Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_031
A Case of Successful Debulking of an Eccentric Calcified LAD Lesion Through Wire Bias Modification
By Jumpei Koike, Yoshihiro Iwasaki
Presenter
Jumpei Koike
Authors
Jumpei Koike1, Yoshihiro Iwasaki1
Affiliation
Omi Medical Center, Japan1
View Study Report
CASE20251114_031
Coronary - Complex PCI - Calcified Lesion
A Case of Successful Debulking of an Eccentric Calcified LAD Lesion Through Wire Bias Modification
Jumpei Koike1, Yoshihiro Iwasaki1
Omi Medical Center, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
A man in his seventies presented with a two-month history of exertional chest pain. On admission he was hemodynamically stable, with no remarkable physical findings. His cardiovascular risk factors included diabetes mellitus, dyslipidemia, hypertension, and a past smoking history.
Relevant Test Results Prior to Catheterization
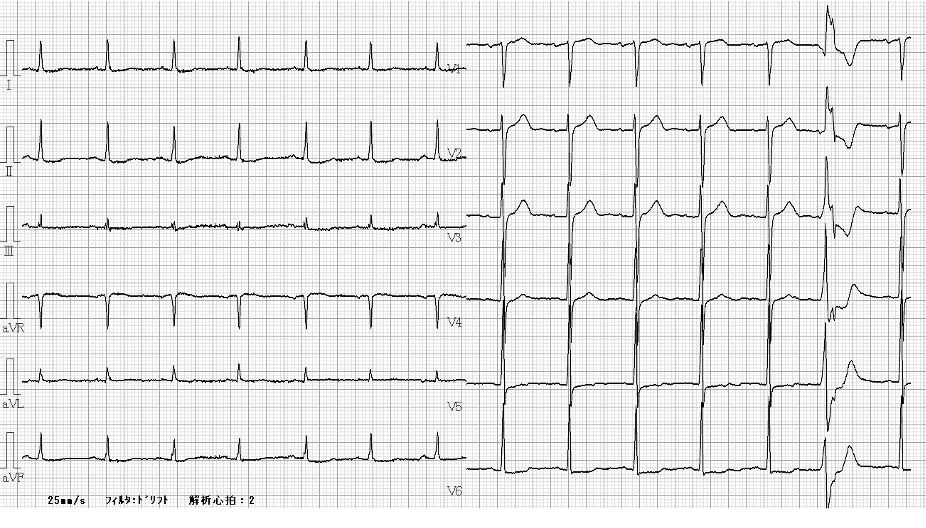
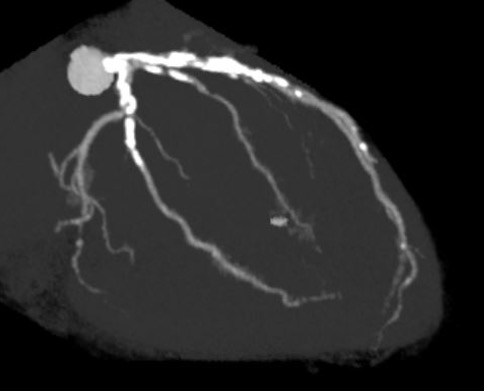
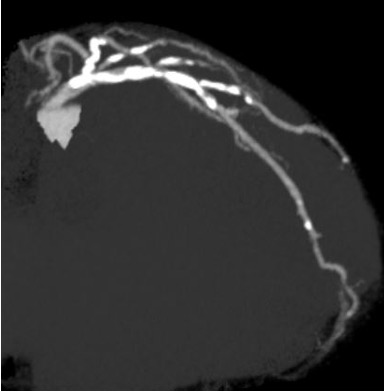
Resting ECG showed ST-segment depression in leads V5–V6. Echocardiography demonstrated preserved left ventricular systolic function with an ejection fraction of 67%. Laboratory tests showed normal renal function and a normal BNP level. Coronary CT angiography revealed severe calcification in both the LAD and left circumflex arteries.
Relevant Catheterization Findings
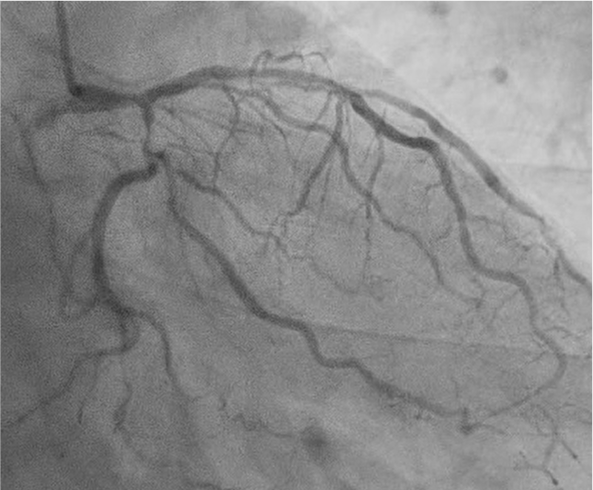
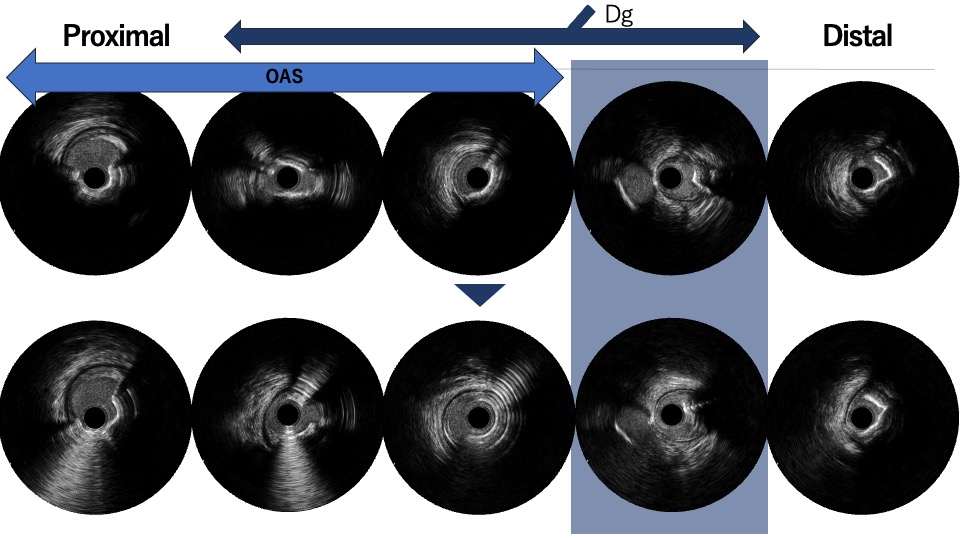
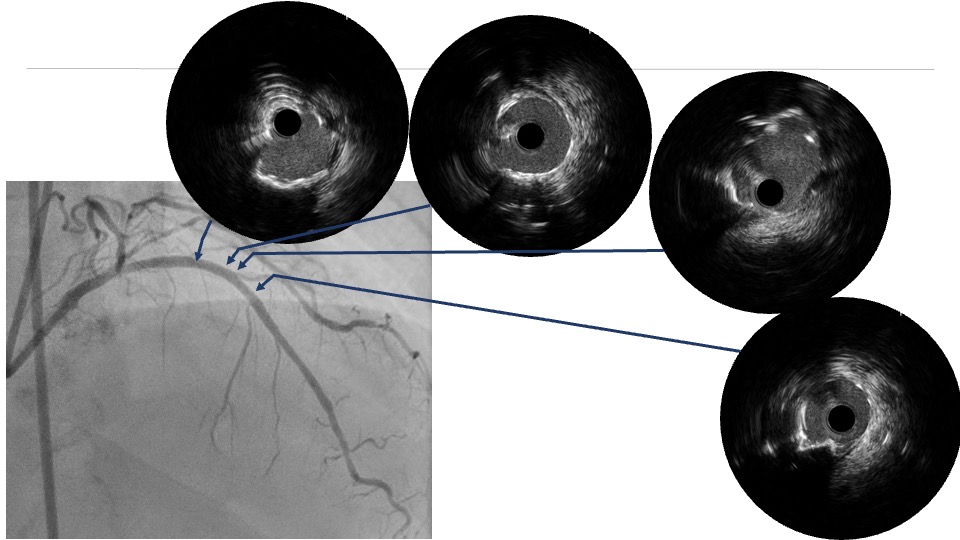
Coronary angiography via the radial approach showed a severe proximal LCx stenosis and a long, severe mid-LAD stenosis, while the RCA had no significant disease. IVUS of the LAD demonstrated diffuse calcification and an eccentric calcified plaque protruding from the septal side near the diagonal branch bifurcation. The guidewire was biased toward the diagonal branch, causing tenting of the relatively healthy wall at the most critical segment.

Interventional Management
Procedural Step
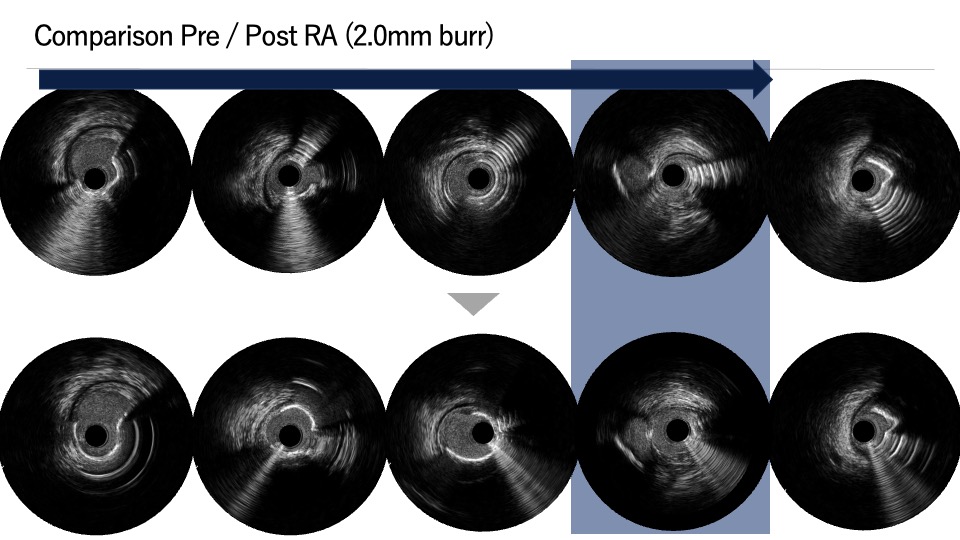
PCI was first performed for the LCx, using orbital atherectomy followed by cutting balloon predilatation and drug-coated balloon therapy with good angiographic result. One month later, PCI was attempted for the LAD lesion using a 8F system via right femoral approach. Intravascular ultrasound (IVUS) revealed a diffusely eccentric calcified plaque located on the septal side. While wire bias in the proximal segment was toward the calcified plaque, the distal segment showed tenting of the wire toward a plaque-free site on the diagonal branch side. At this point, we considered that debulking of the distal segment would be a high risk of vessel injury. We hypothesized that performing proximal segment debulking that had a favorable wire bias might shift the overall wire bias toward the septal side. Then Only proximal OAS was performed using pull-back ablation.Follow-up IVUS showed disappearance of distal tenting and favorable wire bias toward the calcified plaque. As a result, OAS was safely performed in the distal segment as well. Additional debulking of the residual calcified plaque was conducted with a 2.0 mm Rotablator. IVUS confirmed effective debulking without vessel injury in the area of concern. The entire lesion was then dilated with a CB; however, a dissection with hematoma occurred, and a drug-eluting stent (DES) was implanted. Final IVUS demonstrated acceptable stent expansion, and final angiography showed no residual stenosis or flow limitation.
Case Summary
In this diffusely calcified, eccentric LAD lesion, initial proximal debulking with orbital atherectomy intentionally modified wire bias and eliminated distal tenting, thereby enabling safe atherectomy in a high-risk distal segment. This case suggests that targeted proximal plaque modification can be a practical strategy for wire bias control in complex eccentric calcified disease, and underscores the importance of repeated IVUS assessment during such procedures.