Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251114_001
The Heart in a Cage: Angiographic Evidence of Constrictive Pericarditis
By Masayoshi Iwamoto
Presenter
Masayoshi Iwamoto
Authors
Masayoshi Iwamoto1
Affiliation
Sumitomo Hospital, Japan1
View Study Report
CASE20251114_001
Heart Failure - Vascular Heart Disease and Cardiomyopathies
The Heart in a Cage: Angiographic Evidence of Constrictive Pericarditis
Masayoshi Iwamoto1
Sumitomo Hospital, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
A 59-year-old man presented with bilateral lower leg edema. His past medical history was no history of open-heart surgery, chest radiation, or preceding febrile illness. His height was 176cm, body weight was 82.1kg. His vital signs were as follows: blood pressure 98/68 mmHg, heart rate 82 bpm, and oxygen saturation 97% on room air. Chest X ray showed bilateral pleural effusion. (Fig 1)

Relevant Test Results Prior to Catheterization
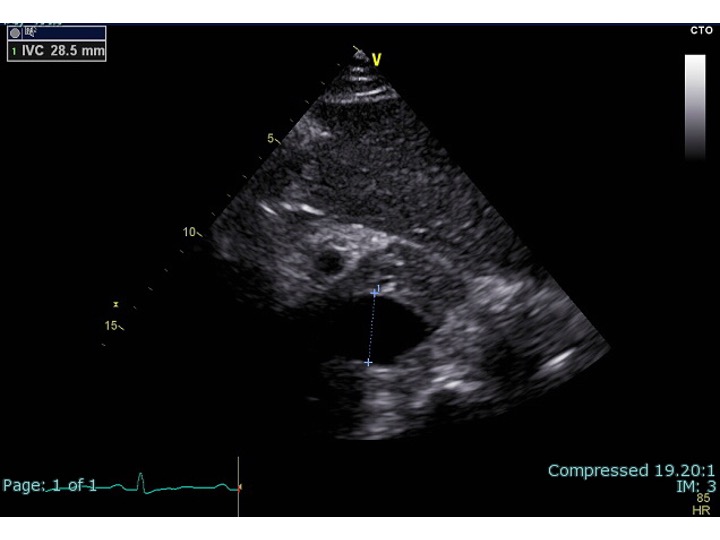
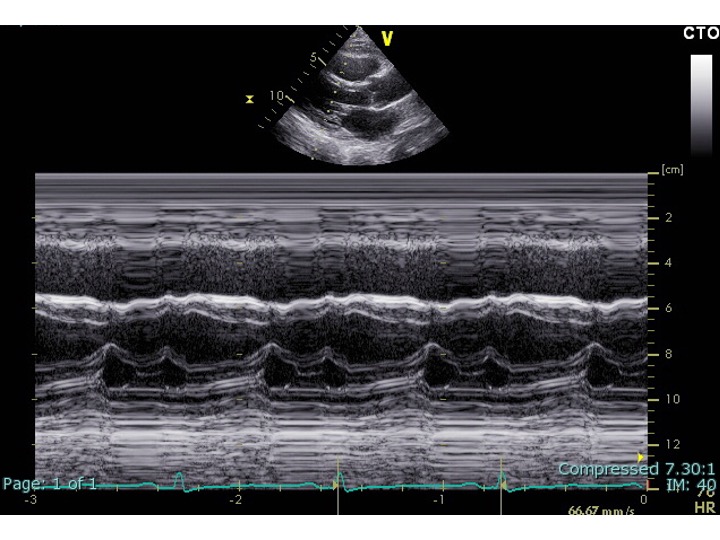
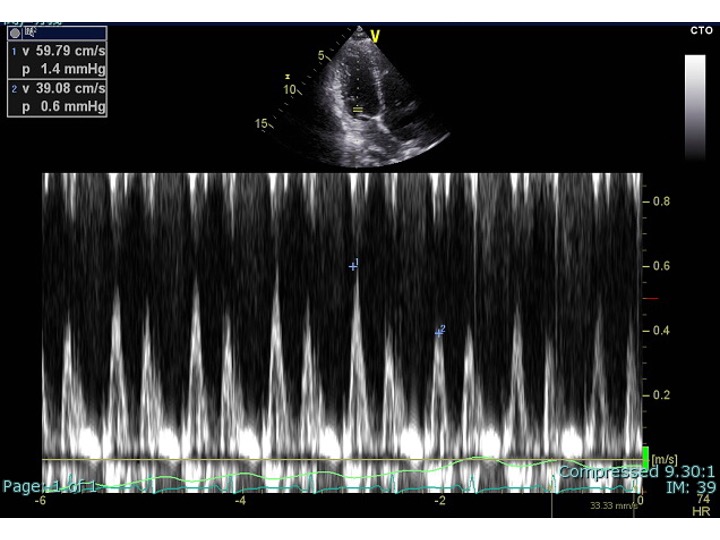
ransthoracic echocardiography was performed: Although the left ventricular ejection fraction was preserved, the inferior vena cava was dilated and showed no respiratory variation. There were pericardial adhesion and a septal bounce (Fig2-4). He was suspected of having constrictive pericarditis and was admitted for further evaluation.
Relevant Catheterization Findings
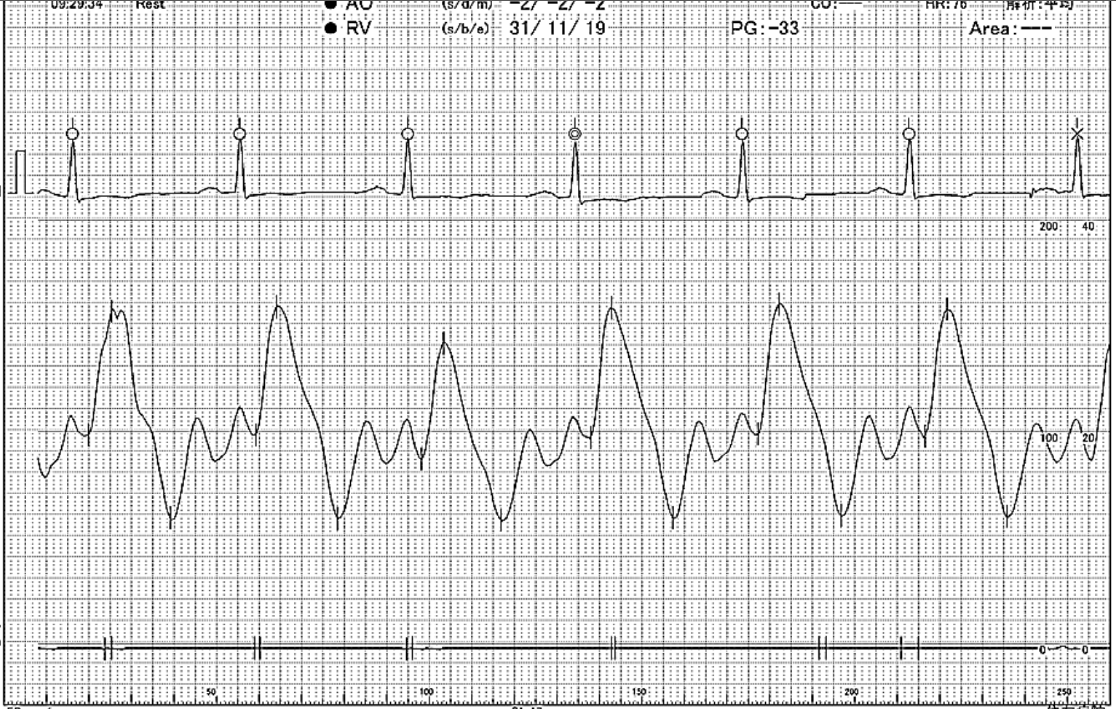
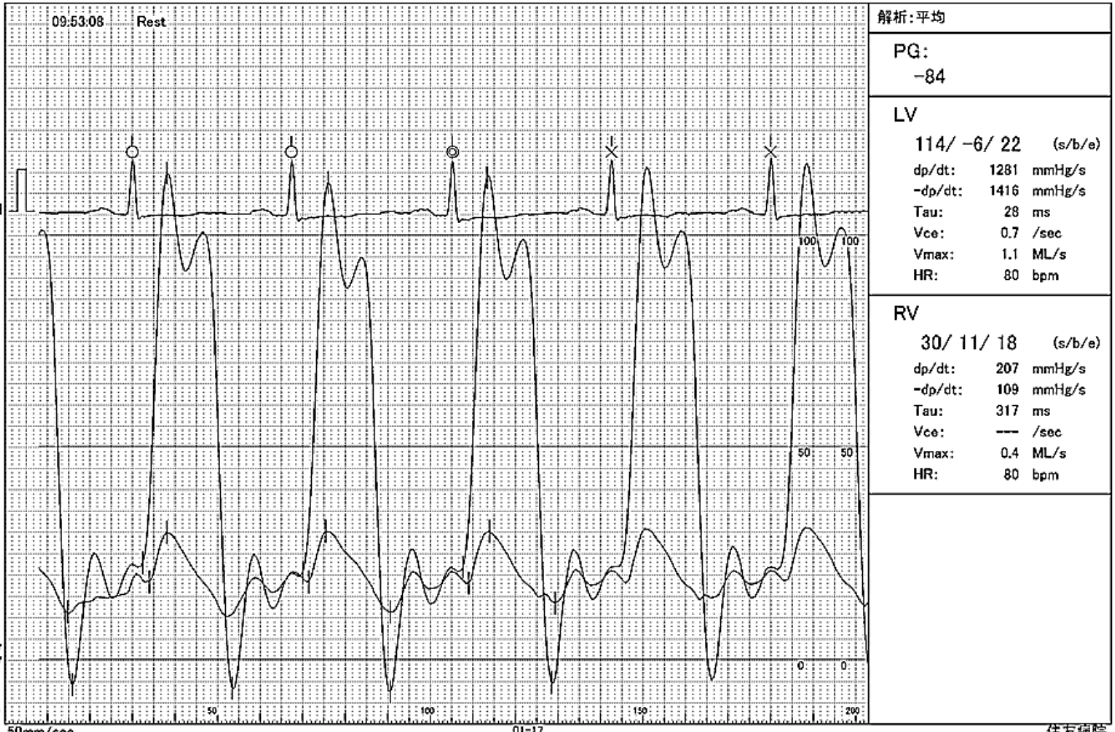
Right heart catheterization demonstrated hemodynamic findings: The LVEDP–RVEDP gradient was 4 mmHg (< 5 mmHg), and the RA pressure waveform demonstrated a deep y descent (Fig 5). Both right and left ventricular pressure tracings showed a characteristic dip-and-plateau pattern. No significant respiratory discordance was observed between LVSP and RVSP (Fig 6).
Interventional Management
Procedural Step
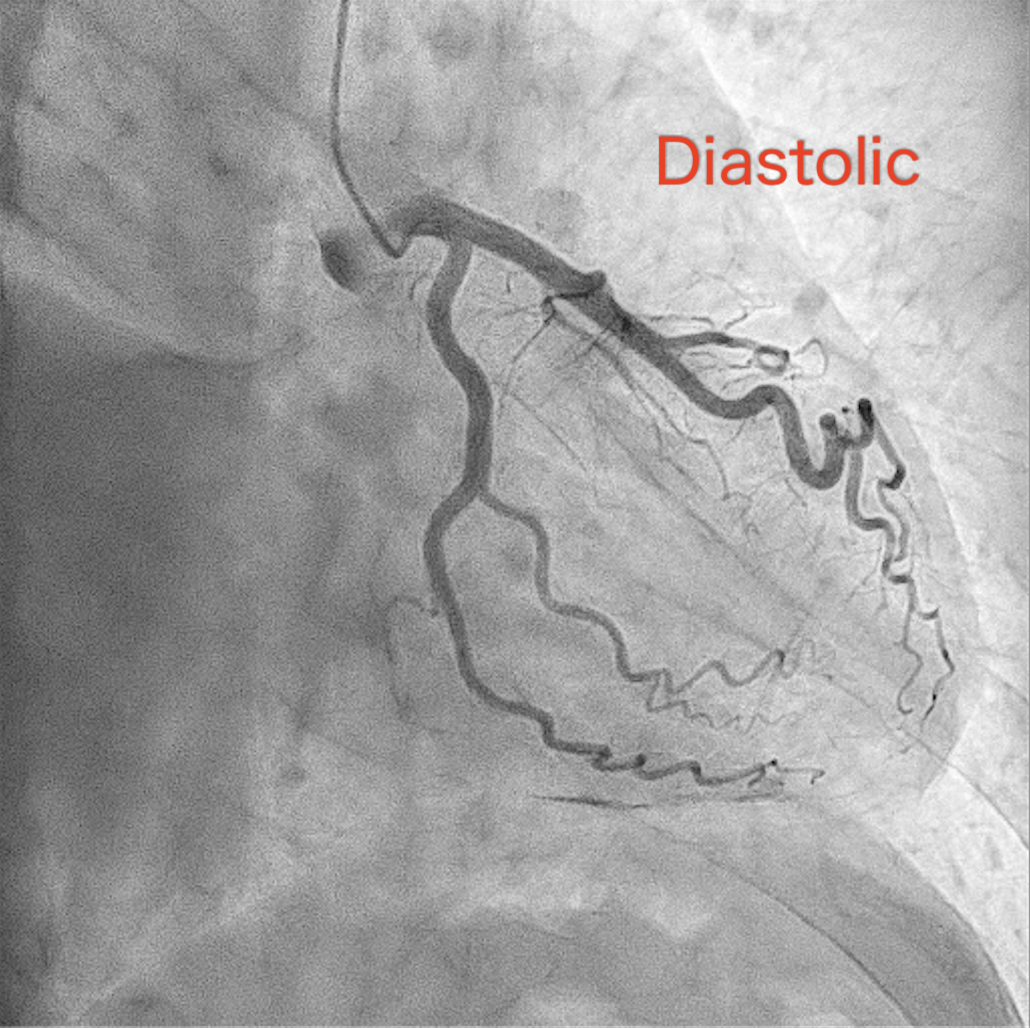
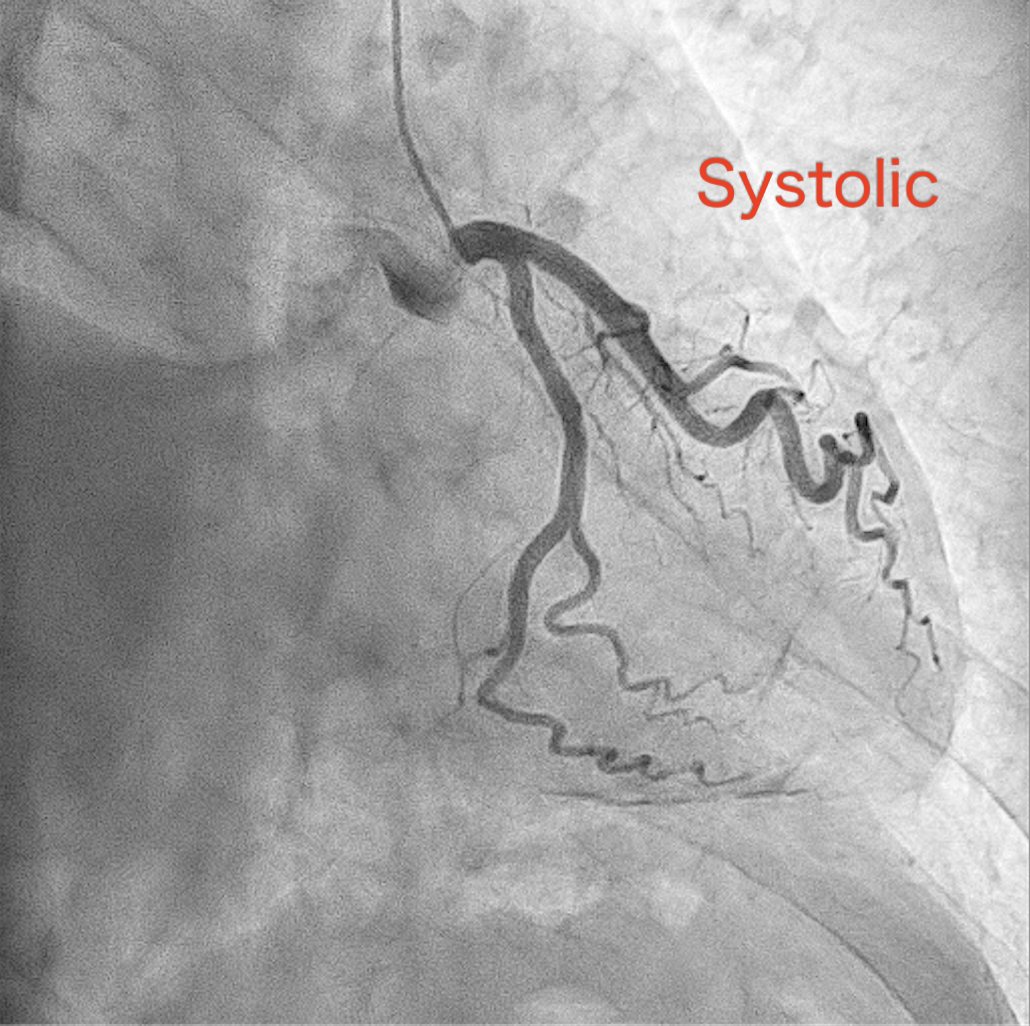
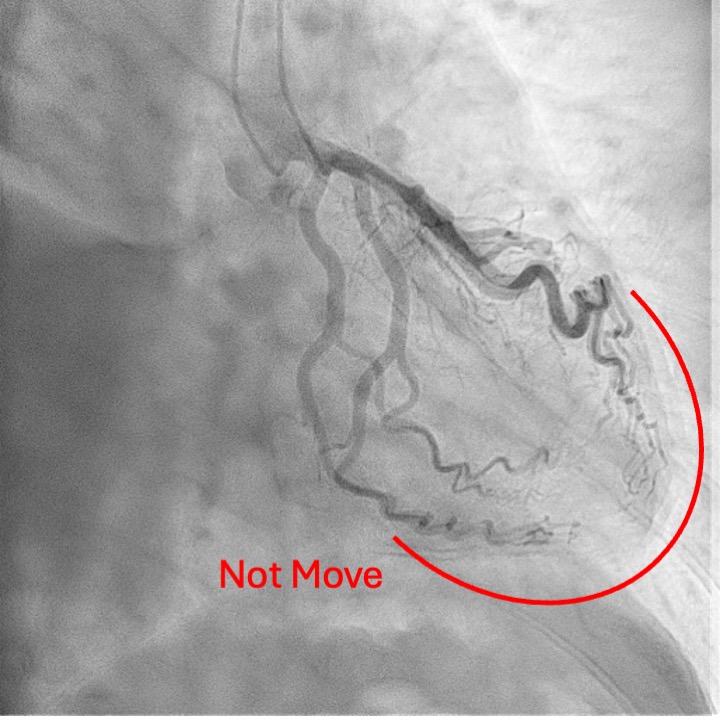
Coronary angiography revealed a distinctive finding in which the vessels and branches covering mid- to apical region of the left ventricle did not completely move in conjunction with the cardiac cycle, while those covering basal-part myocardium and running along left atrioventricular groove remain synchronized with the heart motion. This unusual finding was explained by the hard-and-fixed pericardium firmly adhered to the myocardium constraining the pulsation of the relevant part of the coronary tree. (Fig7-8)
 RAO35 CAU30.mp4
RAO35 CAU30.mp4
CardiacCT.mp4
Case Summary
Constrictive pericarditis is typically diagnosed by a combination of echocardiography, hemodynamic assessment. However, cases in which coronary angiography clearly demonstrates pericardial adhesion are extremely rare. Recognition of such findings may be clinically valuable, as preoperative identification of adhesion sites could allow for more accurate surgical planning when considering pericardiectomy. Moreover, the combination of coronary angiography and cardiac CT may provide complementary information that enhances diagnostic confidence.We present this case with a literature review to highlight the potential diagnostic utility of coronary angiography in constrictive pericarditis.