Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_013
Overcoming an Ambiguous Proximal Cap in a Long Femoropopliteal CTO Using Retrograde Guidance and BeBack-Assisted Cap Penetration
By Fadhil Pratama Apriansyah, Suci Indriani
Presenter
Fadhil Pratama Apriansyah
Authors
Fadhil Pratama Apriansyah1, Suci Indriani1
Affiliation
National Cardiovascular Center, Harapan Kita, Indonesia1
View Study Report
CASE20251114_013
Endovascular - Iliac / SFA Intervention
Overcoming an Ambiguous Proximal Cap in a Long Femoropopliteal CTO Using Retrograde Guidance and BeBack-Assisted Cap Penetration
Fadhil Pratama Apriansyah1, Suci Indriani1
National Cardiovascular Center, Harapan Kita, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A 65-year-old male presented with worsening left leg pain for one week and a chronic non-healing ulcer for two months. Examination revealed a cool, tender limb with distal ulceration. The WIfI classification was 2-3-2, indicating high amputation risk. Past medical history included chronic heart failure (EF 28%), coronary artery disease, and chronic kidney disease (eGFR 41 mL/min/1.73 m²). Cardiovascular risk factors included hypertension, diabetes mellitus, dyslipidemia, and ex-smoker.

Relevant Test Results Prior to Catheterization
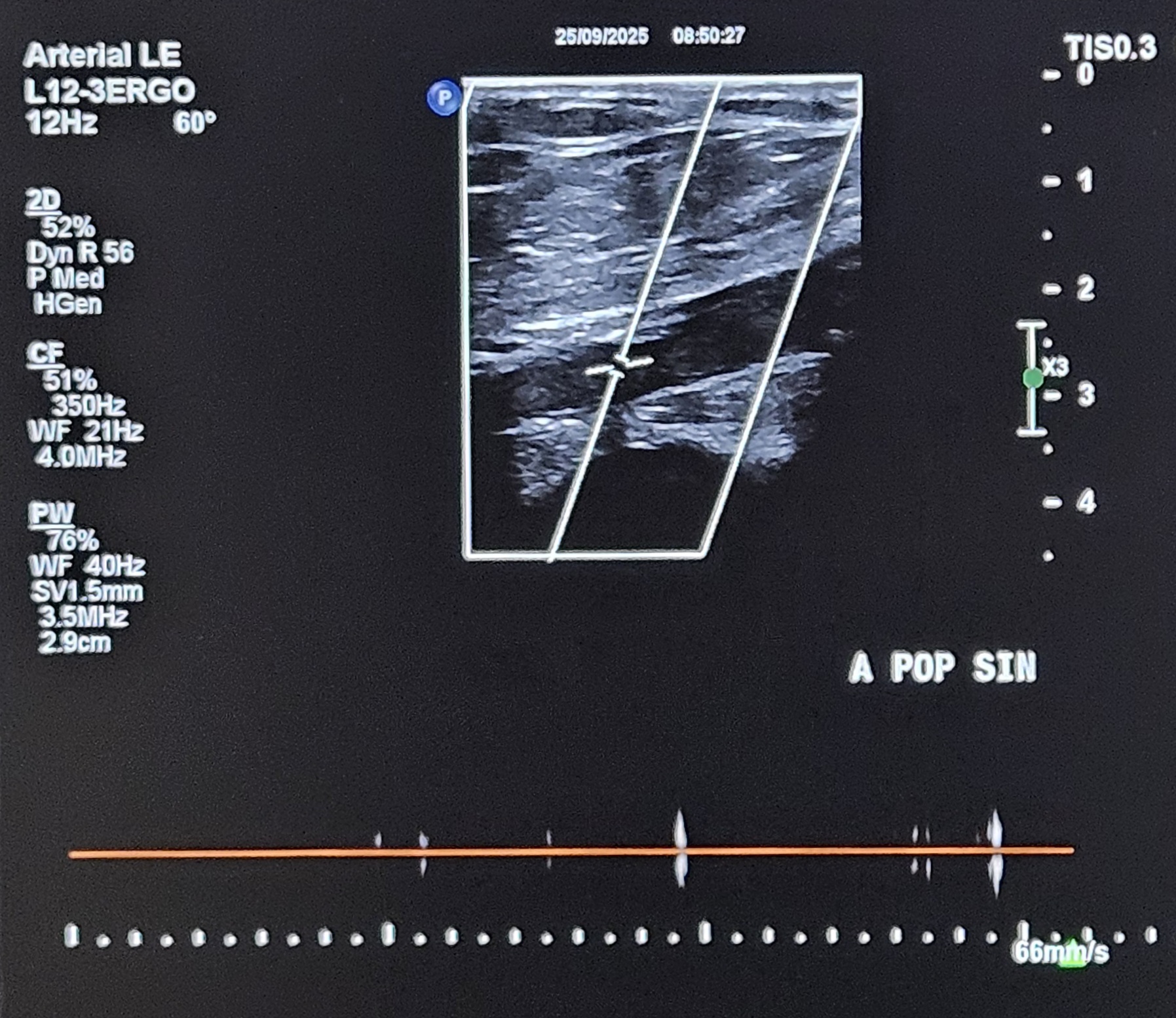
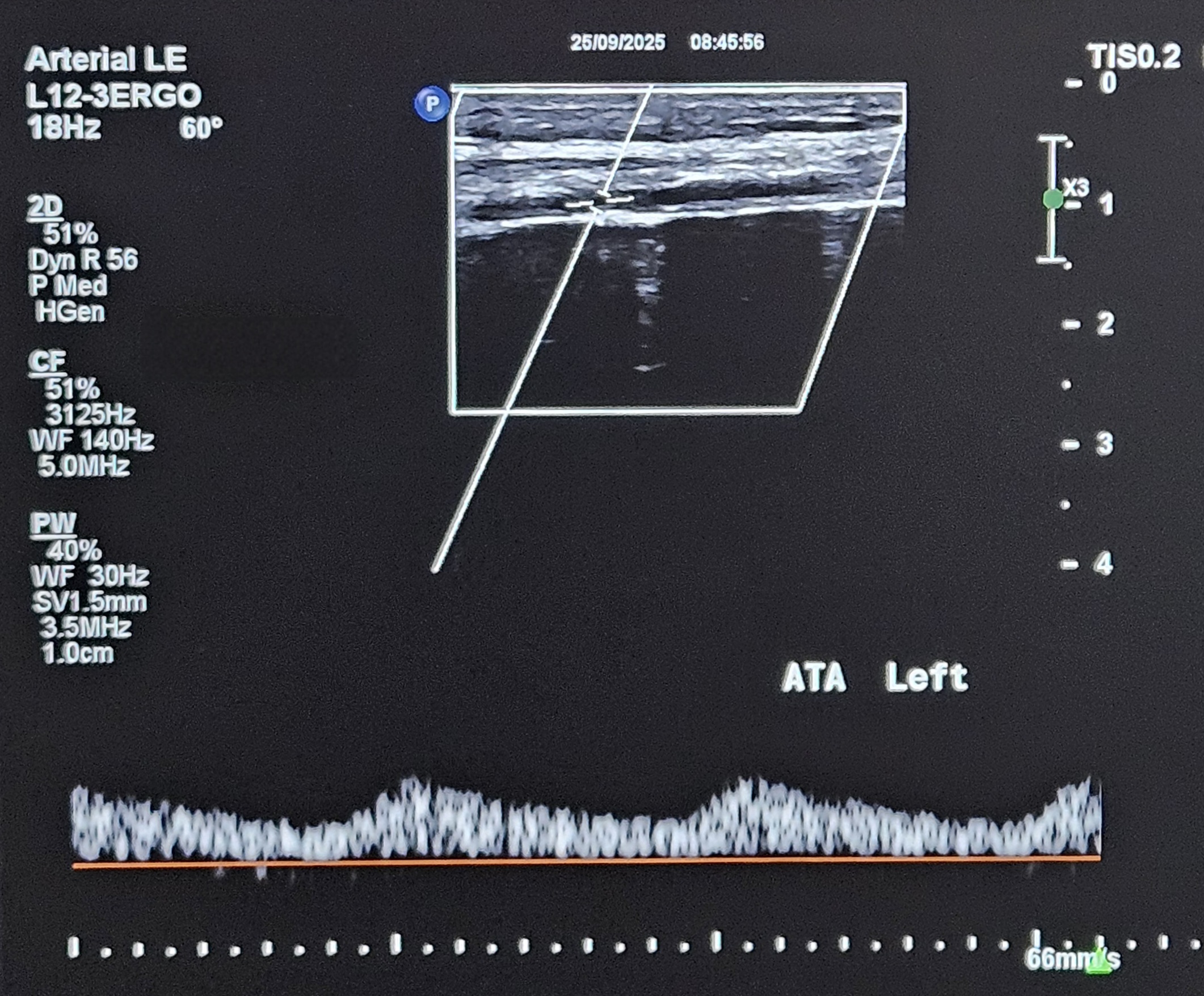
Doppler ultrasound demonstrated triphasic waveform at the left common femoral artery and biphasic flow at the mid superficial femoral artery (SFA). There was total occlusion from the distal SFA to the distal popliteal artery, with monophasic high end-diastolic flow at the anterior tibial artery (ATA), consistent with severe infra-popliteal ischemia.
Relevant Catheterization Findings
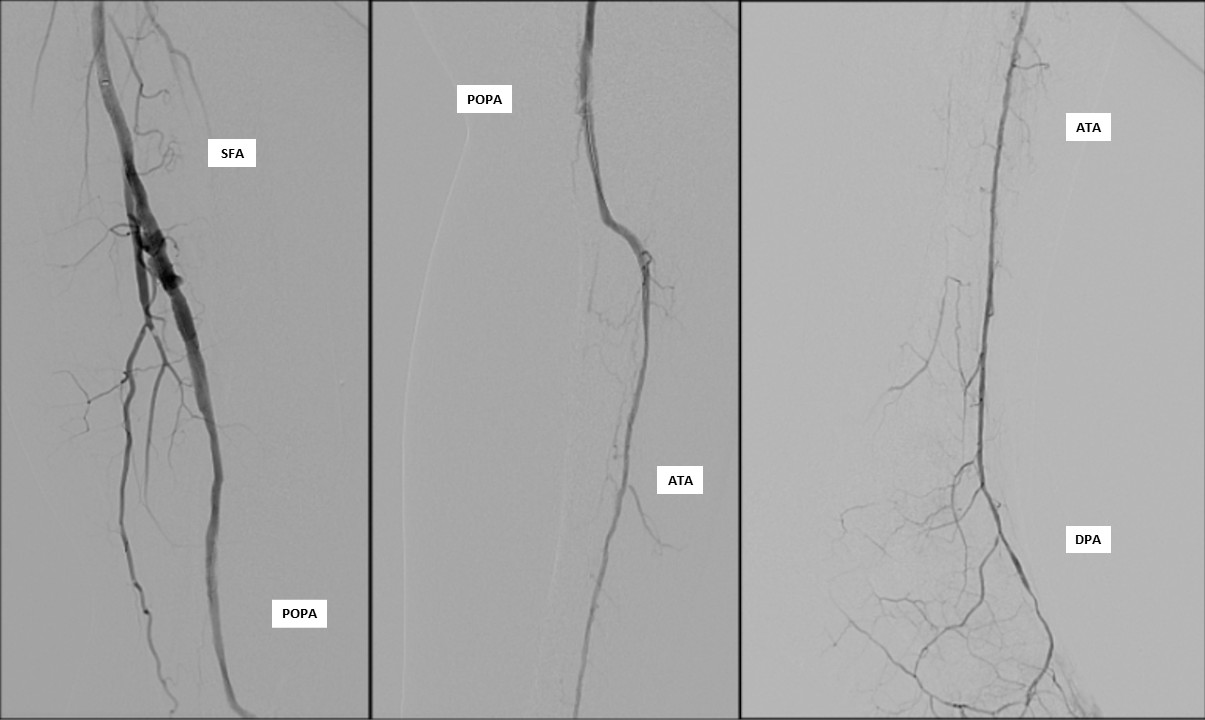
Diagnostic arteriography showed total occlusion of the distal SFA with poor distal runoff. Reconstitution was identified only at the distal ATA as the single suitable target vessel.


 Angio Video.mp4
Angio Video.mp4
Interventional Management
Procedural Step
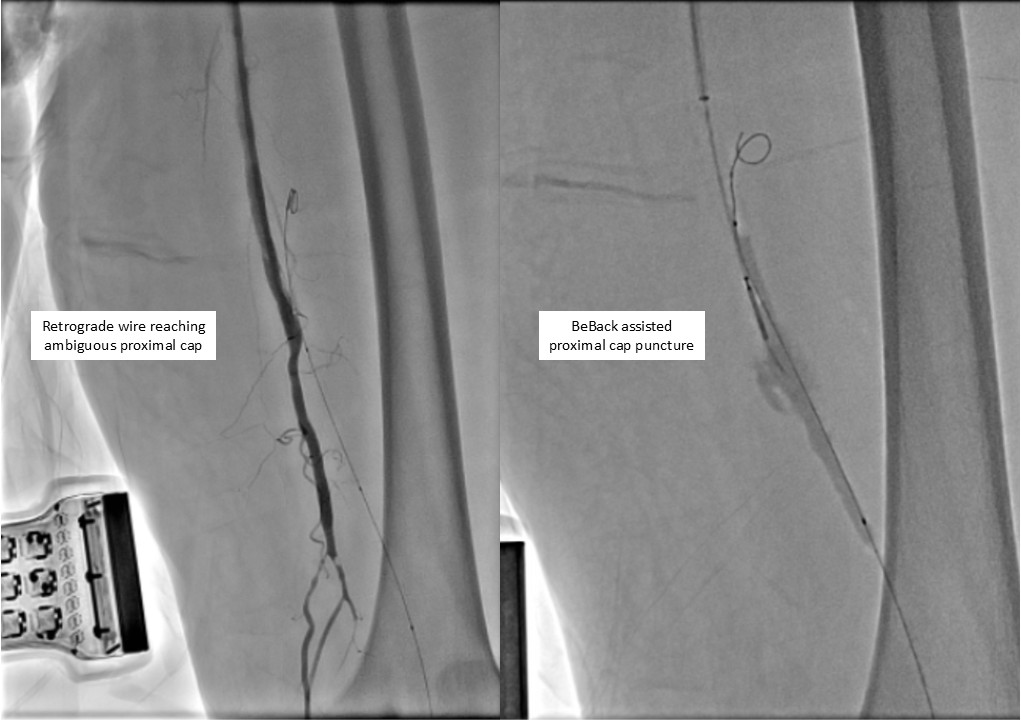
Antegrade puncture was performed, and a microcatheter with a Command 14 guidewire (Abbott Vascular, Santa Clara, CA, USA) was advanced toward the distal SFA but failed to cross because the proximal cap was misidentified due to its blunt and ambiguous appearance. The wire entered aside branch that ran parallel to the true SFA–popliteal course. Given the long chronic total occlusion (CTO) segment and uncertain vessel path, a retrograde approach was pursued to overcome this anatomical ambiguity. Distal ATA access was gained and a CXI Support Catheter (Cook Medical, Bloomington, IN, USA) with a V-18 Guidewire (Boston Scientific, Marlborough, MA, USA) was advanced retrogradely into the popliteal artery but failed to meet the antegrade wire. Another retrograde access from popliteal artery followed a consistent tract. Further attempt from the ATA successfully approached the proximal cap. A 4.0 ×80 mm balloon was advanced retrogradely and inflated at 10 atm. From the antegrade route, the BeBack Crossing Catheter (Bentley InnoMed, Hechingen, Germany) was aimed toward the inflated balloon and successfully punctured the proximal cap, entering the balloon and confirming re-entry. Lesion preparation was completed antegradely, followed by drug-eluting stent deployment in the SFA, drug-coated balloon angioplasty of the popliteal–proximal ATA segment, and plain old balloon angioplasty of the distal ATA to DPA. Final angiography demonstrated excellent in-line flow to the plantar arch.

Retrograde Wiring.mp4
Retrograde Wiring Reaching The Proximal Cap.mp4
BeBack Puncturing Retrograde Balloon.mp4
Case Summary
This case demonstrates successful recanalization of a long femoropopliteal CTO with an ambiguous proximal cap and unclear vessel course. The combined antegrade and retrograde strategy, supported by distal ATA access and BeBack-assisted cap penetration, enabled successful revascularization. Restoration of in-line flow to the foot underscores the value of dual-access techniques and targeted device-assisted re-entry in complex chronic limb-threatening ischemia.