Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_018
Leave-Nothing-Behind Strategy for RCA ISR-CTO: IVUS-Guided DCB-Only Revascularization in HFrEF
By Daniel Eng Theng Sheng, Noor Muhammad Azlan Shah Bin Atan, Hafidz Bin Abd Hadi
Presenter
Daniel Eng Theng Sheng
Authors
Daniel Eng Theng Sheng1, Noor Muhammad Azlan Shah Bin Atan1, Hafidz Bin Abd Hadi1
Affiliation
Institut Jantung Negara (IJN), Malaysia1
View Study Report
CASE20251114_018
Coronary - Complex PCI - In-Stent Restenosis
Leave-Nothing-Behind Strategy for RCA ISR-CTO: IVUS-Guided DCB-Only Revascularization in HFrEF
Daniel Eng Theng Sheng1, Noor Muhammad Azlan Shah Bin Atan1, Hafidz Bin Abd Hadi1
Institut Jantung Negara (IJN), Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
A 68-year-old man with hypertension, dyslipidemia, prior RCA DES (2017) and ischemic cardiomyopathy presented with progressive exertional angina. He reported no rest pain or decompensated heart failure symptoms. On examination, he was haemodynamically stable with clear lung fields, normal heart sounds, and no peripheral oedema or clinical evidence of congestion.
 1.avi
1.avi
3.avi
4.avi
Relevant Test Results Prior to Catheterization
ECG showed sinus rhythm with non-specific ST-T changes. Echocardiography demonstrated LVEF 35% with inferior wall hypokinesia. SPECT stress imaging revealed moderate inducible inferior ischemia. Coronary CT indicated severe mid-RCA in-stent restenosis with possible CTO. Routine blood tests were unremarkable.
5.avi
6.avi
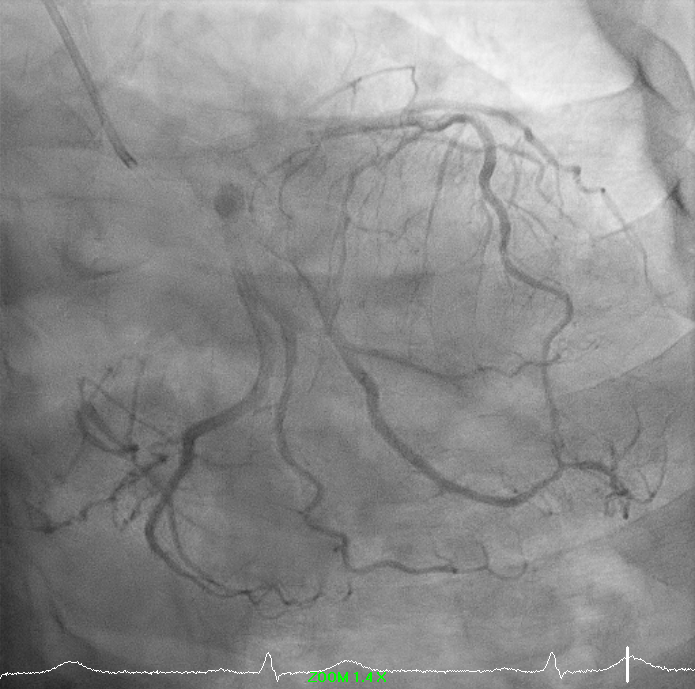
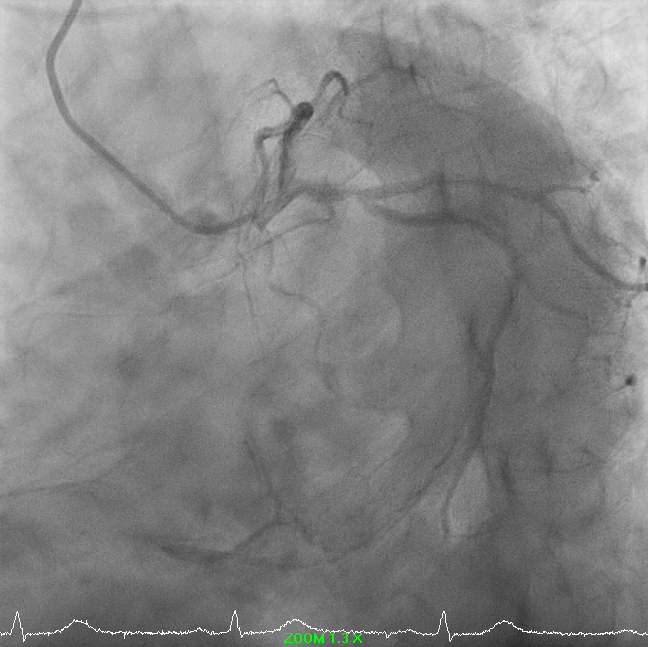
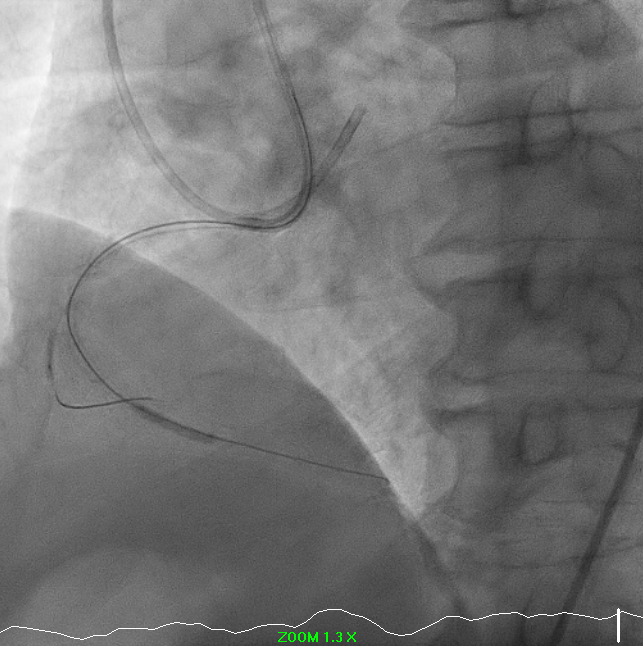
Relevant Catheterization Findings
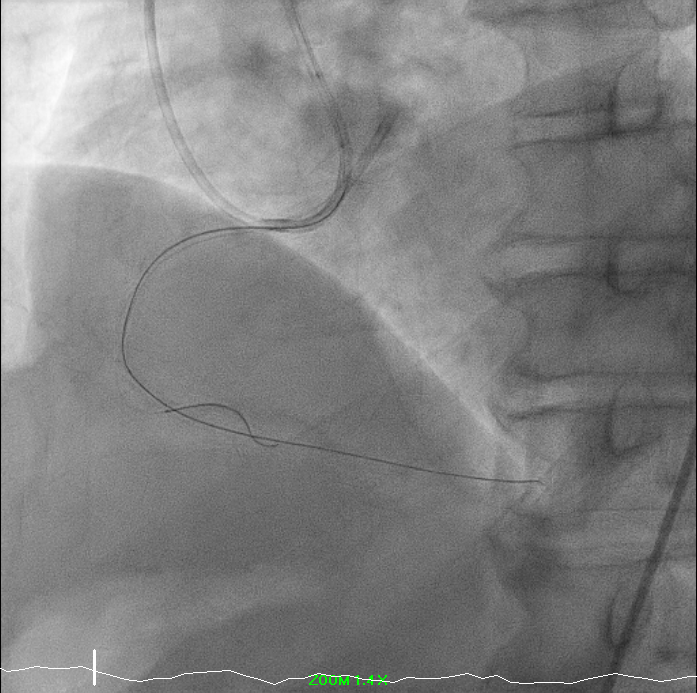
Right-dominant system. Proximal LAD shows 50% moderate calcified disease. Proximal LCx has 50% stenosis with severe calcification. RCA demonstrates severe diffuse proximal–mid 70% stenosis with moderate calcification and distal severe ISR-CTO with heavy calcification and minimal antegrade flow. Impression: Complex RCA ISR-CTO as culprit with moderate pLAD/pLCx disease.
8.avi
9.avi
11.avi
Interventional Management
Procedural Step
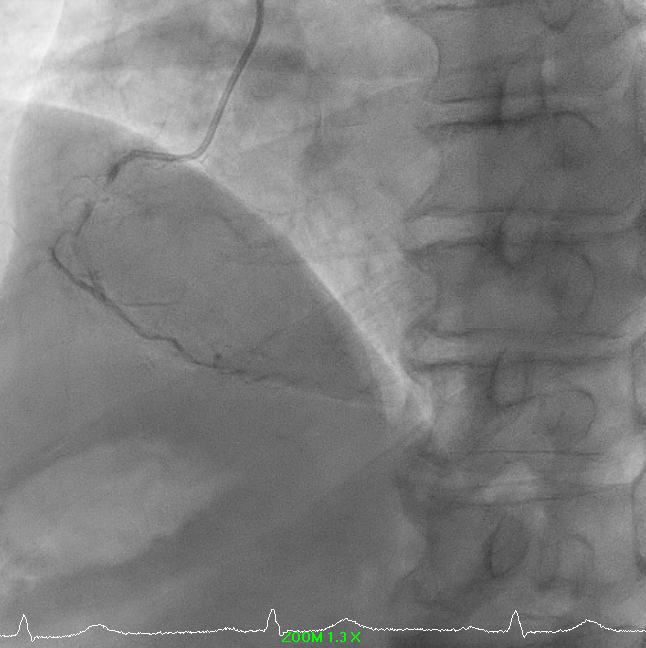
PCI to RCA CTO ISR: A PCI was performed for RCA chronic total occlusion in-stent restenosis (ISR) in a patient with ischemic cardiomyopathy, reduced LVEF, and moderate inducible ischemia. Femoral access was obtained using EBU (USG-guided, single attempt) and RRA 7F exchange. Initial crossing attempt with Corsair Pro XS/Fielder XTR failed; the lesion was successfully crossed using Fielder XTA, confirmed by retrograde angiography. Microcatheter was removed using the balloon trapping technique.
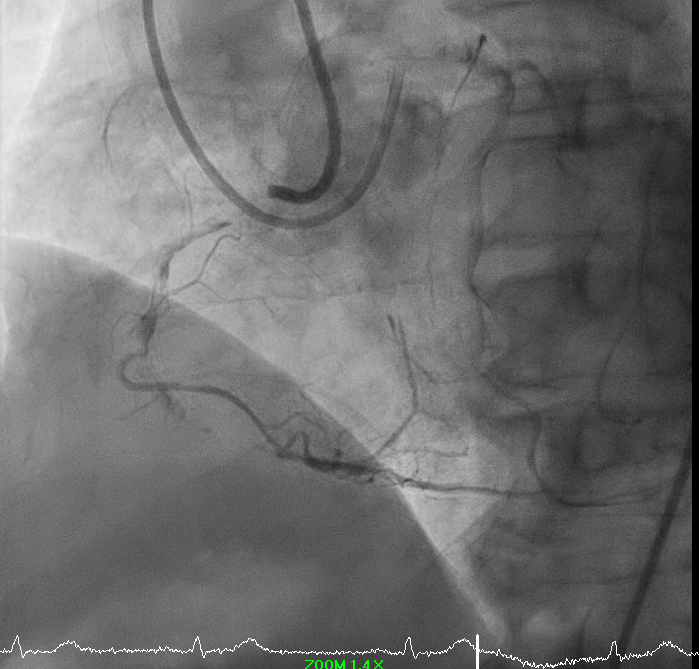
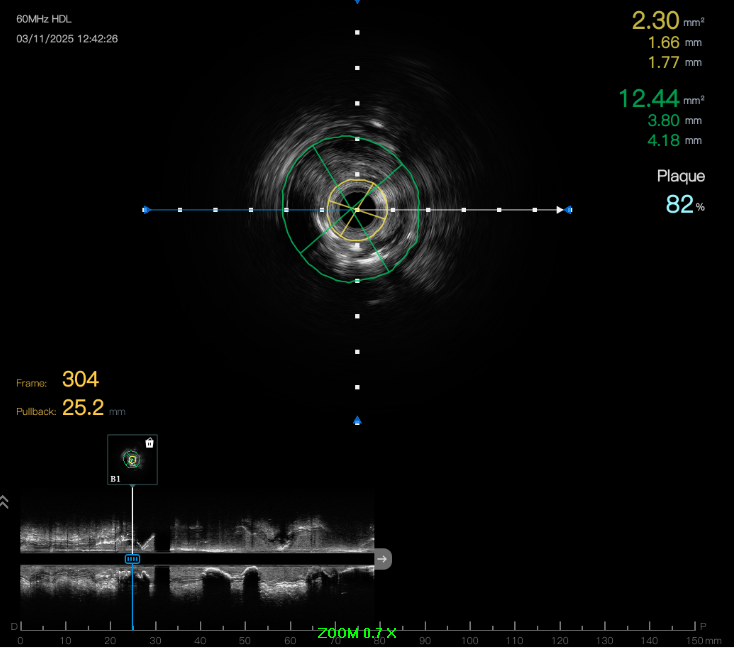
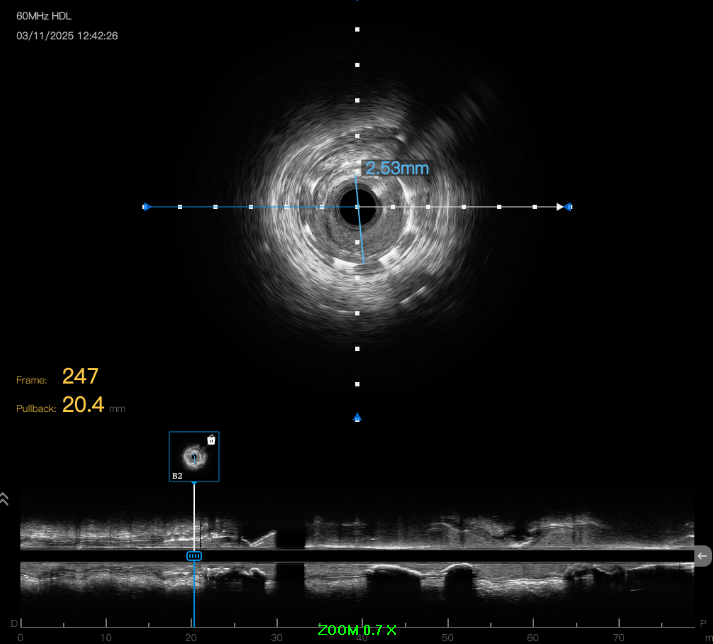
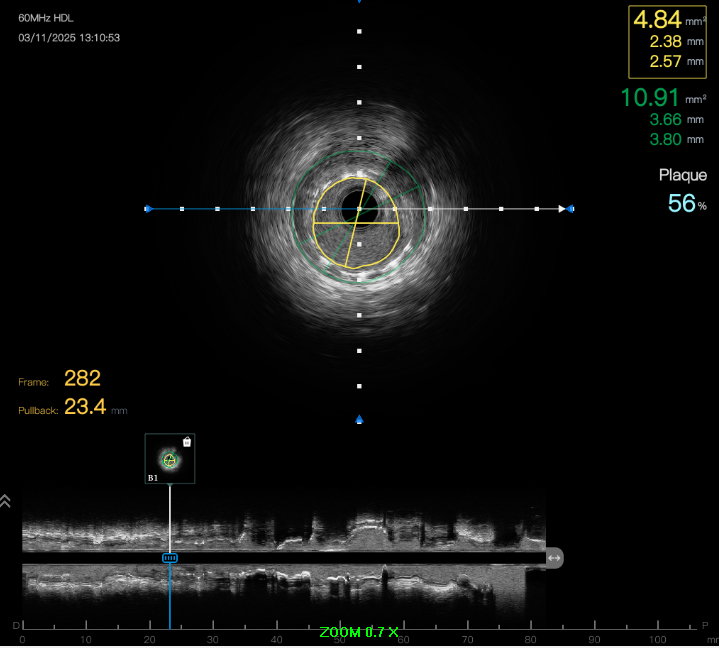
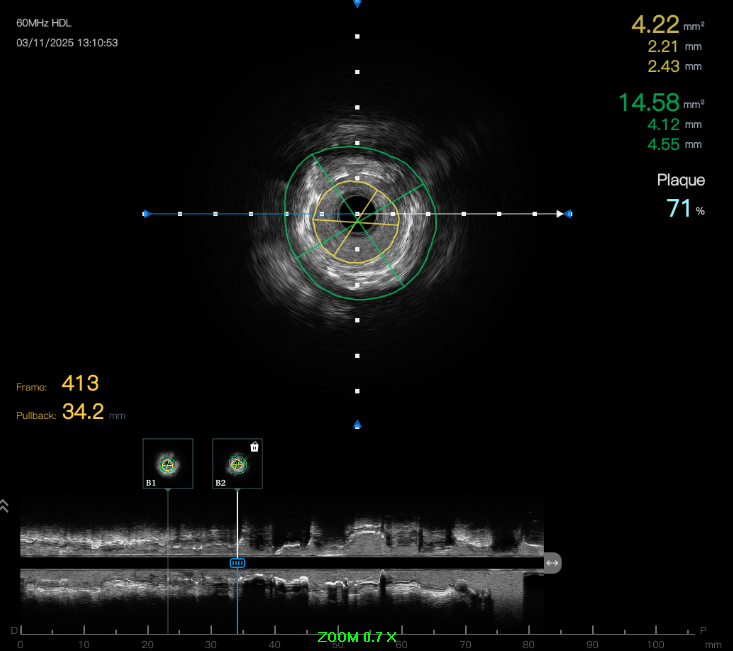
Predilation was challenging due to poor support. Initial 0.75 mm balloon could not pass; support was augmented with Sion Blue to RV branch. Subsequent predilation was performed sequentially with Zinrai 0.75 × 4 mm, Ryureo 1.0 × 5 mm, and NC balloon 2.0 × 15 mm, achieving satisfactory antegrade flow. IVUS assessment demonstrated a distal vessel diameter of 2.5 mm, proximal/mid 3.5 mm, previous MSA 3.5 mm, and 360° proximal calcium. Additional predilation using Wedge 2.5 × 15 mm (distal→proximal) and Scoreflex 3.0 × 15 mm (mid→proximal) resulted in <30% recoil and no dissection. Post-IVUS, MSA improved from 3.5 → 4.8 mm.
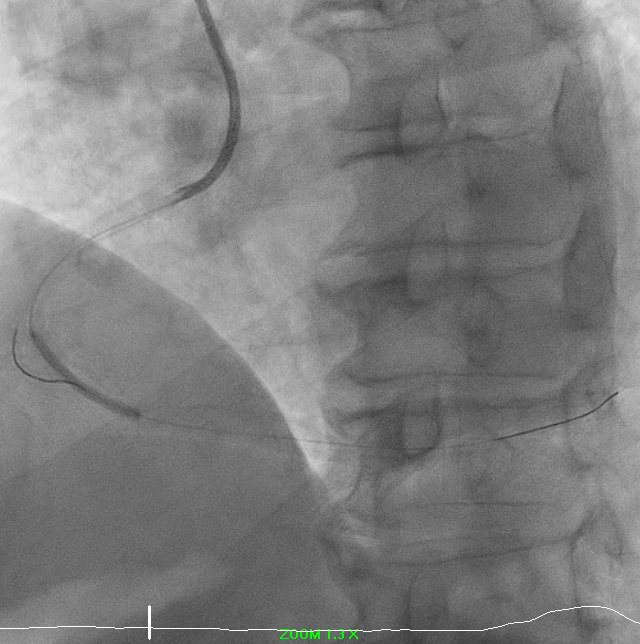
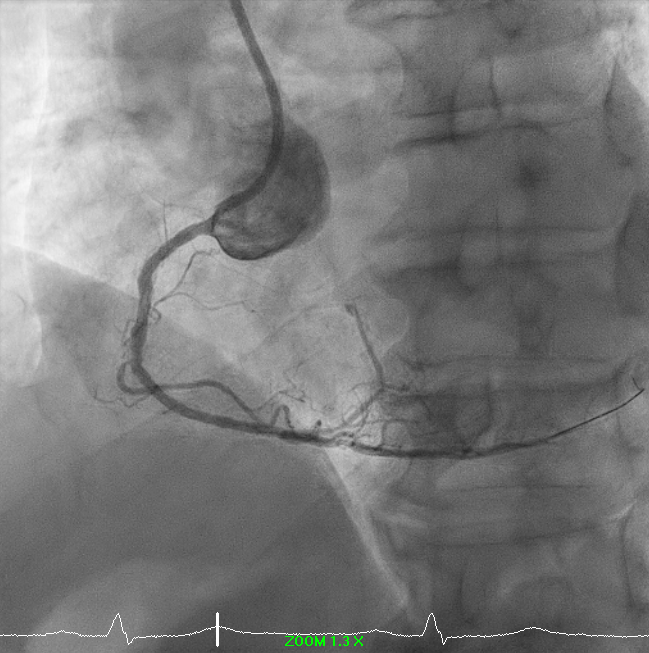
A drug-coated balloon strategy was employed: Prevail 2.5 × 30 mm @ 8 ATM × 60s and Selution SLR 3.0 × 35 mm @ 6 ATM × 60s. Final angiography showed TIMI 3 flow with no residual dissection. The case highlights a complex RCA ISR-CTO managed successfully with a contemporary DCB-based, stent-less strategy guided by IVUS and meticulous lesion preparation.
12.avi
13.avi
Predilation was challenging due to poor support. Initial 0.75 mm balloon could not pass; support was augmented with Sion Blue to RV branch. Subsequent predilation was performed sequentially with Zinrai 0.75 × 4 mm, Ryureo 1.0 × 5 mm, and NC balloon 2.0 × 15 mm, achieving satisfactory antegrade flow. IVUS assessment demonstrated a distal vessel diameter of 2.5 mm, proximal/mid 3.5 mm, previous MSA 3.5 mm, and 360° proximal calcium. Additional predilation using Wedge 2.5 × 15 mm (distal→proximal) and Scoreflex 3.0 × 15 mm (mid→proximal) resulted in <30% recoil and no dissection. Post-IVUS, MSA improved from 3.5 → 4.8 mm.
A drug-coated balloon strategy was employed: Prevail 2.5 × 30 mm @ 8 ATM × 60s and Selution SLR 3.0 × 35 mm @ 6 ATM × 60s. Final angiography showed TIMI 3 flow with no residual dissection. The case highlights a complex RCA ISR-CTO managed successfully with a contemporary DCB-based, stent-less strategy guided by IVUS and meticulous lesion preparation.
Case Summary
IVUS-guided DCB-only PCI is a safe and effective ‘leave-nothing-behind’ strategy for ISR-CTO, minimizing further stent layering while promoting vessel healing. Meticulous lesion preparation and intravascular imaging are crucial for optimal luminal expansion, procedural success, and potentially improved long-term outcomes.
Learning points: 1. IVUS-guided DCB-only PCI is safe and effective with adequate lesion preparation. 2. ‘Leave-nothing-behind’ minimizes risks from multiple stent layers. 3. IVUS ensures precise assessment, optimized treatment, and durable outcomes.
Learning points: 1. IVUS-guided DCB-only PCI is safe and effective with adequate lesion preparation. 2. ‘Leave-nothing-behind’ minimizes risks from multiple stent layers. 3. IVUS ensures precise assessment, optimized treatment, and durable outcomes.