Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_005
A Case of OCT-Identified Coronary Perforation in a Calcified Coronary Lesion: Imaging Warning Signs
By Masahiro Shimoda, Hirohiko Ando, Atomu Tajima, Hirohumi Ohashi, Akihiro Suzuki, Tetsuya Amano
Presenter
Masahiro Shimoda
Authors
Masahiro Shimoda1, Hirohiko Ando1, Atomu Tajima1, Hirohumi Ohashi1, Akihiro Suzuki1, Tetsuya Amano1
Affiliation
Aichi Medical University, Japan1
View Study Report
CASE20251114_005
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
A Case of OCT-Identified Coronary Perforation in a Calcified Coronary Lesion: Imaging Warning Signs
Masahiro Shimoda1, Hirohiko Ando1, Atomu Tajima1, Hirohumi Ohashi1, Akihiro Suzuki1, Tetsuya Amano1
Aichi Medical University, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
A 80-year-old male with a history of smoking and a family history of myocardial infarction presented with chest pain during exercise.
Relevant Test Results Prior to Catheterization
The electrocardiogram revealed no abnormalities, and echocardiography showed an ejection fraction (EF) of 64% with normal wall motion.Blood tests, including lipid levels, revealed no significant abnormalities.However, coronary CT angiography revealed diffuse, severe stenotic lesions with extensive calcification in all three main coronary arteries.

Relevant Catheterization Findings
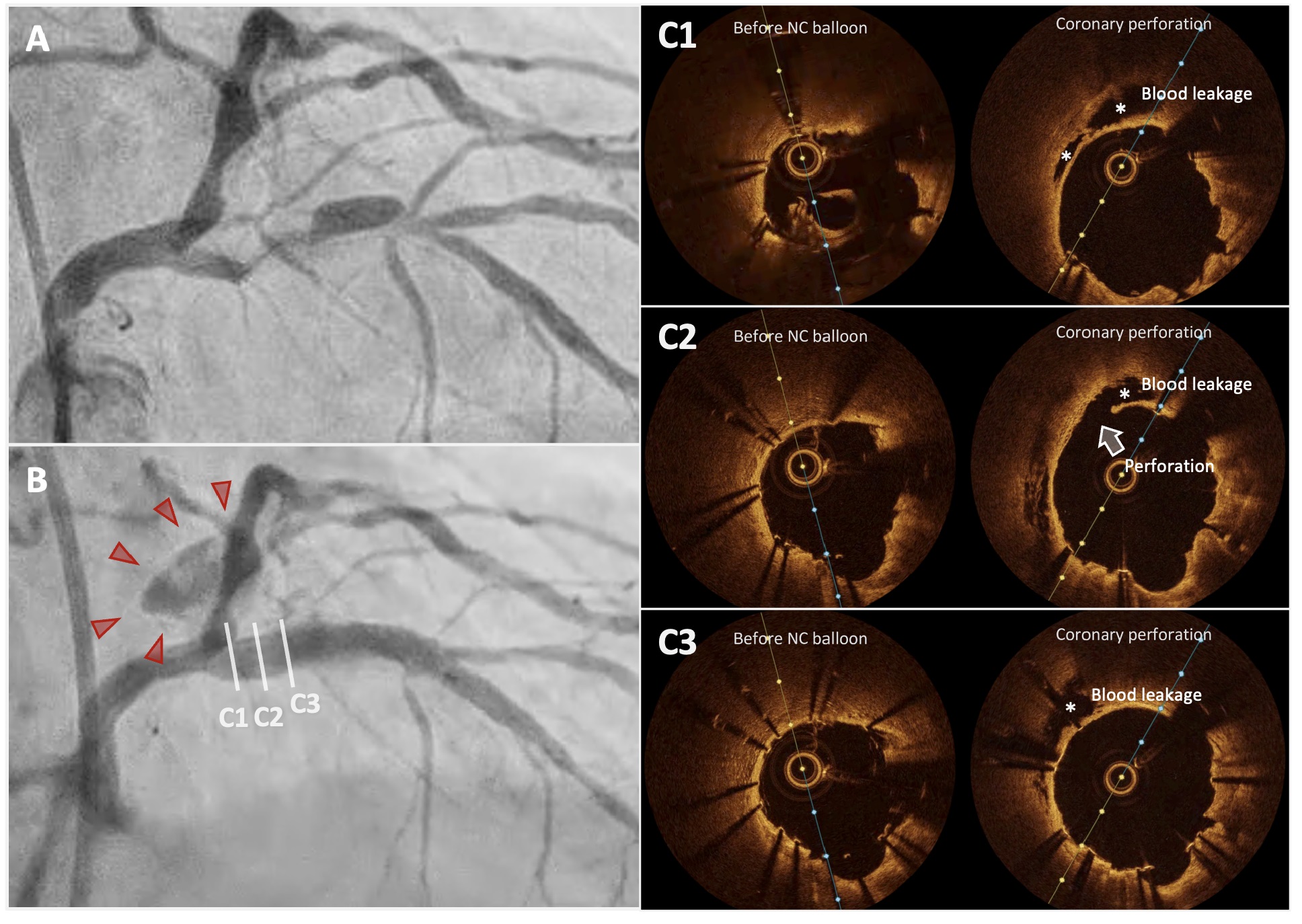
Coronary angiography revealed severe, heavily calcified stenosis in the proximal LAD. After stent implantation, OCT showed marked incomplete stent apposition at the proximal segment. During the OCT run, contrast extravasation emerged at the stent’s proximal edge, indicating perforation.
Interventional Management
Procedural Step
Lesion preparation was performed with rotational atherectomy (1.5mm burr) and 3.0mm balloon predilation were performed, followed by implantation of a 3.0×32mm Synergy drug-eluting stent (DES) in the proximal LAD. Post-stent OCT demonstrated notable incomplete stent apposition, so post-dilation with a 4.0-mm non-compliant balloon was undertaken, focusing on the proximal portion. During the subsequent OCT angiography run, new contrast extravasation was seen at the proximal stent edge consistent with coronary perforation. Immediate inflation of a 3.5-mm perfusion balloon across the injured segment secured hemostasis while maintaining distal flow. Extravascular hemorrhage gradually subsided, and the patient remained hemodynamically stable. Comparative OCT frames before and after the event revealed epicardial-side wall detachment and signal-free zones within perivascular adipose tissue. Notably, pre-dilation OCT at the same site showed loss of the normal three-layer architecture, suggesting local fragility that, combined with aggressive post-dilation in a calcified segment, predisposed the vessel to perforation.
Case Summary
OCT revealed the mechanism of perforation and its warning signs. These include wall detachment and extravascular signal loss at the perforation site, as well as pre-existing weakening of the arterial tri-laminar structure at the injury site. Recognizing these patterns may allow for more cautious post-dilatation management during the use of debulking devices for calcified coronary lesions.