Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_022
Adopting the Shock Protocol: Early Utilization of MCS in AMI Patient With Cardiogenic Shock
By Jonathan Gabriel Sung
Presenter
Jonathan Gabriel Sung
Authors
Jonathan Gabriel Sung1
Affiliation
Tuen Mun Hospital, Hong Kong, China1
View Study Report
CASE20251114_022
Heart Failure - Mechanical Circulatory Support
Adopting the Shock Protocol: Early Utilization of MCS in AMI Patient With Cardiogenic Shock
Jonathan Gabriel Sung1
Tuen Mun Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
We report a case of a 60-year-old gentleman, chronic smoker with otherwise unremarkable past health, who presented to the emergency department with acute onset chest pain for 12 hours. Upon arrival, his blood pressure was 80/40 mmHg with heart rate of 80 bpm. His SaO2 was 92% on 4L/min O2. He appeared drowsy with altered sensorium and was vomiting during assessment.
Relevant Test Results Prior to Catheterization
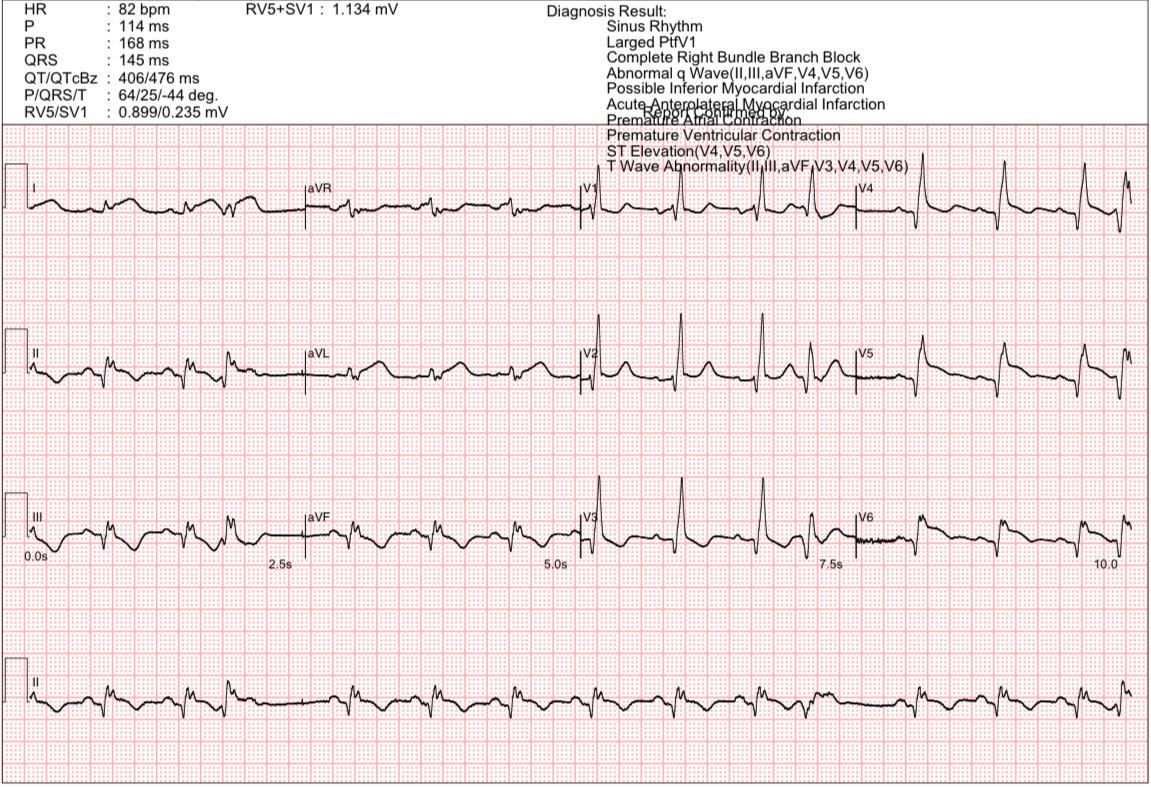
ECG in the emergency department showed sinus rhythm with ST elevation in anterolateral leads and right bundle branch block. Bedside echocardiogram revealed a severely impaired LV systolic function with an estimated LVEF of 30% and no signs of mechanical complications.
Relevant Catheterization Findings
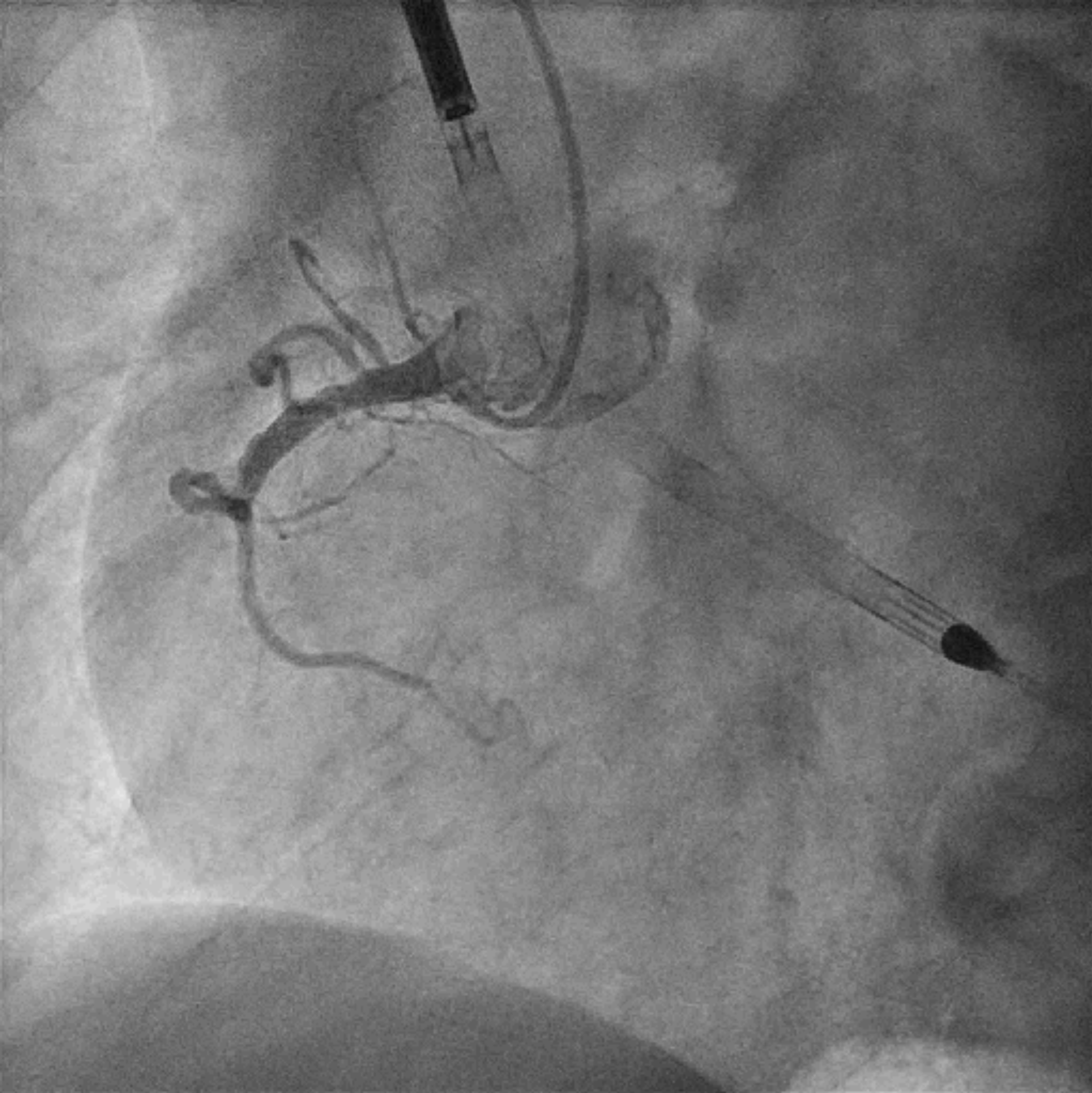
Patient was immediately brought to the catheterization laboratory. During transfer he required escalating inotropic support. LVEDP using a 5Fr pigtail catheter measured 30 mmHg. Coronary angiogram revealed minor disease in LMCA, proximal LAD acute total occlusion, LCx minor disease, proximal RCA total occlusion with no obvious collateral supply.
 LCA Coro.avi
LCA Coro.avi
RCA Coro.avi
Interventional Management
Procedural Step
Left common femoral artery and vein, and right common femoral artery were punctured under ultrasound and fluoroscopy guidance with micropuncture set. Prior to coronary angiogram, Impella was inserted via right common femoral artery into LV. ICU was informed to provide potential ECMO support in the event of further hemodynamic collapse.
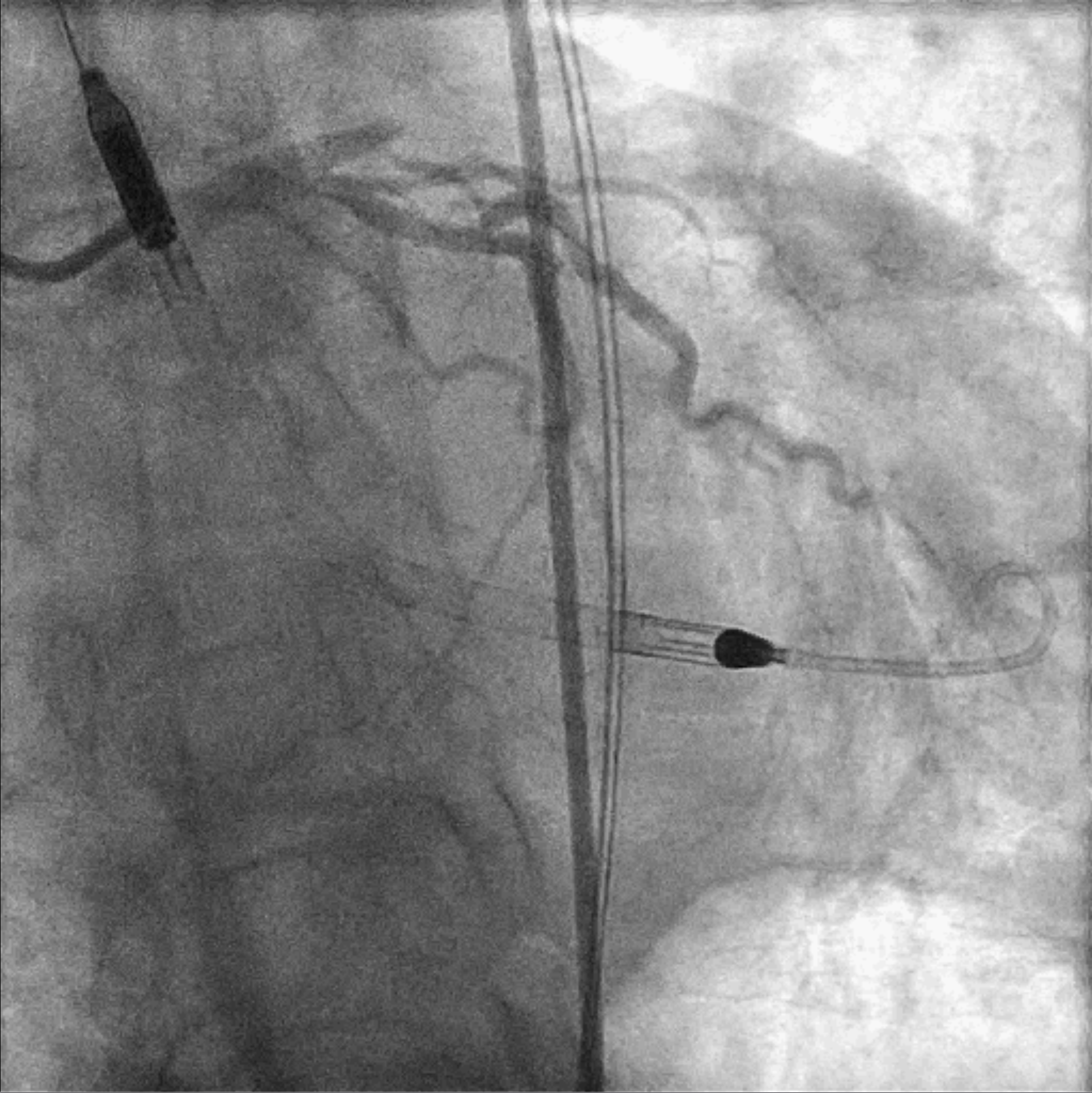
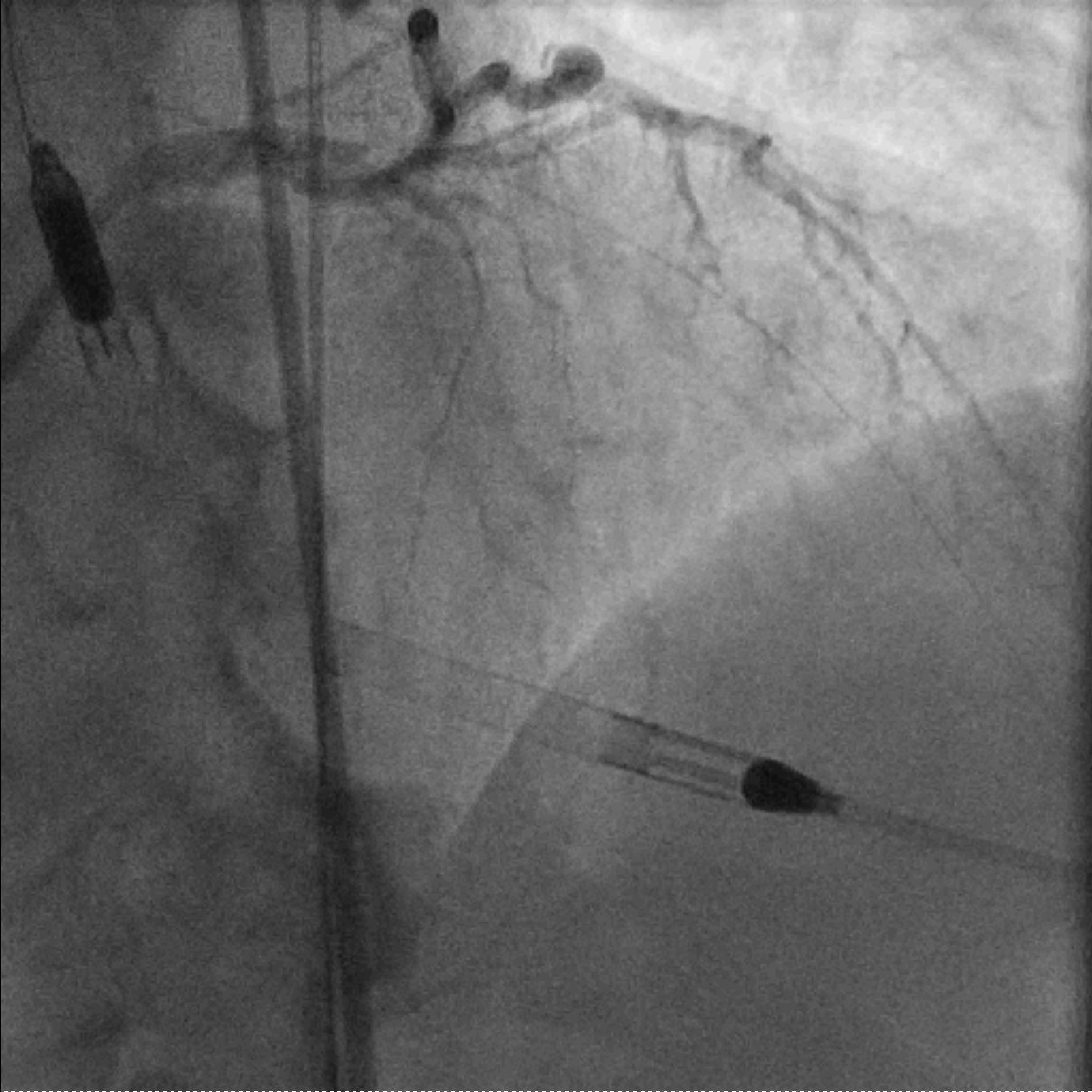
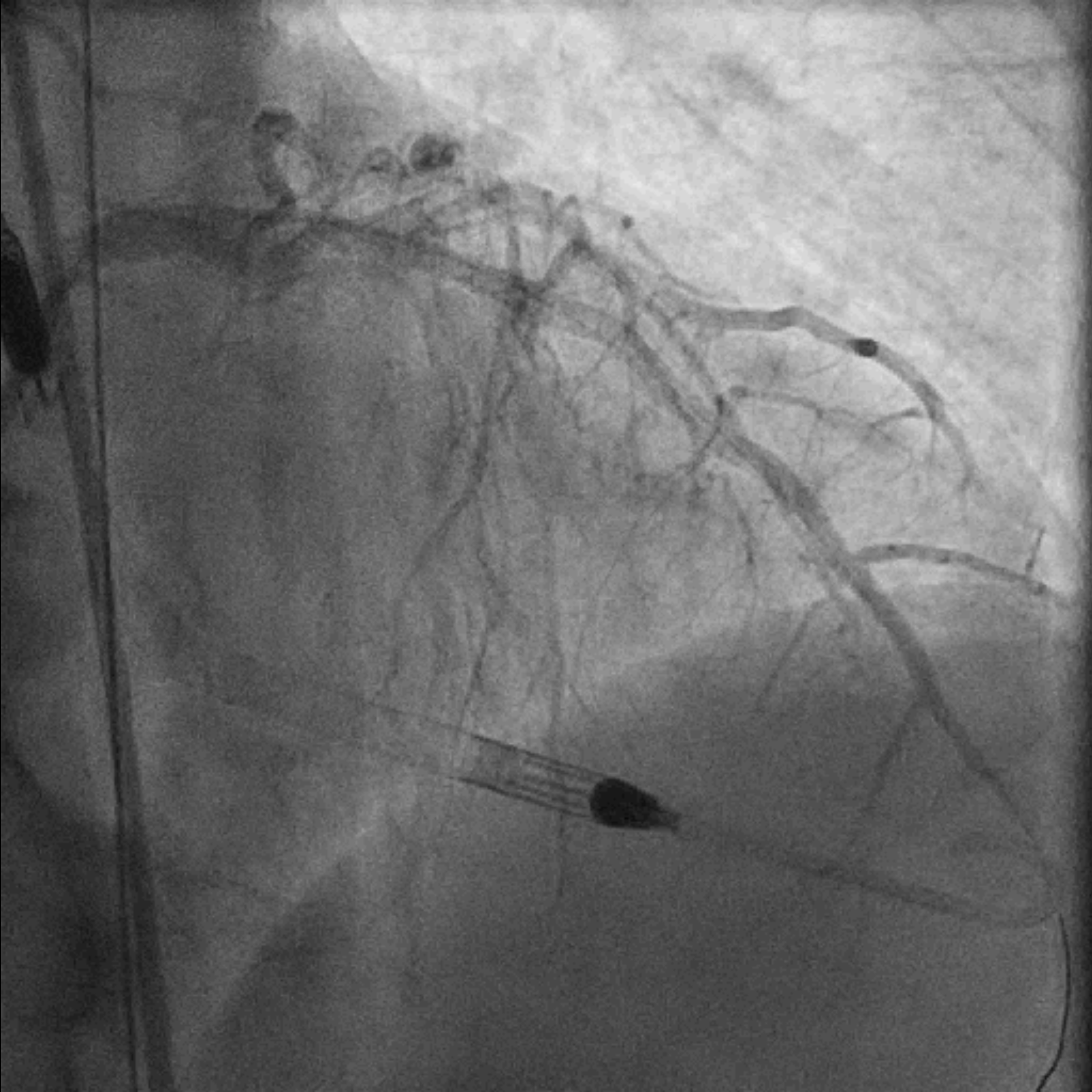
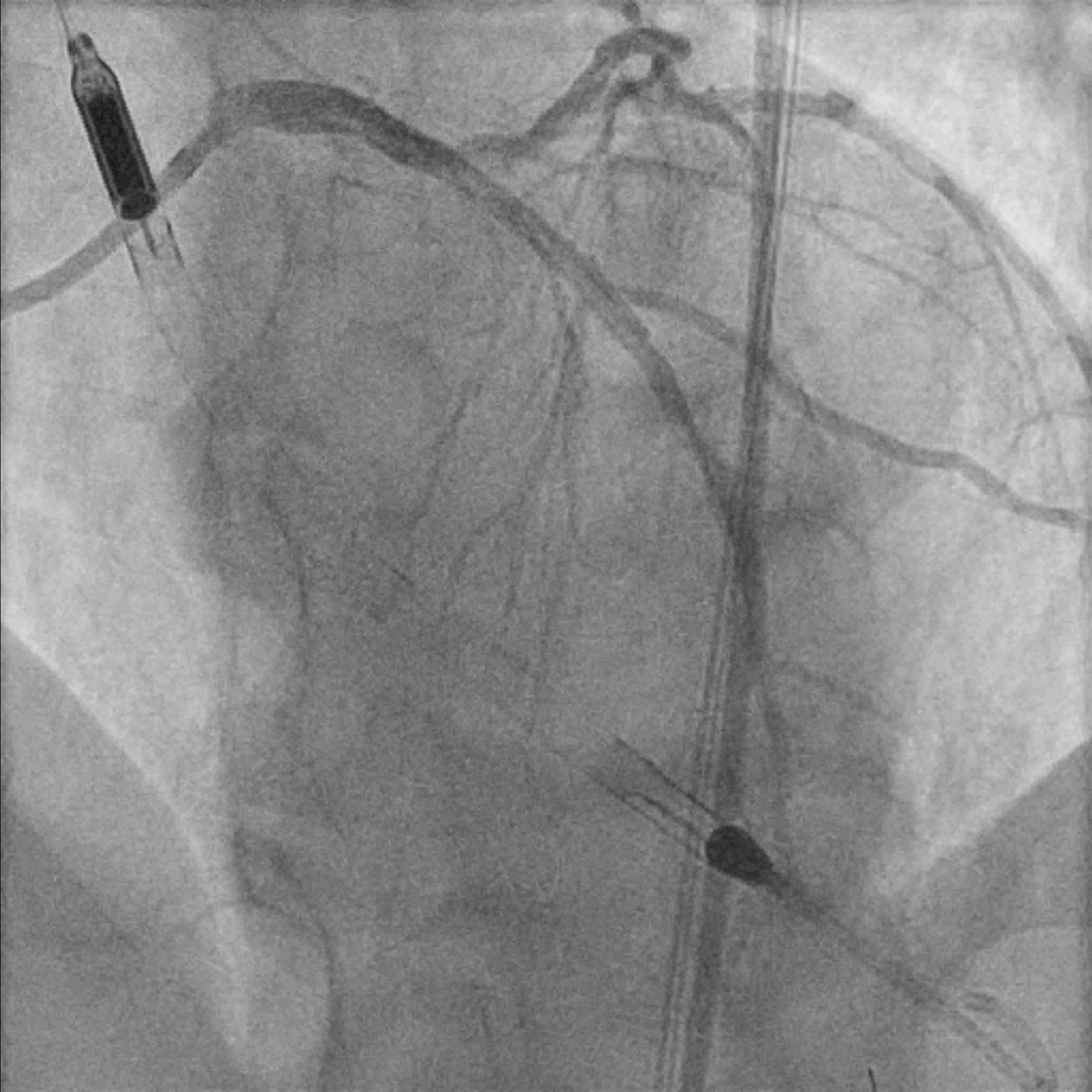
EBU 3.5 7Fr was used to engage left main common artery. Proximal LAD lesion was crossed with a Corsair Pro XS supported Fielder XT-R. Dottering with Sapphire 2.0/15 was unable to achieve flow in LAD. Low pressure inflation of 2.0 mm x 15 mm semi-compliant balloon at ostial to proximal LAD restored TIMI II flow. IVUS demonstrated organised clot in pLAD and plaque extension into LM. A 3.5 mm x 48 mm DES was deployed over mid-LM to mLAD at nominal pressure. The stent was further optimized with 5.0 mm x 6 mm and 4.0 mm x 15 mm non-compliant balloons under IVUS guidance. Intracoronary Adenosine was administered to improve coronary flow. Final angiogram showed TIMI III flow with no immediate complications. Faint retrograde flow to distal RCA was observed. A brief attempt to open RCA was made as the chronicity of the lesion was uncertain. However, Fielder XT-A supported by Corsair Pro XS failed to cross the lesion and the procedure was aborted.
Impella CP was kept in place as patient was transferred back to cardiac care unit. A pulmonary artery line was inserted for monitoring purpose. His hemodynamic status remained stabilized at the end of the procedure.
LAD Wiring.avi
LAD Final.avi
LAD Final 1.avi
EBU 3.5 7Fr was used to engage left main common artery. Proximal LAD lesion was crossed with a Corsair Pro XS supported Fielder XT-R. Dottering with Sapphire 2.0/15 was unable to achieve flow in LAD. Low pressure inflation of 2.0 mm x 15 mm semi-compliant balloon at ostial to proximal LAD restored TIMI II flow. IVUS demonstrated organised clot in pLAD and plaque extension into LM. A 3.5 mm x 48 mm DES was deployed over mid-LM to mLAD at nominal pressure. The stent was further optimized with 5.0 mm x 6 mm and 4.0 mm x 15 mm non-compliant balloons under IVUS guidance. Intracoronary Adenosine was administered to improve coronary flow. Final angiogram showed TIMI III flow with no immediate complications. Faint retrograde flow to distal RCA was observed. A brief attempt to open RCA was made as the chronicity of the lesion was uncertain. However, Fielder XT-A supported by Corsair Pro XS failed to cross the lesion and the procedure was aborted.
Impella CP was kept in place as patient was transferred back to cardiac care unit. A pulmonary artery line was inserted for monitoring purpose. His hemodynamic status remained stabilized at the end of the procedure.
Case Summary
Patient was weaned off Impella and inotrope 4 days later. He returned for further optimization of LM-LAD stent 2 weeks later. Prior to discharge, he was optimized on guideline-directed medical therapy. He remained well to this day, approximately one year after index admission.
This case illustrated the importance of early utilization of mechanical circulatory support in AMI patients with cardiogenic shock. Initiation of Impella before primary PCI provided timely hemodynamic support and effective unloading of the LV, which could potentially reduce LV infarct size. The use of standardized, and multidisciplinary approach with a shock protocol in such scenario could significantly improve outcome.
This case illustrated the importance of early utilization of mechanical circulatory support in AMI patients with cardiogenic shock. Initiation of Impella before primary PCI provided timely hemodynamic support and effective unloading of the LV, which could potentially reduce LV infarct size. The use of standardized, and multidisciplinary approach with a shock protocol in such scenario could significantly improve outcome.