Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_023
Protected Precision: Impella-Supported Rotational Atherectomy of the Left Main Bifurcation
By Yu Chuan Chuang, Wen-Lieng Lee
Presenter
Yu Chuan Chuang
Authors
Yu Chuan Chuang1, Wen-Lieng Lee1
Affiliation
Taichung Veterans General Hospital, Taiwan1
View Study Report
CASE20251114_023
Coronary - Complex PCI - Left Main
Protected Precision: Impella-Supported Rotational Atherectomy of the Left Main Bifurcation
Yu Chuan Chuang1, Wen-Lieng Lee1
Taichung Veterans General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
An 82-year-old woman (BMI 26 kg/m²) presented with several weeks of typical exertional chest tightness that was refractory to antianginal therapy. Her past medical history included type 2 diabetes mellitus, hyperlipidemia, and hypertension. She denied any smoking or family history of premature coronary artery disease.

Relevant Test Results Prior to Catheterization
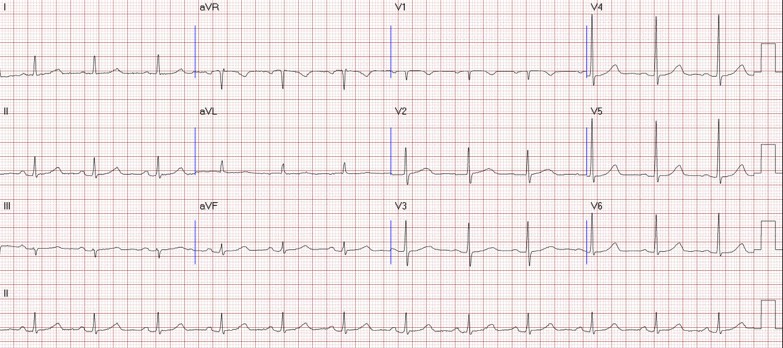
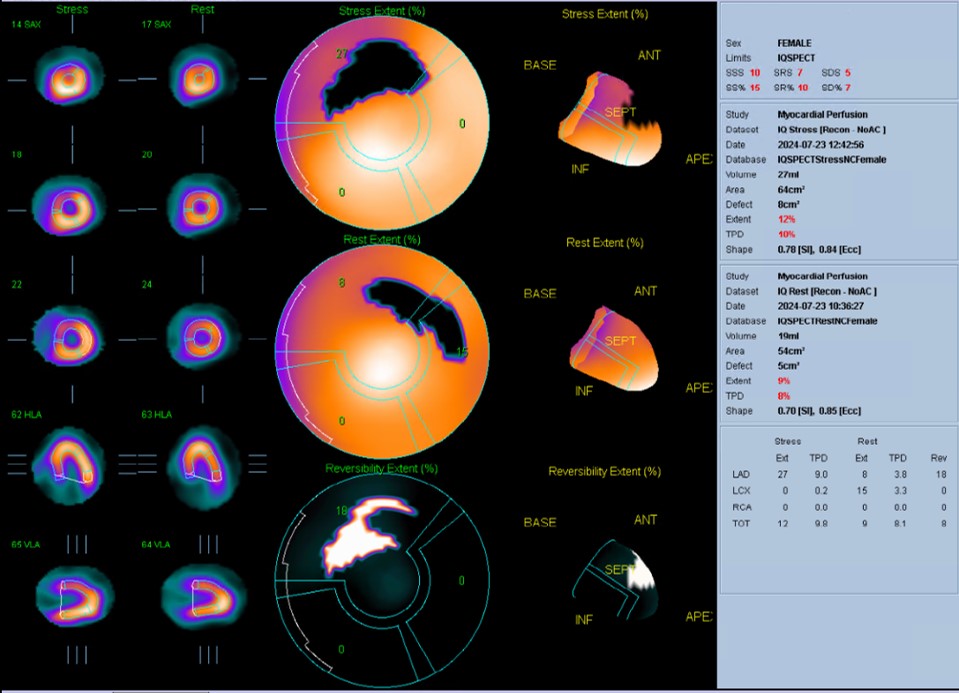
Chest radiography showed no evidence of heart failure. Transthoracic echocardiography demonstrated a left ventricular ejection fraction of 60% with no regional wall-motion abnormalities and no significant valvular heart disease. A myocardial perfusion scan revealed reversible ischemia, suggestive of underlying obstructive coronary artery disease.
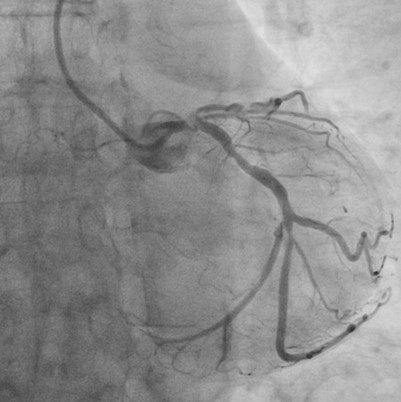
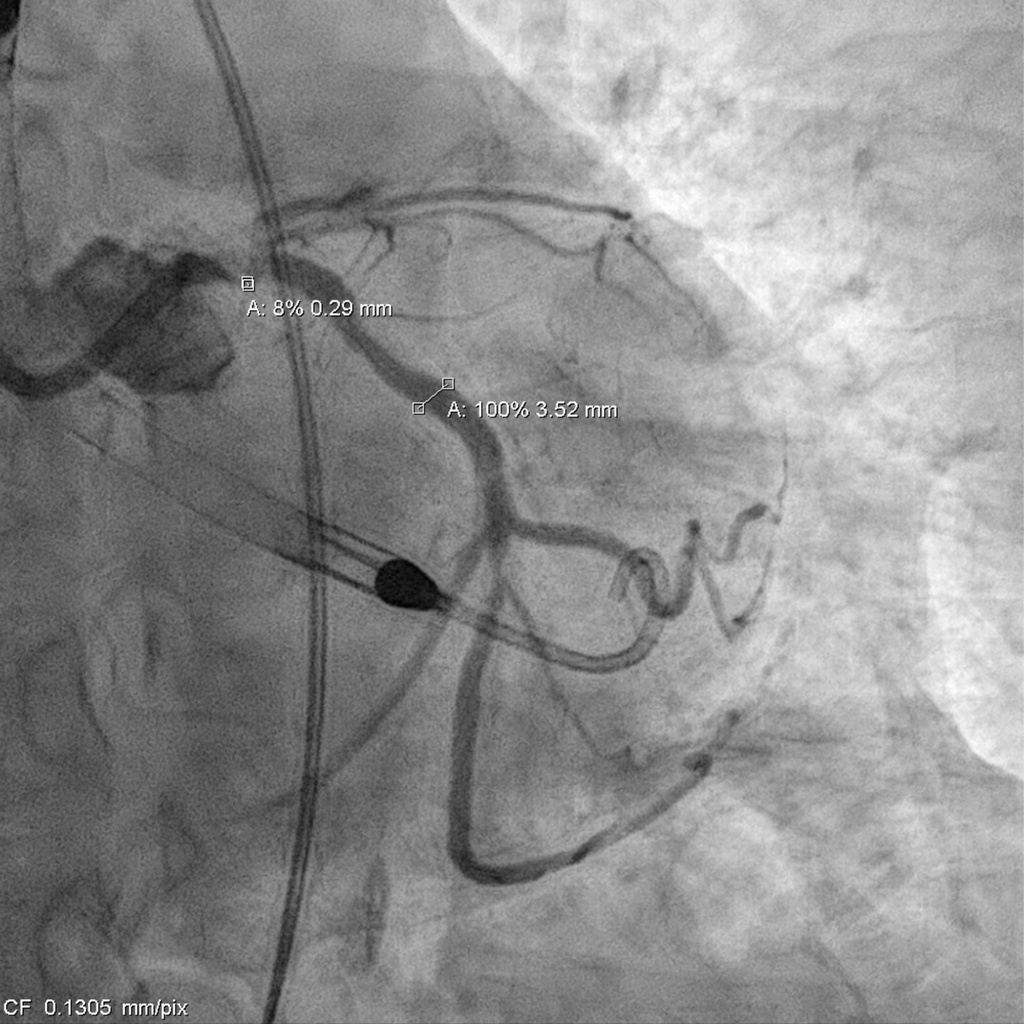
Relevant Catheterization Findings
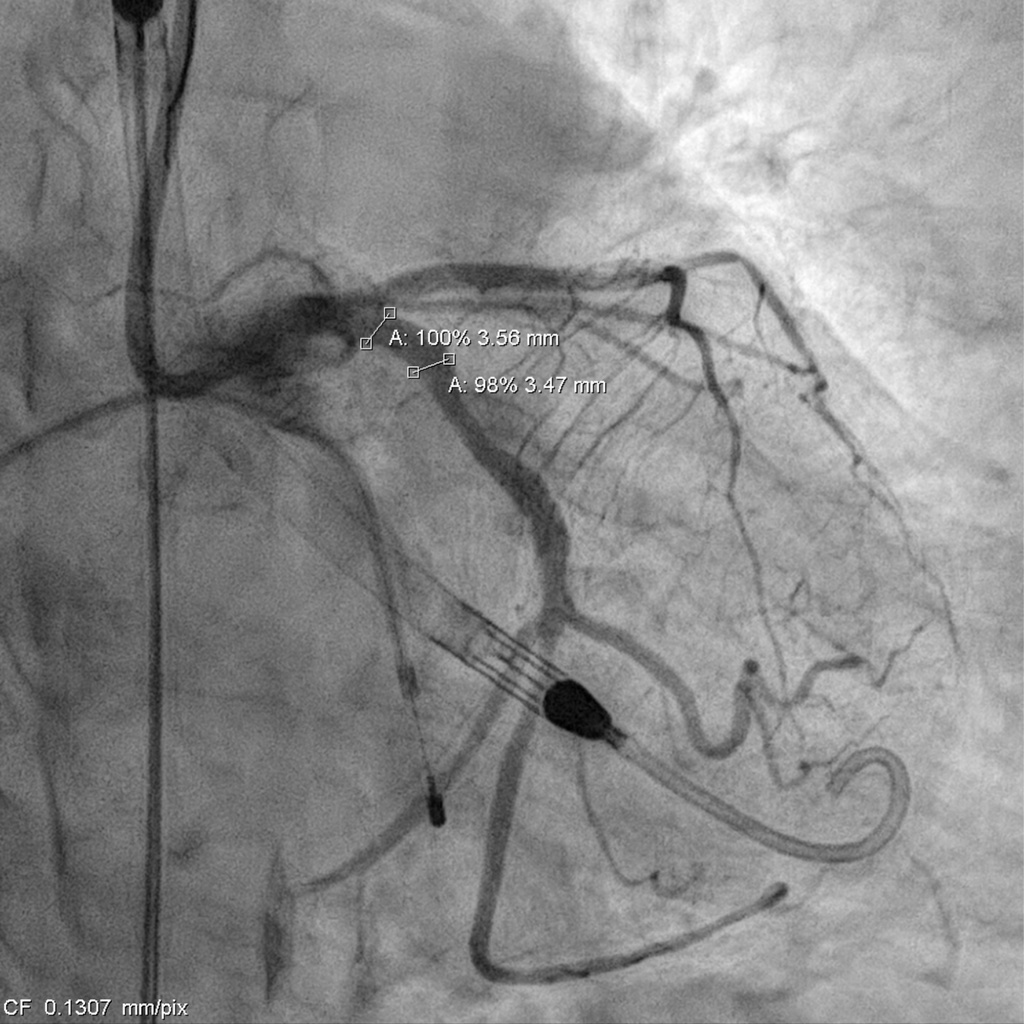
Catheterization revealed a 95% distal left main stenosis with a calcified nodule protruding into the LAD and LCX ostia, a 99% proximal LAD lesion with an additional 90% stenosis after the first diagonal branch, non-critical LCX disease, and a 70% proximal RCA lesion with multiple critical PDA stenoses. The patient and family declined PCI in the cath lab, with a Syntax score of 40.

 000715889G_003.AVI
000715889G_003.AVI
000715889G_006.AVI
000715889G_010.AVI
Interventional Management
Procedural Step
Impella support was established before the procedure. The LCA was engaged with an EBU 3.0 × 7 Fr guide, and a SUOH-03 wire was advanced into the LCX. A 2.0 × 20 mm balloon was inflated across the very tight LM–LCX lesion, but IVUS still could not cross, so rotablation was performed first. The SUOH-03 wire was exchanged for a Rota Floppy using a Caravel microcatheter, and a 2.0 mm burr successfully ablated the heavily calcified, angulated LM–LCX segment.After calcium modification, a Fielder FC wire was advanced into the LAD using a reverse-wire technique. Severe mid-LAD calcification required switching to a Rota Floppy wire, and a 1.25 mm burr was used for LAD rotablation. Bradycardia occurred during Rota, so a temporary pacemaker was inserted. A 2.25 × 15 mm NC balloon was then inflated to 12 atm to further prepare the LAD.The LAD was stented with an Onyx 2.25 × 22 mm DES (6–16 atm) and subsequently crushed with a 3.5 × 12 mm NC balloon. LM–LCX was stented with an Onyx 3.5 × 15 mm DES (11–12 atm). LAD was rewired with a Sion Blue supported by a Crusade dual-lumen catheter, and stent struts were opened using 1.5 × 10 mm and 2.5 × 15 mm balloons. LAD-P was post-dilated with a 2.5 × 15 mm NC (10 atm), and LM–LAD with a 2.5 × 15 mm NC (12–18 atm). Final kissing inflation with a 3.5 × 12 mm NC and 2.5 × 15 mm NC balloons achieved optimal flow.The Impella was removed under stable hemodynamics, and the access site was closed with two Perclose devices without bleeding.

000715889G_040.AVI
000715889G_012.AVI
000715889G_021.AVI
Case Summary
- Mechanical debulking of bulky calcified nodules is crucial when wire bias is evident on angiography or intravascular imaging, as inadequate lesion preparation increases procedural risk.
- Distal left main calcium nodules extending into the LAD or LCX ostium can create significant wiring challenges; upfront mechanical debulking should be strongly considered in such anatomies.
- Mechanical circulatory support (e.g., Impella) plays a vital role in CHIP (complex high-risk indicated PCI) procedures to maintain hemodynamic stability and reduce the risk of catastrophic compromise during extensive plaque modification.