Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_032
Intervention for Bilateral Carotid Artery Occlusion and SFA CTO With Repeated Syncope and Claudication
By Chien Hsien Lo
Presenter
Chien Hsien Lo
Authors
Chien Hsien Lo1
Affiliation
Da-Chien General Hospital, Taiwan1
View Study Report
CASE20251114_032
Endovascular - Carotid Intervention
Intervention for Bilateral Carotid Artery Occlusion and SFA CTO With Repeated Syncope and Claudication
Chien Hsien Lo1
Da-Chien General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 81 yr-old patient with history of familial hypercholesterolemia with highest level CHOL 545, LDL-C 423 under PCSK9i treatment, CAD s/p CABG and PCI.
This time complained of chronic dizziness, worsening for one month, recurrent syncope attack for 2 weeks, unstable gait with even unable to walk by support.
He also presented with worsening claudication of both lower limbs.

Relevant Test Results Prior to Catheterization
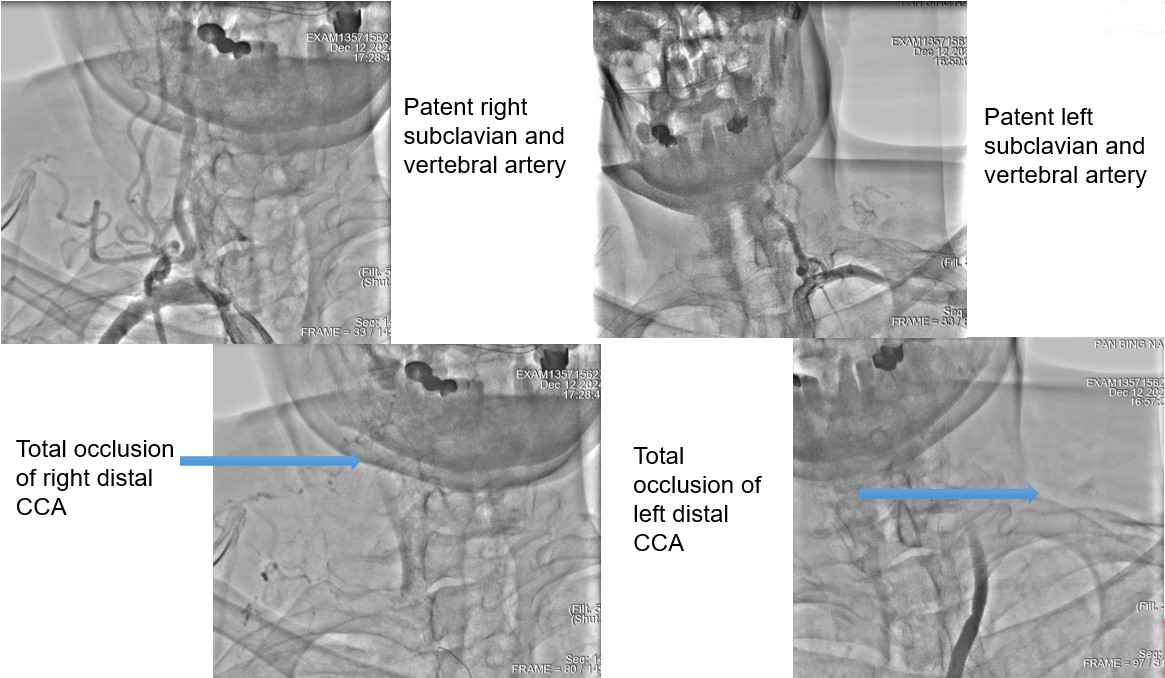
MRI revealed invisible of bilateral ICA, angiography showed bilateral CCA total occlusion with bridge collaterals.ABI showed severe decreased over both sides
Relevant Catheterization Findings
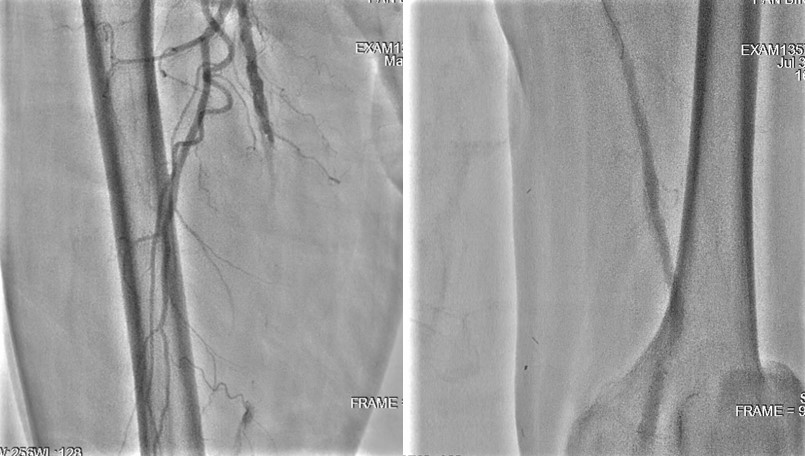
Carotid angiography showed bilateral CCA occlusion with bridge collaterals from vertebral and subclavian artery. Patient refused surgical endarterectomy. Lower limbs angiography revealed right SFA CTO, left SFA distal stenosis.We tried endovascular treatment for left CCA occlusion first but failed.
Interventional Management
Procedural Step
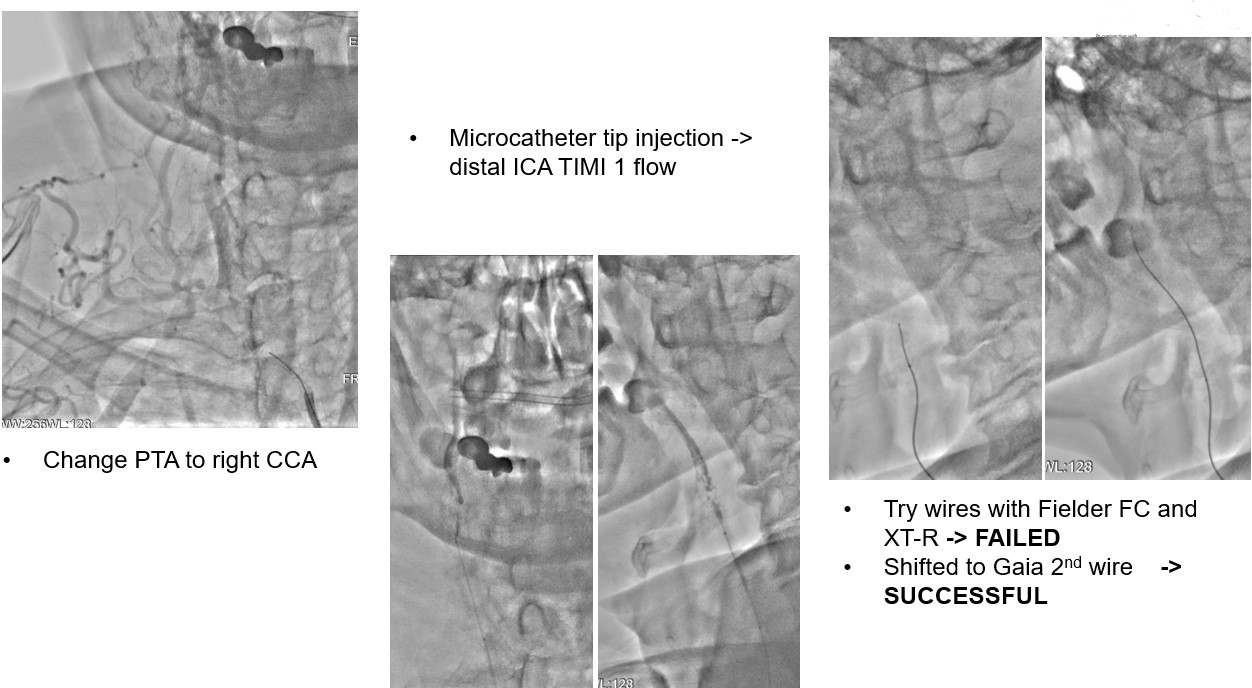
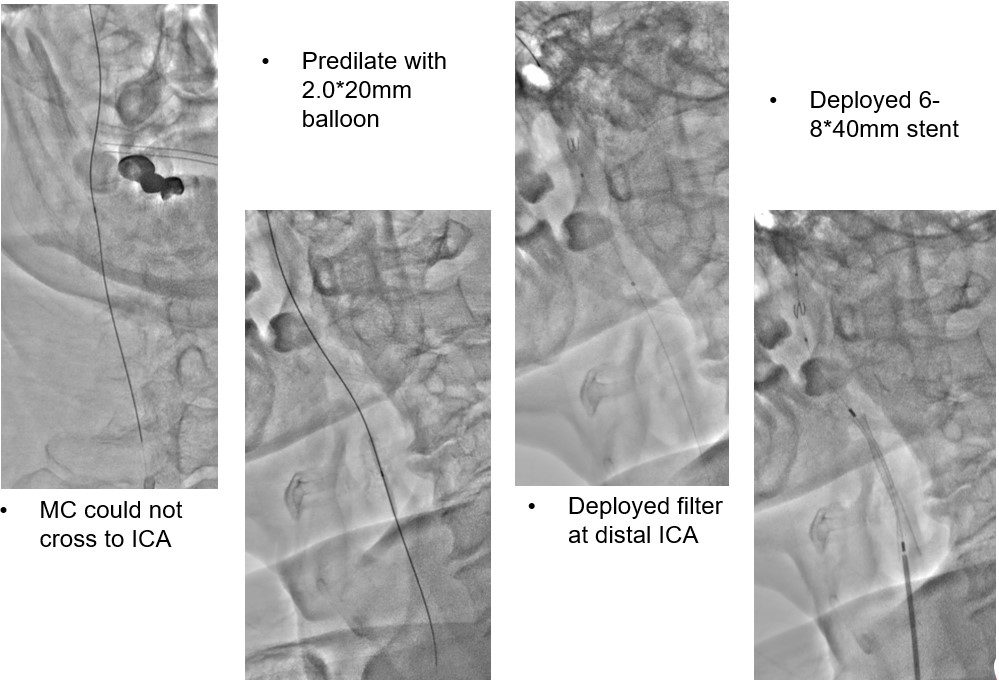
We tried wiring to left ICA occlusion with microcatheter first but failed.Then we tried PTA for right CCA occlusion. With microcatheter support, Gaia 2nd wire advanced to right ICA difficultly2.0mm small balloon pre-dilateddistal filter placement then carotid stenting smoothly.Patient symptoms improved dramatically and discharged 4 days later.We tried elective PTA for right SFA CTO by bilateral puncture approach. Antegrade from left transfemoral cross over sheath, and retrograde from right POPA.Antegrade failed wiringThen retrograde wire successfully advance to antegrade microcatheter -> Rendezvous -> externalization -> balloon pre-dilate and stenting
 se036.avi
se036.avi
se003 rendezvous.avi
se017 final.avi
Case Summary
Familial hypercholesterolemia may cause poly-vascular atherosclerotic diseases (triple vessel CAD, PAOD, bilateral CCA occlusion in our case)Decision of choice for revascularization in bilateral CCA total occlusion is importantEndovascular treatment for CCA-ICA occlusion is controversial and also challengeDistal ICA filtering and carotid stenting is a treatment of choice and can be considered if other treatment option unavailable