Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_019
Dressler's Syndrome: Rare?
By Swee En Goay, Wei Liang Lee, Afif Ashari, Chee Kiang Teoh
Presenter
Swee En Goay
Authors
Swee En Goay1, Wei Liang Lee1, Afif Ashari1, Chee Kiang Teoh1
Affiliation
National Heart Institute, Malaysia1
View Study Report
CASE20251114_019
Coronary - Imaging & Physiology - Non-Invasive Imaging (CTA, MRI, Echo, etc)
Dressler's Syndrome: Rare?
Swee En Goay1, Wei Liang Lee1, Afif Ashari1, Chee Kiang Teoh1
National Heart Institute, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
68 years old lady presented with worsening reduced effort tolerance past 3 weeks in NYHA III associated with intermittent chest tightness. She had NSTEMI in October 2024 at a district hospital. She has Hypertension, Diabetes and Dyslipidaemia on medications. She was afebrile with HR 87 bpm, BP 142/96mmHg, SpO2 96%(RA). On auscultation, she has muffled heart sound with reduced air entry.
Relevant Test Results Prior to Catheterization
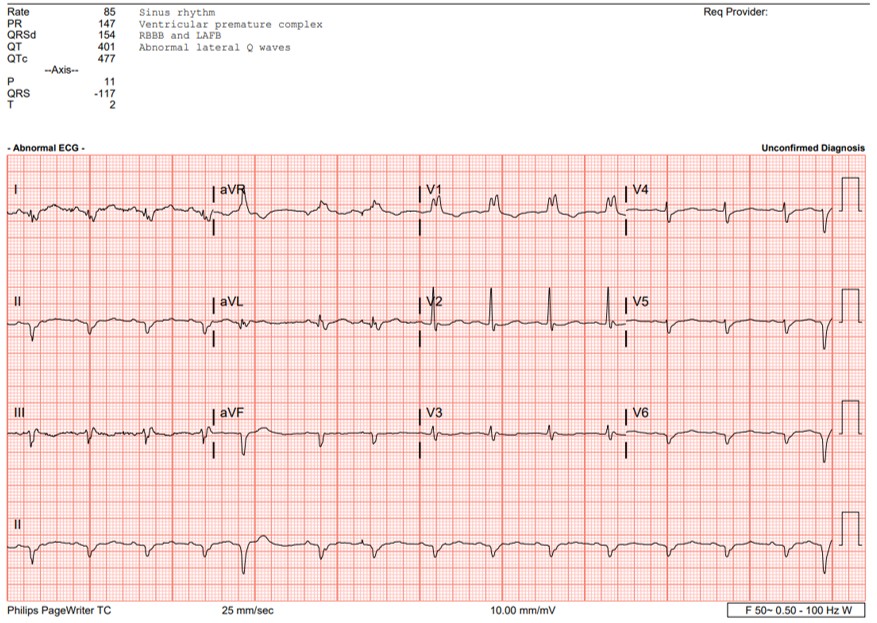
ECG showed sinus rhythm, RBBB with small QRS complexes. Her laboratory workup including full blood count and metabolic panel was unremarkable with Troponin recorded at 13pg/ml. Chest XRay showed cardiomegaly. Urgent echocardiogram showed ejection fraction of 45% with global pericardial effusion with right ventricular collapse during diastole. Emergency pericardial tapping was done with 480cc serous fluid drained, repeated echocardiogram showed near total resolved pericardial effusion.

 A4C.mp4
A4C.mp4
Relevant Catheterization Findings
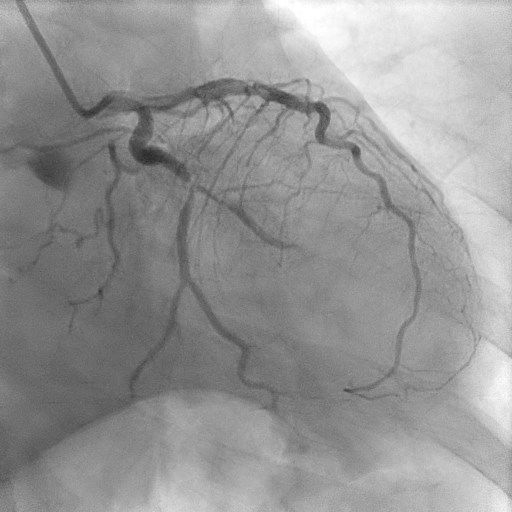
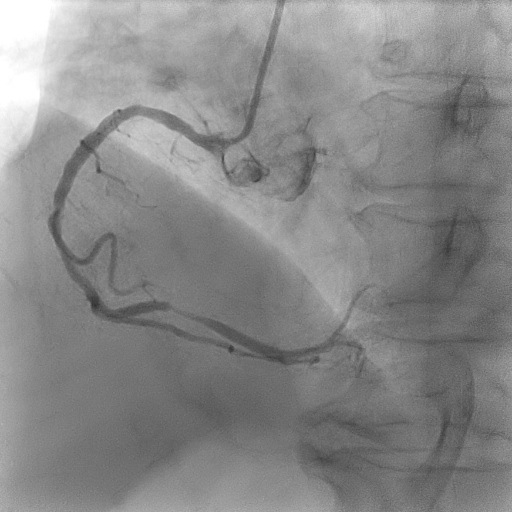
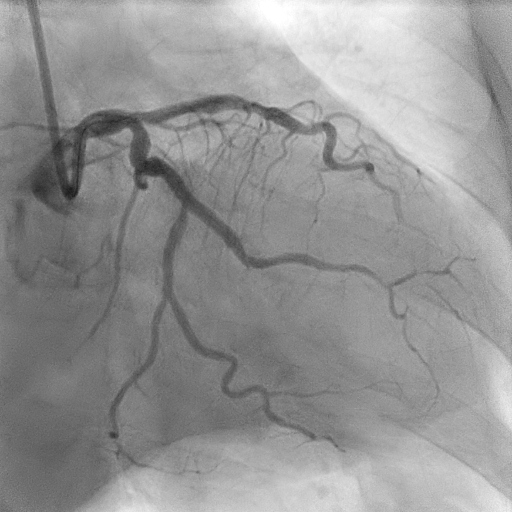
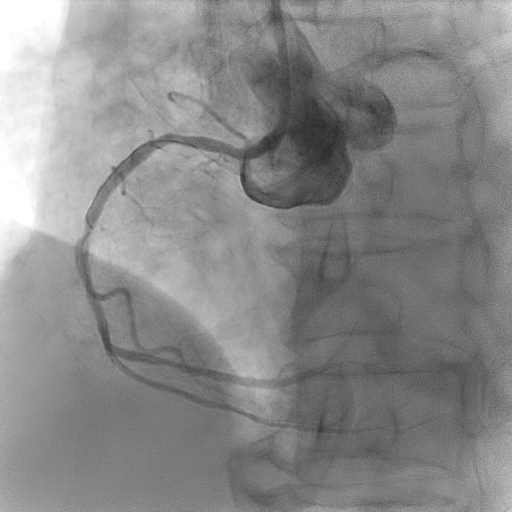
Coronary angiogram showed two vessel disease with severe stenosis at the obtuse marginal (OM), distal left circumflex (LCx) artery and distal right coronary artery (RCA) with mild disease at the proximal left anterior descending artery (LAD).
LCx before.mpg
RCA before.mpg
Interventional Management
Procedural Step
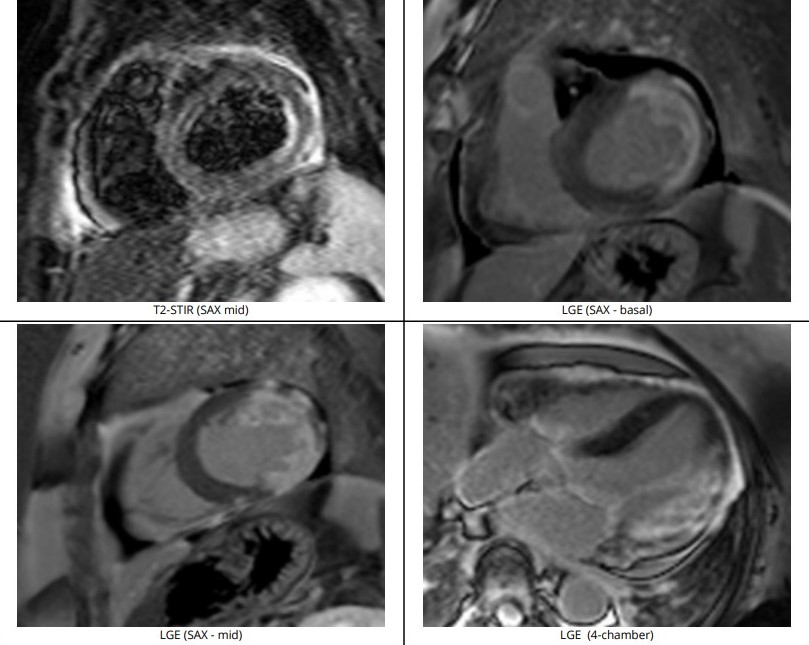
Using guide EBU 3.0/6Fr, RTF crossed lesion OM and predilated with SC 2.0/12mm 8-12atm, then Scoreflex 2.5/15mm upto 20atm. DCB (distal LCx) with Agent 2.5/20mm at 8atm then DES (OM) with Synergy 2.5/24mm at 11atm followed by postdilatation using NC 2.75mm at12-20atm. Using guide JR 3.5/6F, coronary wire RTF to distal RCA, sequential predilatation with SC 2.0/12mm at 10-12atm then Wedge 2.5/15mm at 16-18atm. DCB with Pantera Lux 2.5/20mm at 8atm. Final angiogram showed TIMI III Flow, No dissection. Further evaluation with Cardiac MRI showed increased pericardial signal at the mid-apical lateral wall and part of the mid anterior wall on STIR-T2 study. In the late phase of gadolinium study, there is near transmural enhancement of the basal-apical lateral wall, partially extending into the inferior wall. The overall findings are in keeping with ischaemic cardiomyopathy, complicated with pericardial effusion and mild pericardial effusion and inflammation likely related to Dressler’s Syndrome.
RCA FINAL.mpg
LCx FINAL.mpg
Case Summary
Dressler syndrome 6 months after a myocardial infarction is quite rare but not impossible, especially if revascularization is delayed which could have prolonged the inflammatory response. In this case, the delayed revascularization, may have exacerbated the inflammatory response, contributing to the development of pericardial effusion. The patient's emergency pericardiocentesis for tamponade was crucial, further assessment with cardiac MRI confirmed the diagnosis of Dressler Syndrome. This case highlights the importance of maintaining a high clinical suspicion, even in uncommon scenarios, to manage potentially life-threatening complications like cardiac tamponade in Dressler Syndrome.