Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_008
Unusual Cause of Cardiac Tamponade During CHIP PCI
By Ganesan Nambirajan, Thomas Xavier Paul
Presenter
Ganesan Nambirajan
Authors
Ganesan Nambirajan1, Thomas Xavier Paul1
Affiliation
Meenakshi Mission Hospital and Research Centre, India1
View Study Report
CASE20251114_008
Coronary - Complication Management
Unusual Cause of Cardiac Tamponade During CHIP PCI
Ganesan Nambirajan1, Thomas Xavier Paul1
Meenakshi Mission Hospital and Research Centre, India1
Clinical Information
Relevant Clinical History and Physical Exam
This case is about an unusual case of cardiac tamponade occurring during a complex Chronic Total Occlusion (CTO) Percutaneous Coronary Intervention (PCI) requiring an innovative bailout strategy.Our patient was a 79-year-old male presenting with Acute Coronary Syndrome, Unstable Angina (ACS UA), and a moderately impaired Left Ventricular Ejection Fraction (LVEF) of 40%.
 se000.avi
se000.avi
Relevant Test Results Prior to Catheterization
His EF was 45 %Syntax score 36
Relevant Catheterization Findings
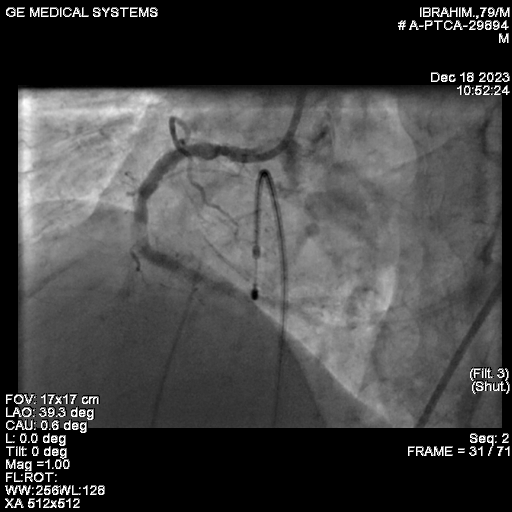
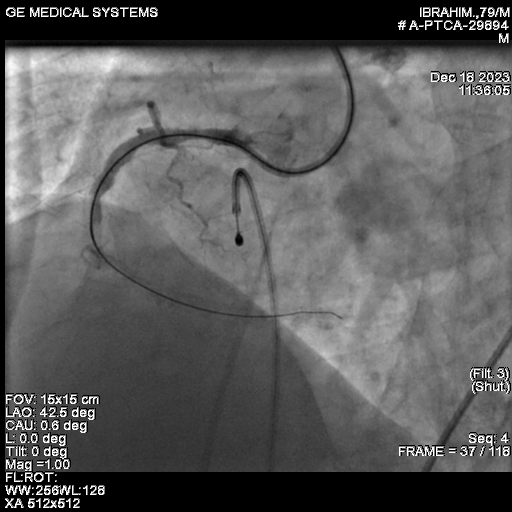
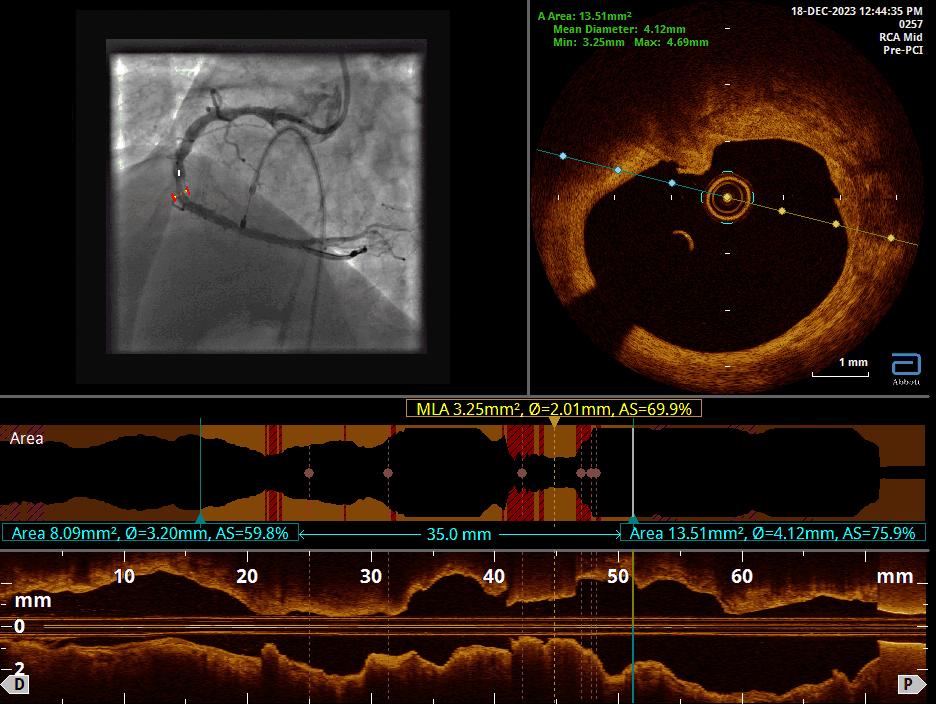
We proceeded with Percutaneous Transluminal Coronary Angioplasty (PTCA) of the Right Coronary Artery (RCA), utilizing ROTAPRO SUPPORT due to the calcified nature of the lesion. The CTO was successfully crossed using a Conquest Pro wire. Intravascular imaging, specifically Optical Coherence Tomography (OCT), confirmed the presence of multiple calcified nodules, highlighting the difficulty of the case.A 1.5 Rotapro was used for preparation.
Interventional Management
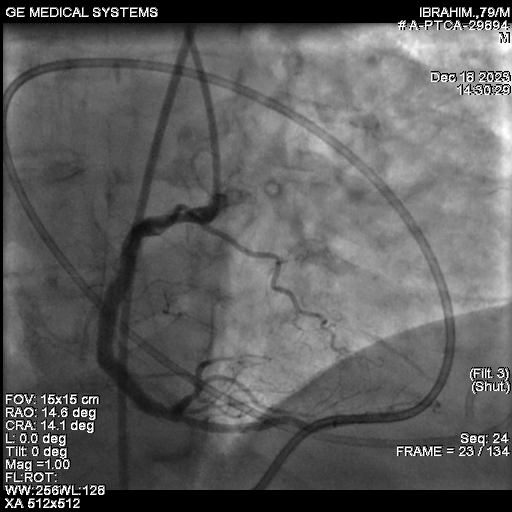
Procedural Step
After adequate lesion preparation, we deployed a 4x 38 mm DES. The post-PCI angiogram confirmed a successful final result in the RCA.Following the successful procedure, the patient was shifted to the CCU. Unfortunately, he rapidly developed hypotension and sweating. An urgent ECHO was performed, which revealed a massive pericardial effusion (PE).We maintained continuous pericardial aspiration. The patient's ACT was 280, and Protamine was administered to reverse the heparin effect. A check angiogram ruled out any wire-induced perforation, suggesting the perforation was likely iatrogenic from the temporary pacing wire that had been placed for Rotapro support. Pericardial aspiration continued, and CTS opinion was sought, with the high risk of surgical intervention being explained to the family.At this critical juncture, given the refractory nature of the bleeding, we looked to a new strategy. Literature supports the use of intra-pericardial thrombin injection as a bailout strategy for iatrogenic pericardial tamponade. The response to the intra-pericardial thrombin injection was prompt. The patient's hemodynamics gradually improved. He had an uncomplicated recovery and was discharged five days later.
se011.avi
Case Summary
Cardiac tamponade remains a rare but life-threatening complication of cardiac interventions.
* Despite prompt pericardiocentesis, managing the patient and achieving hemodynamic stabilization can be difficult.
* Intra-pericardial thrombin injection, performed after pericardiocentesis, is effective because it promotes hemostasis and acts as a sealing agent.
* Based on our experience, intra-pericardial thrombin injection appears to be a viable, new bailout strategy for patients presenting with iatrogenic pericardial tamponade following percutaneous intracardiac procedures, especially when surgery is high-risk or delayed.