Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_015
Redressing the Relentless Restenosis: A Minimalistic Approach to Recurrent Stent Failure
By Nancy Virginia, Kai Soon Liew, Huan Yean Kang, Chai Yih Tan, Vijayendran Rajalingam, Prabahkar Subramaniam, Kenneth Kay Leong Khoo, Mohd Khairi Othman, Aditya Fahmi Prianda, Christian Sunur, Pirevina Naidu, MN Azalizam Abdullah, Nurul Syifaa Najwa Nadzri, Muhammad Anis bin Abdul Aziz, Saravanan Krishinan, Kantha Rao Narasamuloo, Chee Tat Liew, Wirash Kehasukcharoen, Anek Kanoksilp, Dharmaraj Karthikesan
Presenter
Nancy Virginia
Authors
Nancy Virginia1, Kai Soon Liew1, Huan Yean Kang1, Chai Yih Tan1, Vijayendran Rajalingam1, Prabahkar Subramaniam1, Kenneth Kay Leong Khoo1, Mohd Khairi Othman1, Aditya Fahmi Prianda1, Christian Sunur1, Pirevina Naidu1, MN Azalizam Abdullah1, Nurul Syifaa Najwa Nadzri1, Muhammad Anis bin Abdul Aziz1, Saravanan Krishinan1, Kantha Rao Narasamuloo1, Chee Tat Liew2, Wirash Kehasukcharoen3, Anek Kanoksilp3, Dharmaraj Karthikesan1
Affiliation
Hospital Sultanah Bahiyah, Malaysia1, Hospital Pantai, Malaysia2, Central Chest Institute of Thailand, Thailand3
View Study Report
CASE20251114_015
Coronary - Complex PCI - In-Stent Restenosis
Redressing the Relentless Restenosis: A Minimalistic Approach to Recurrent Stent Failure
Nancy Virginia1, Kai Soon Liew1, Huan Yean Kang1, Chai Yih Tan1, Vijayendran Rajalingam1, Prabahkar Subramaniam1, Kenneth Kay Leong Khoo1, Mohd Khairi Othman1, Aditya Fahmi Prianda1, Christian Sunur1, Pirevina Naidu1, MN Azalizam Abdullah1, Nurul Syifaa Najwa Nadzri1, Muhammad Anis bin Abdul Aziz1, Saravanan Krishinan1, Kantha Rao Narasamuloo1, Chee Tat Liew2, Wirash Kehasukcharoen3, Anek Kanoksilp3, Dharmaraj Karthikesan1
Hospital Sultanah Bahiyah, Malaysia1, Hospital Pantai, Malaysia2, Central Chest Institute of Thailand, Thailand3
Clinical Information
Relevant Clinical History and Physical Exam
A 63-year-old man with hypertension, diabetes, dyslipidemia, and a history of smoking had multiple admissions for unstable angina since 2015. Physical examination during the current admission was unremarkable, with no signs of heart failure. Left ventricular systolic function remained normal throughout his clinical course.
Relevant Test Results Prior to Catheterization
Angiography in 2015 showed severe proximal LAD and subtotal mid-RCA lesions, both stented. In 2019, he developed inferior STEMI; angiography revealed patent LAD stent and very late distal RCA stent thrombosis, treated with DCB. On current presentation, echocardiography showed normal LVEF, and noninvasive tests suggested recurrent inferior ischemia.
Relevant Catheterization Findings
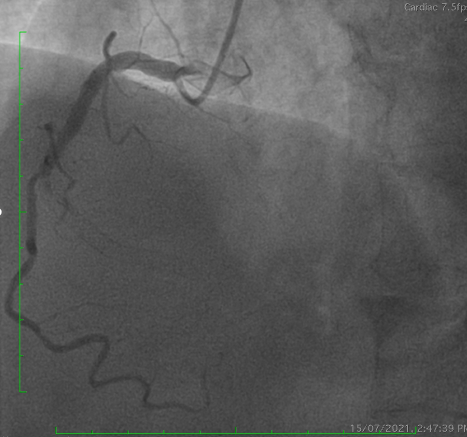
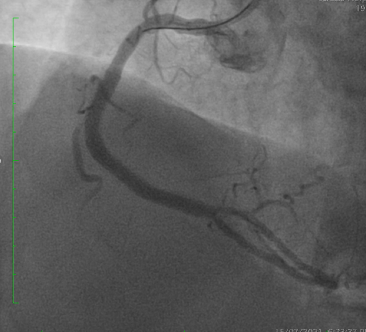
Coronary angiography demonstrated a patent LAD stent and CTO in-stent restenosis (ISR) at mid RCA with ipsilateral collateral flow from the RV branch to the PDA. Anatomical challenges included a proximal RV branch near the CTO cap, a nearly 90° CTO entry angle, a lesion length of ~60 mm, and distal bifurcation involvement. The CTO had a tapered stump with a visible microchannel. The J-CTO score was 2.


Interventional Management
Procedural Step
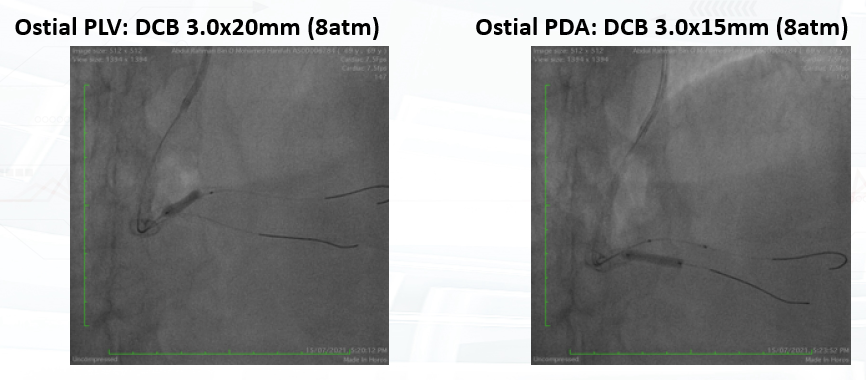
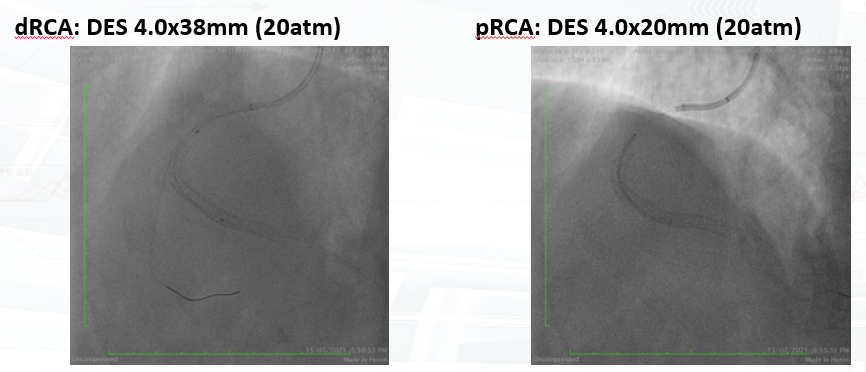
PCI was performed via single radial access with a 6F short-tip AL guiding catheter and Finecross microcatheter. 3D wiring with UB3 under orthogonal views; escalation to Gaia 3. Anchor ballooning in the RV branch improved support. The wire successfully crossed into the PLV. Predilation with a small balloon, followed by scoring ballooning. A Crusade dual-lumen catheter enabled Gaia 3 wiring into the PDA, which was predilated with a 2.5 mm balloon. IVUS revealed undersized and extensively malapposed stents contributing to ISR and prior very late thrombosis. High-pressure NC 3.75 mm ballooning improved expansion, though full correction was limited by the original stent size. A hybrid treatment strategy was chosen—DCB for both PLV and PDA (3.0×20 mm and 3.0×15 mm respectively, with DCB-assisted kissing), and DES reconstruction of the mid-to-proximal RCA using 4.0×38 mm and 4.0×20 mm stents delivered with guide extension support. Final IVUS confirmed optimal expansion and apposition without edge dissection. Final angiography showed TIMI 3 flow with no complications. At 9 months, angiography demonstrated patent RCA stents and positive remodeling at the PLV ostium.
Case Summary
This case illustrates that well-planned antegrade CTO-ISR PCI through single radial access can achieve successful revascularization in complex restenotic anatomy. Maintaining the guidewire within the stent architecture is crucial when treating ISR-related CTOs. Intravascular imaging plays a pivotal role in identifying the mechanism of stent failure—here, significant malapposition and undersizing. Adequate lesion preparation is essential before DCB therapy, and a DCB–DES combination can be an effective strategy for complex bifurcation ISR while minimizing additional metal burden.