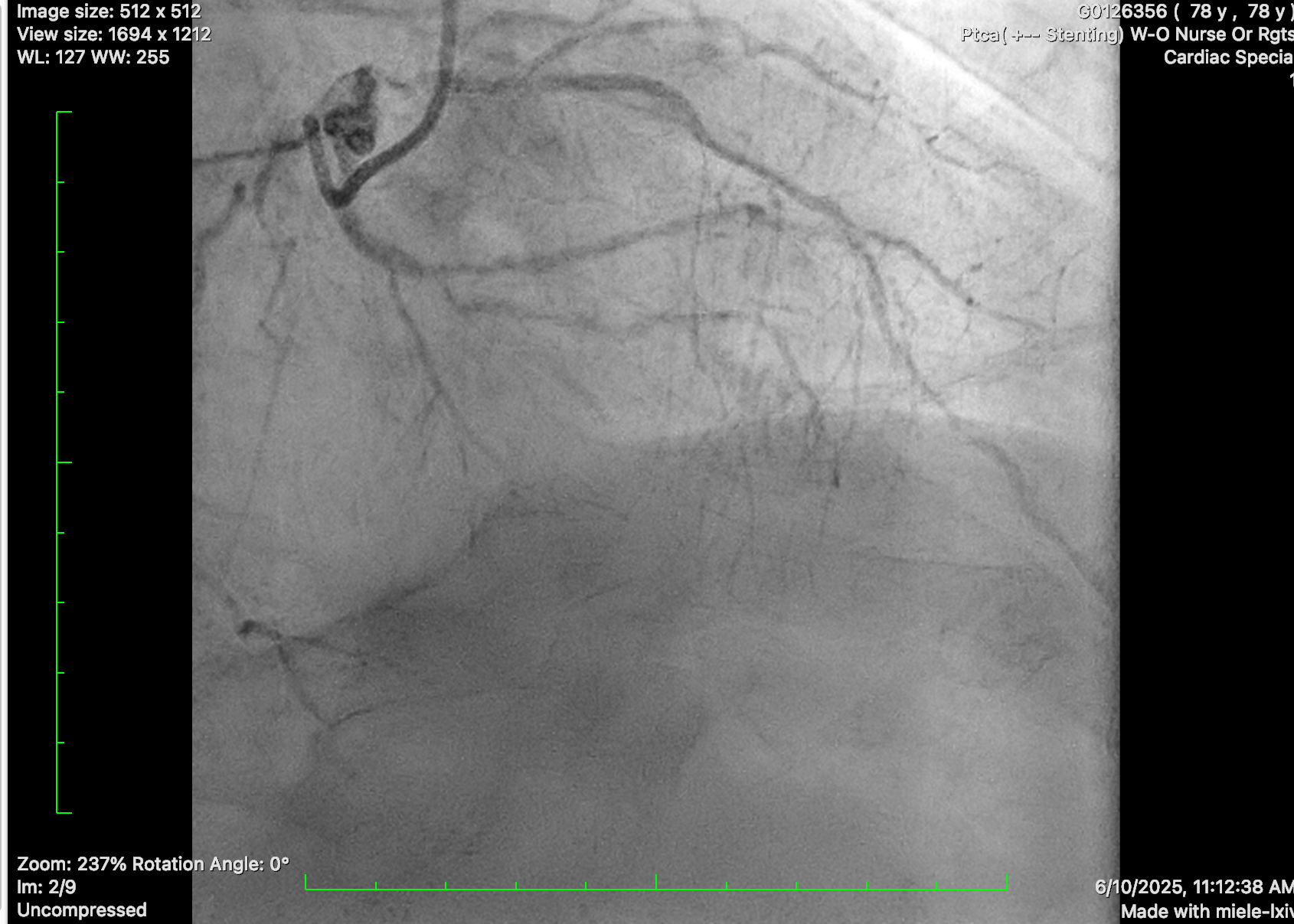
Diagnostic coronary angiogram was performed, showing distal left main disease and ostial LAD subtotal occlusion with antegrade flow, diffuse severe disease over proximal to mid LAD. Mid-LCx showed severe stenosis. RCA was dominant, with mRCA severe disease followed by subtotal occlusion with antegrade collateral to distal RCA and retrograde collateral to septal branches of LAD and diffuse severe disease at PL branch.
Interventional Management
Procedural Step
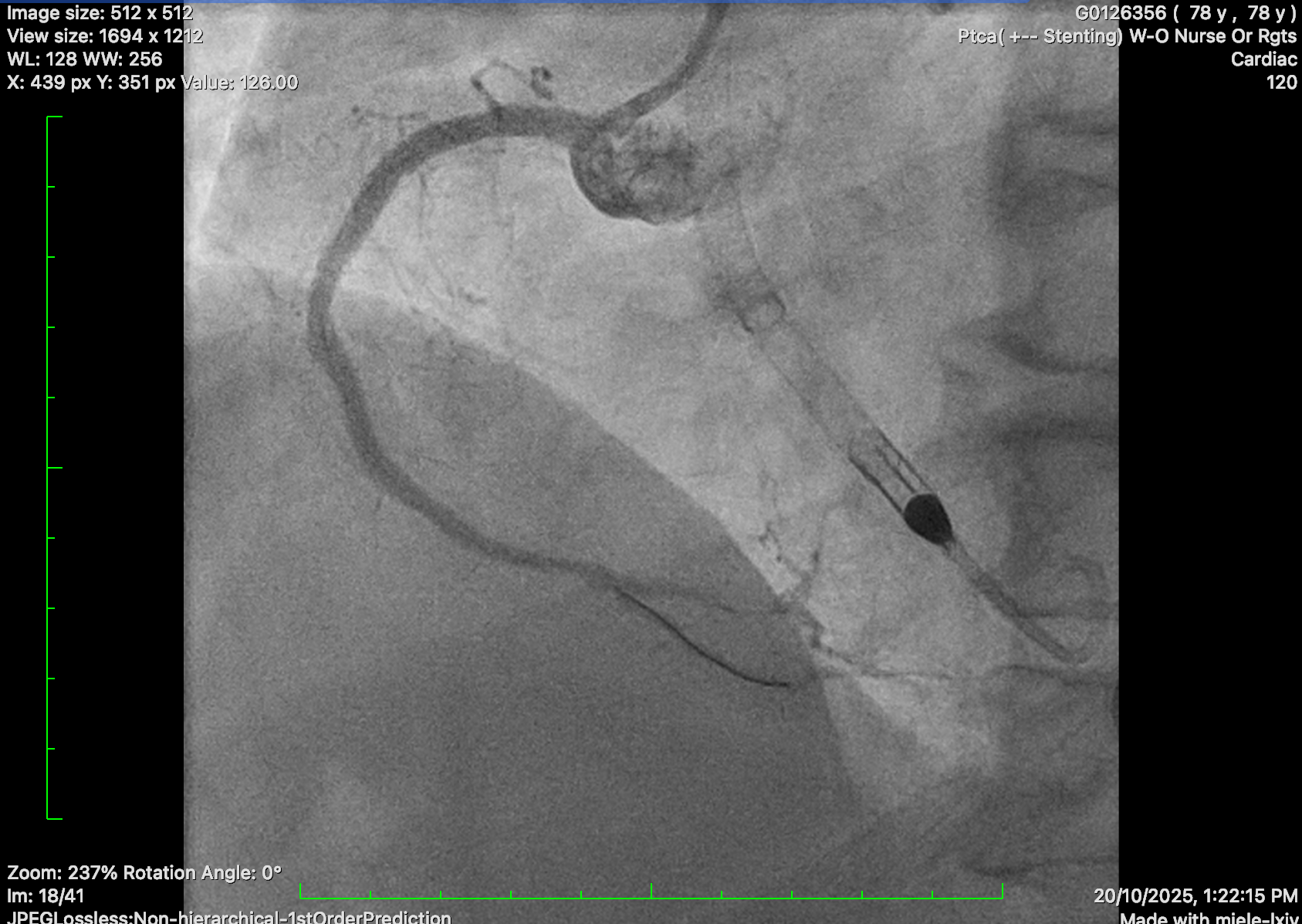
Impella CP inserted due to underlying poor LVEF and intention for rotational atherectomy in the left main.
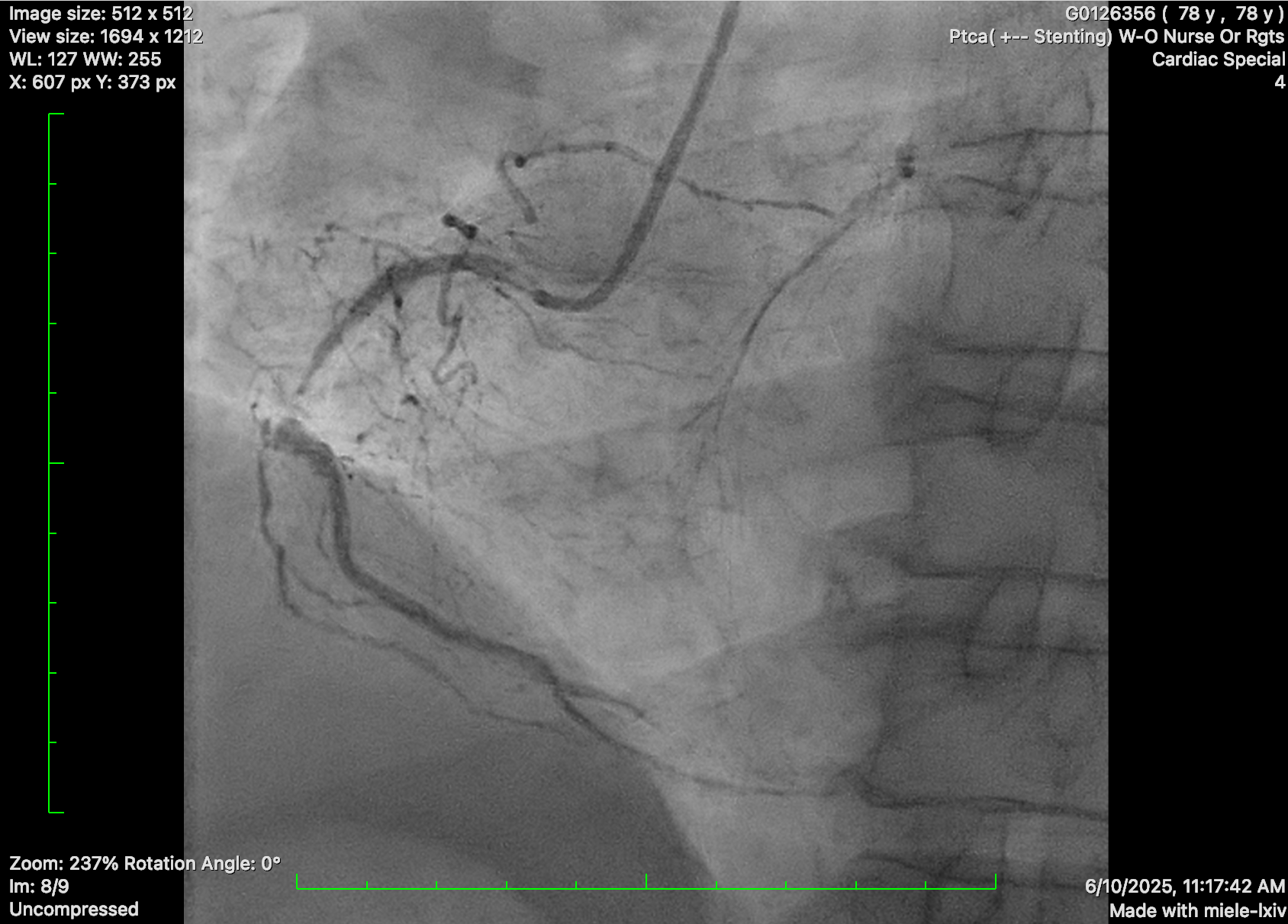
PCI to RCA: JR 4.0 guide catheter. Critical RCA lesion crossed with Fielder XT-R supported by microcatheter. Predilated with semi-compliant balloon and 3.0/40, 3.5/22 and 3.5/9 stents deployed. Post dilated with NC 3.25 balloons.
PCI to LCA: EBU 3.0 7 Fr guide catheter. Successful wiring to distal LAD with workhorse wire. Unable to cross SC 1.0 balloon. Exchanged for Rotawire Extra Floppy. 1.25mm burr for rotational atherectomy with significant decelerations. Still failed to deliver SC 1.0 and 1.5 balloon. Upsized to 1.5mm Rotaburr. Further dilated with SC 1.5 and 2.0 balloon, then shockwave with 2.5 balloon and further predilatation with NC balloon. DES 2.25/30, 3.0/18 and 3.5/24 deployed. Post dilatation with NC 4.0 and 3.5 balloon.
Satisfactory results

PCI to RCA: JR 4.0 guide catheter. Critical RCA lesion crossed with Fielder XT-R supported by microcatheter. Predilated with semi-compliant balloon and 3.0/40, 3.5/22 and 3.5/9 stents deployed. Post dilated with NC 3.25 balloons.
PCI to LCA: EBU 3.0 7 Fr guide catheter. Successful wiring to distal LAD with workhorse wire. Unable to cross SC 1.0 balloon. Exchanged for Rotawire Extra Floppy. 1.25mm burr for rotational atherectomy with significant decelerations. Still failed to deliver SC 1.0 and 1.5 balloon. Upsized to 1.5mm Rotaburr. Further dilated with SC 1.5 and 2.0 balloon, then shockwave with 2.5 balloon and further predilatation with NC balloon. DES 2.25/30, 3.0/18 and 3.5/24 deployed. Post dilatation with NC 4.0 and 3.5 balloon.
Satisfactory results
Case Summary
Calcified coronaries require prolonged procedure using different treatment modalities such as rotational atherectomy and shockwave lithotripsy. The use of Impella in a patient with poor left ventricular function can help support the patient haemodynamically during the procedure, and the use of intravascular images help to decide treatment method and assess immediate results.