Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_029
Aortic Injury With Intimo-Intimal Intussusception During Transcatheter Aortic Valve Replacement
By Euihong Ko
Presenter
Euihong Ko
Authors
Euihong Ko1
Affiliation
Kokura Memorial Hospital, Japan1
View Study Report
CASE20251114_029
Structural - Aortic Valve Intervention - Complex TAVR
Aortic Injury With Intimo-Intimal Intussusception During Transcatheter Aortic Valve Replacement
Euihong Ko1
Kokura Memorial Hospital, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
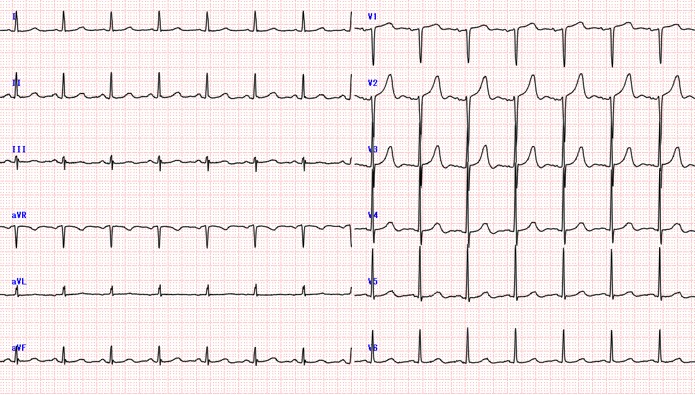
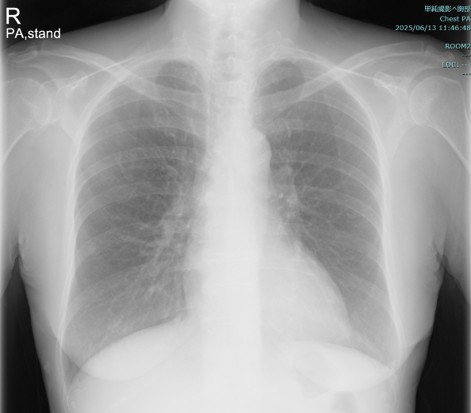
A70-year-old female referred to our institution with progressive chest pain on exertion that had persisted for about 1 month. On physical examination, she was normotensive(114/56 mmHg). She also had a 4/6 systolic murmur. She had been diagnosed AuDHD (autism and attention-deficit hyperactivity disorder) at the age of 19. Other comorbidities included hypertension and hyperlipidemia.
Relevant Test Results Prior to Catheterization
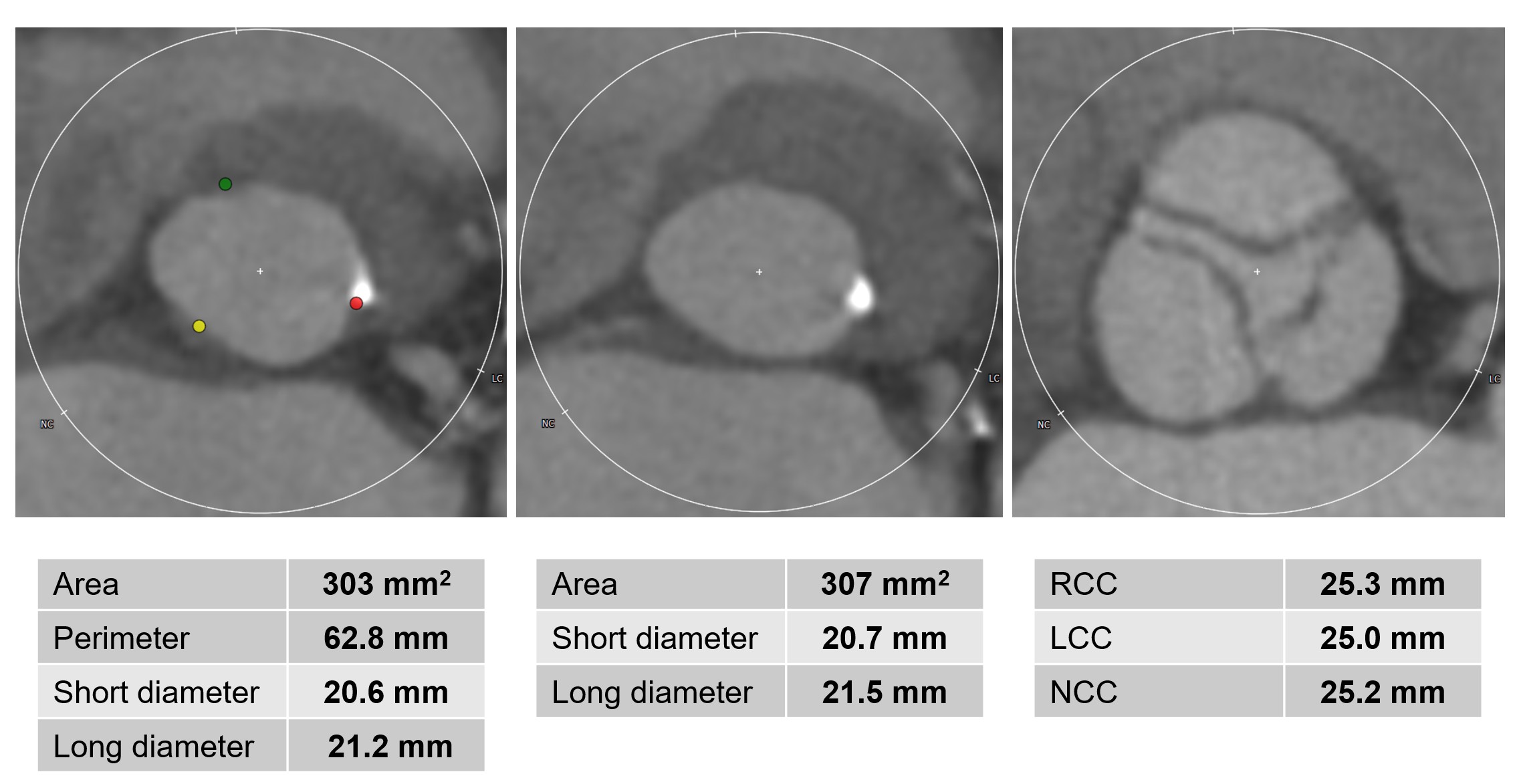
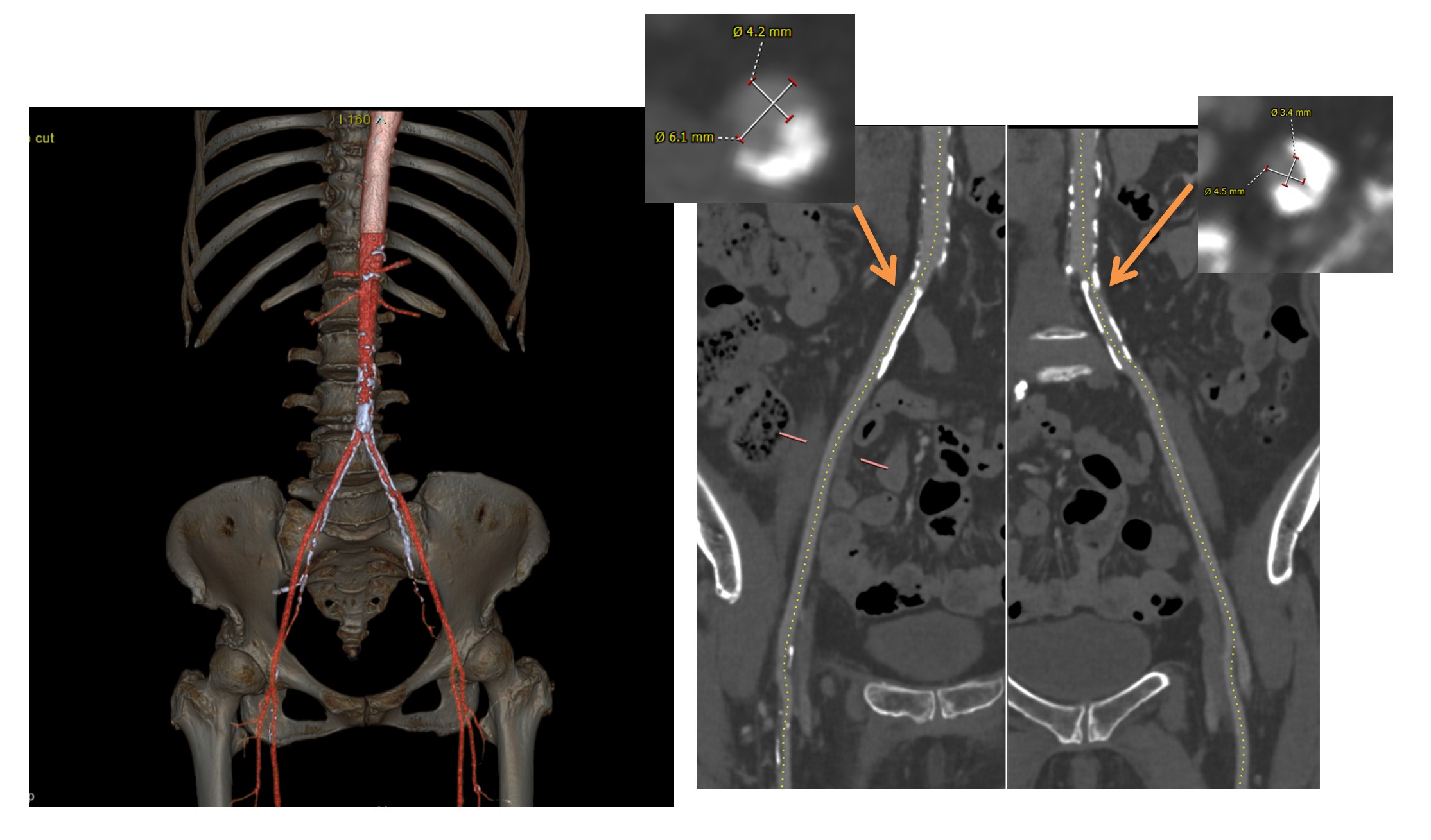
Echocardiographyshowed preserved ejection fraction of 66.8%, with aortic valve area of 0.51cm2. Thepeak velocity across the aortic valve was 4.64 m/s, with a meanpressure gradient of 53.9 mmHg. CT finding showed a severelycalcified trileaflet aortic valve with annulus area of 302.5 mm2,and perimeter of 62.8 mm. Minimum diameter of bilateral iliofemoral artery was5.2 mm without calcification.
 01. Long axis.mp4
01. Long axis.mp4
02. short axis.mp4
04. AV.mp4
Relevant Catheterization Findings
Interventional Management
Procedural Step
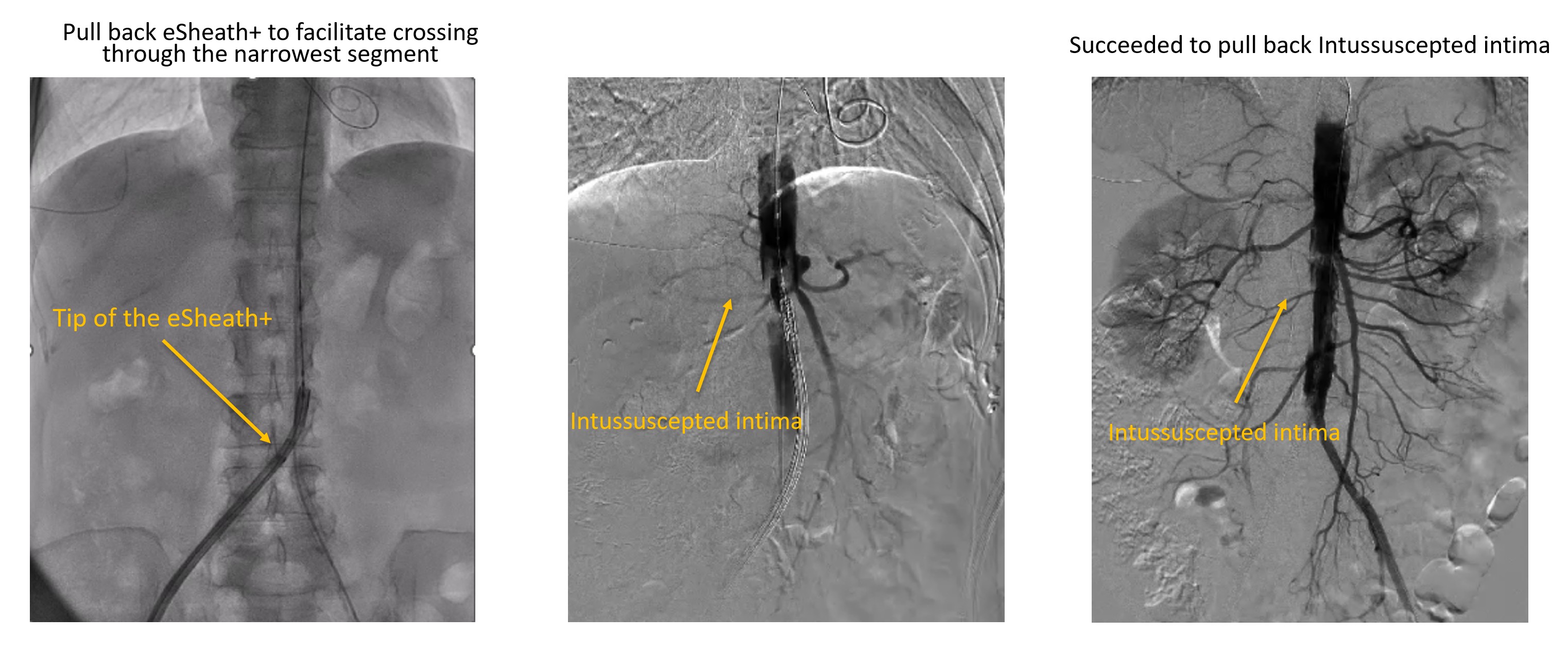
The procedure was performed under conscious sedation. A 14F eSheath+ was inserted via right femoral artery. The aortic valve was crossed using an AL 1.0 with an Argon straight wire, which was exchanged for SAFARI2 small. Although the diameter of iliofemoral artery was enough, delivery of SAPIEN 3 Ultra RESILIA 20 mm (S3UR) through the14F eSheath+ was challenging. The SAFARI2 wire was subsequently exchanged for a Confida Guidewire to get adequate support and back-up force; however, this also failed. Therefore, the 14F eSheath+ was pulled back to the common iliac artery, and the S3UR valve was advanced without the sheath to facilitate crossing through the narrowest segment of the iliofemoral artery. This maneuver succeeded to advance S3UR into abdominal aorta (Video 1). However, patient suddenly claimed severe abdominal pain and aortography revealed intimo-intimal intussusception, possibly caused during valve delivery (Video 2). Intravascular ultrasound (IVUS) also confirmed completely intussuscepted intima, and revealed absence of intimal layer at the terminal aorta. The TAVR procedure was subsequently aborted. The resultant tubular structure of completely detached intima posed a risk of antegrade or retrograde migration, potentially leading to acute aortic occlusion. Therefore, an endoprosthesis (GORE EXCLUDER) was implanted in the infrarenal aorta to stabilize the lesion (Video 3).
Video 1.mp4
Video 2.mp4
Video 3.mp4
Case Summary
Covering S3UR with the eSheath+ is essential, particularly during advancing tortuous and/or narrowed aortic segment to prevent aortic injury. Using larger size of sheath (16FeSheath+) may improve deliverability and safety. Additionally, in patients with a small iliofemoral arteries, selecting a transcatheter heart valve with better crossability-such as the NAVITOR-would be considered.