Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_021
The Role of the Cardiac Physiologist in Complex Percutaneous Coronary Intervention: Intravascular Imaging-Guided Orbital Atherectomy to Treat a Heavily Calcified Right Coronary Artery
By Samantha Cashell, Scott Harding, Sarah Fairley
Presenter
Samantha Cashell
Authors
Samantha Cashell1, Scott Harding1, Sarah Fairley1
Affiliation
Wellington Regional Hospital, New Zealand1
View Study Report
CASE20251114_021
Coronary - Complex PCI - Calcified Lesion
The Role of the Cardiac Physiologist in Complex Percutaneous Coronary Intervention: Intravascular Imaging-Guided Orbital Atherectomy to Treat a Heavily Calcified Right Coronary Artery
Samantha Cashell1, Scott Harding1, Sarah Fairley1
Wellington Regional Hospital, New Zealand1
Clinical Information
Relevant Clinical History and Physical Exam
A 79-year old male with hypertension and moderate left ventricular impairment was admitted to hospital with a non-ST segment elevation myocardial infarction (NSTEMI). A diagnostic angiogram showed severe right coronary disease with moderate disease in the left coronary system (Figure 1a - 1c). The patient was transferred to our tertiary centre for complex percutaneous coronary intervention (PCI) to the culprit right coronary artery (RCA) with calcium modification and intravascular imaging (IVI).
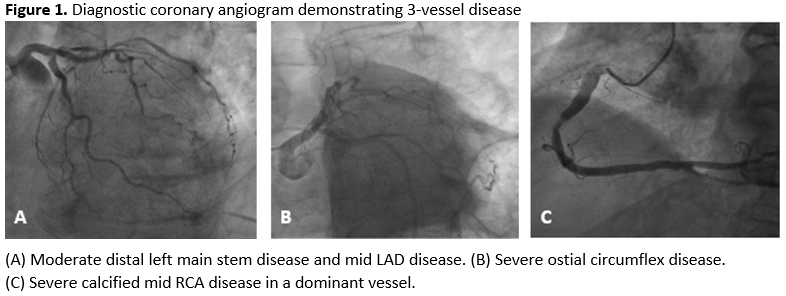
 Figure 1c Pre RCA.mov
Figure 1c Pre RCA.mov
Pre RCA RAO View.mov
Relevant Test Results Prior to Catheterization
There was a mild troponin elevation of 52 ng/mL. Diagnostic angiography showed moderate disease in the left coronary system (Figure 1a & 1b). A Heart Team discussion was undertaken with a decision to perform PCI to the severe culprit RCA lesion (Figure 1c) using calcium modification and IVI, with a right radial artery approach and a 7F AL 1.0 guide catheter.
Relevant Catheterization Findings
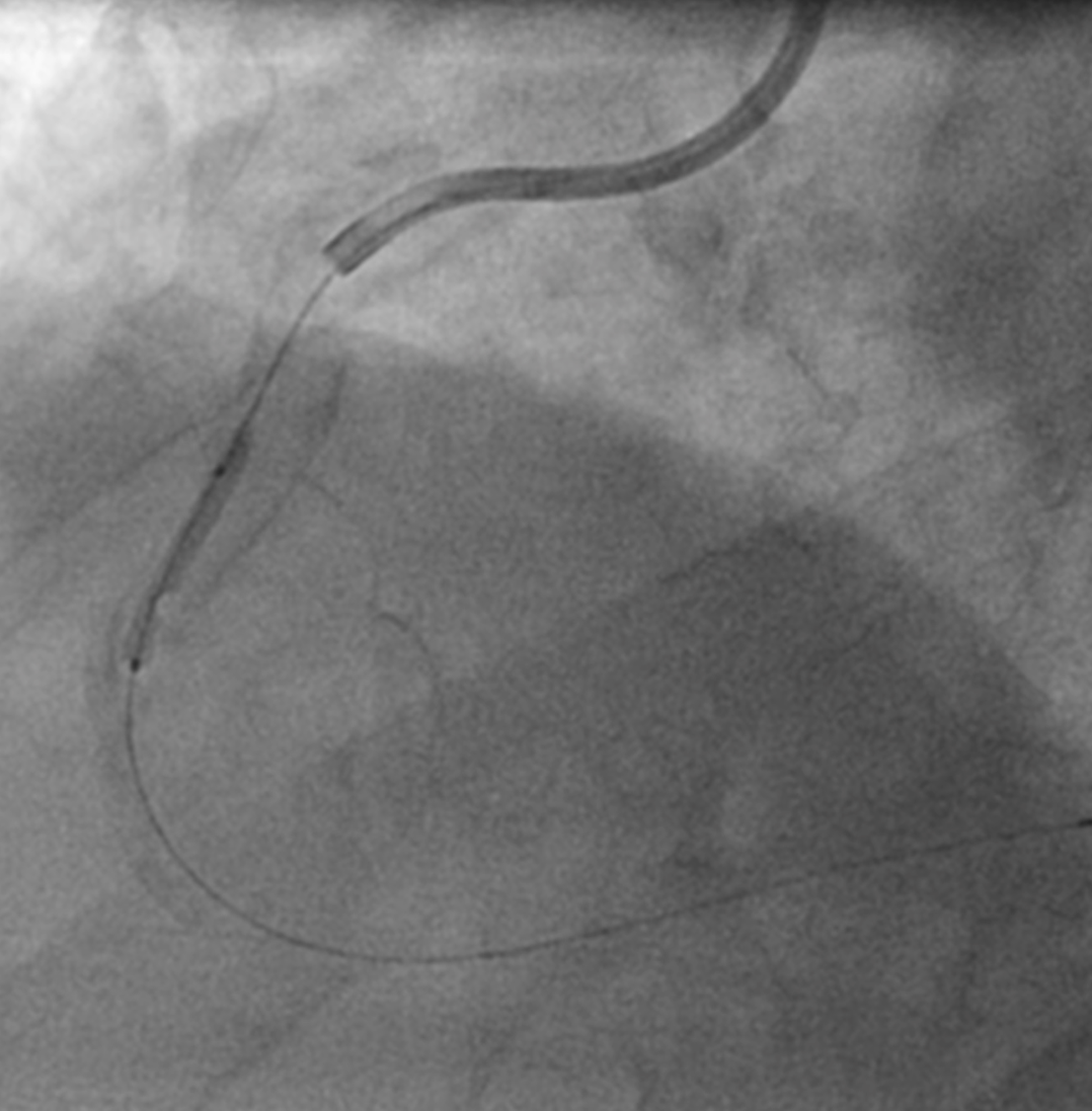
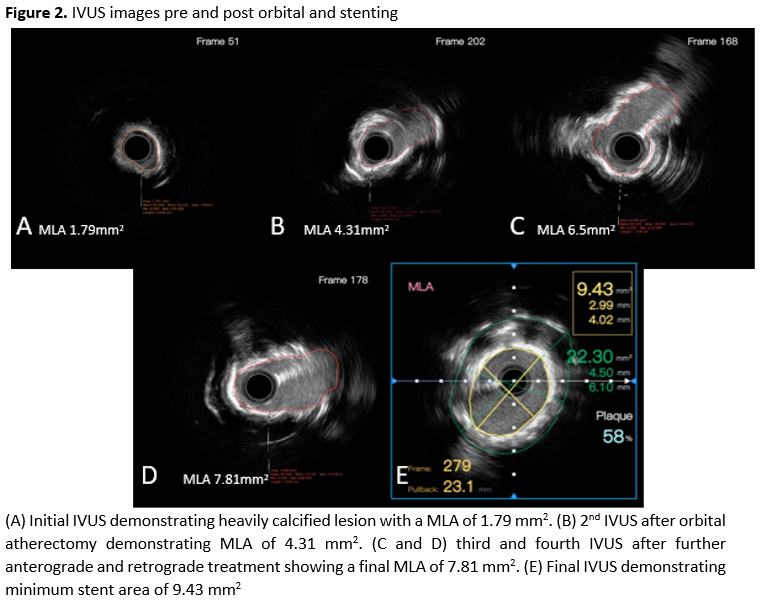
A Sion Blue wire was passed and pre-dilated with a 2.0/20 mm Ryurei balloon, showing clear underexpansion. Intravasular ultrasound (IVUS) showed severe circumferential calcification and a minimal luminal area (MLA) of 1.79 mm2 (Figure 2a). Because the lesion was balloon-crossable with a favourable wire bias, orbital atherectomy (OA) was deemed appropriate. A Cardiac Physiologist expert in IVI performed all the IVUS measurements to guide calcium-modification, as is often the workflow in our cases
First IVUS MLA 1.79mm.mpg
Interventional Management
Procedural Step
OA was performed at low speed and was tolerated well by the patient. Subsequent IVUS demonstrated an improvement in MLA to 4.31 mm2 (Figure 2b). Two further runs (both low and high speed in antegrade and retrograde direction) were performed with IVUS assessment undertaken after each run. There was a further increase in MLA with calcium fractures seen on IVUS (Figure 2c & 2d). The lesion was then modified with a 4.00 mm non-compliant (NC) balloon prior to deployment of a 5.00 x 24 mm Megatron stent, which was post-dilated with a 4.50 mm NC balloon. The final angiographic result was satisfactory. The final IVUS showed good stent apposition, no edge dissection, and a minimal stent area (MSA) of 9.43 mm2 (Figure 2E).
2nd IVUS MLA 4.31mm.mov
POST IVUS RUN MLA 9.43.mpg
RCA Post PCI angio.mpg
Case Summary
This case showed the importance of IVI to help choose the appropriate modality to safely modify severe calcification. Assessment with IVUS after every OA showed modification of calcium in real-time. Perhaps the most important point of this case was demonstrating the positive impact of involving cath lab staff in the decision making process during IVI. This fosters and environment of open discussion and enables staff to become more involved in the case, and ultimately develop the expertise to independently interpret intravascular images and advise the operator, even in complex cases. This approach supports the operator and leads to improved workflow and patient outcomes.