Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251113_017
Rescue PCI With Rotational Atherectomy for Severely Calcified LM Bifurcation in a High-Risk Octogenarian
By Chuan-Tsai Tsai, Pei Hsi Wu
Presenter
Pei Hsi Wu
Authors
Chuan-Tsai Tsai1, Pei Hsi Wu1
Affiliation
Taipei Veteran General Hospital, Taiwan1
View Study Report
CASE20251113_017
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Rescue PCI With Rotational Atherectomy for Severely Calcified LM Bifurcation in a High-Risk Octogenarian
Chuan-Tsai Tsai1, Pei Hsi Wu1
Taipei Veteran General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
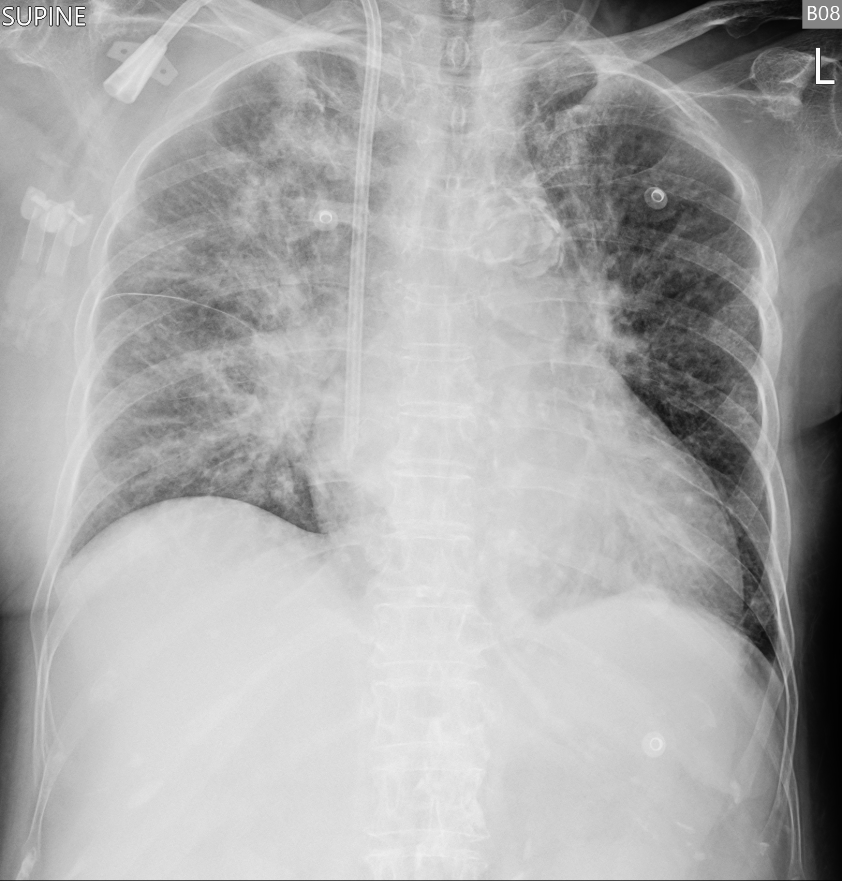
An 86-year-old woman with ESRD on HD, recurrent heart failure, prior PEA arrest, AF (CHA₂DS₂-VASc 7), DM, HTN, dyslipidemia, and prior NSTEMI presented with sudden dyspnea, orthopnea, diarrhea, and desaturation at home. She appeared acutely ill on arrival, tachypneic with RR 30/min, BP 156/67 mmHg, pulse 78/min, GCS 15, and without peripheral edema. CXR showed increased opacities over both lung fields.
Relevant Test Results Prior to Catheterization
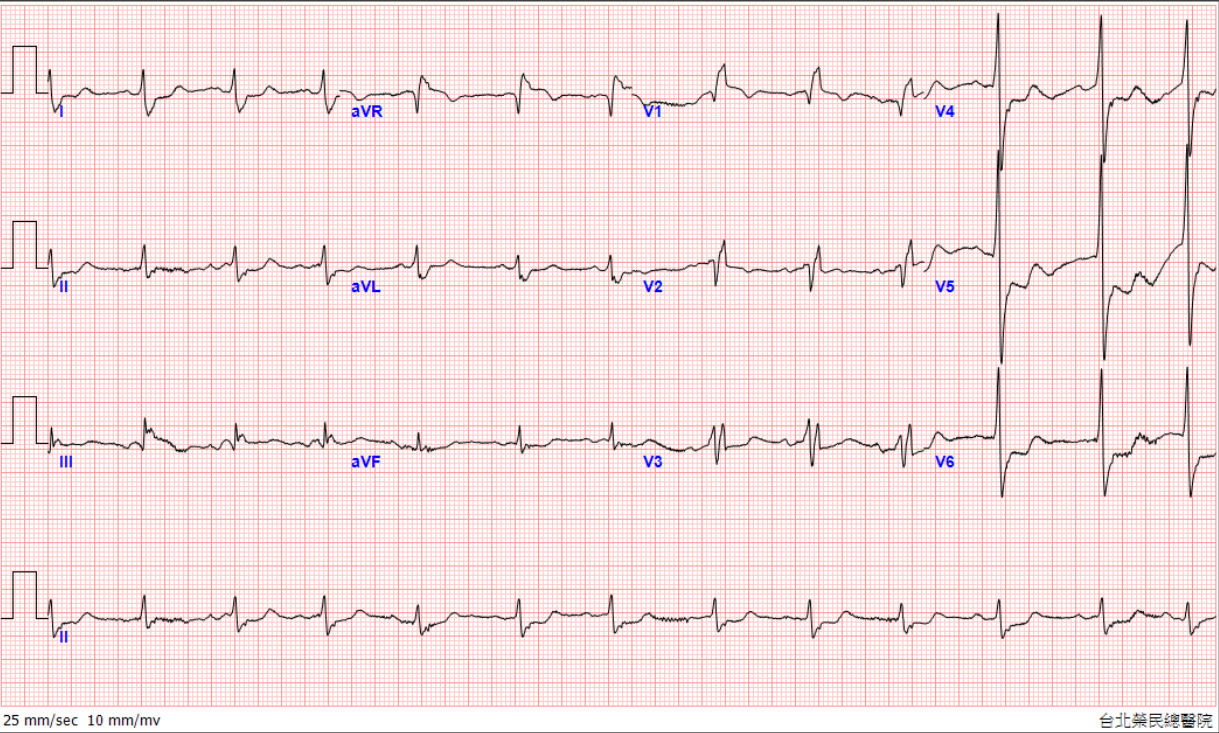
Before catheterization, labs showed WBC 24,090/µL, Hb 9.8 g/dL, glucose 909 mg/dL, Na 129 mmol/L, CRP 21.66 mg/dL, NT-proBNP 42,140 pg/mL, CK 384 U/L, and troponin rapidly rising from 1.00 to 63 ng/mL. ECG revealed ST elevation in aVR with diffuse ST depression. Bedside echocardiogram showed decreased LVEF with hypokinesia over apical area. BP later dropped to 85/28 mmHg, prompting urgent PCI.
 1_A4C TTE.mp4
1_A4C TTE.mp4
Relevant Catheterization Findings
CAG was performed through RRA access with a 6/7 Fr APT sheath, which revealed AMI with CAD and LM+TVD.
Left Main :
- D: Calcified lesion with 99% stenosis(Medina 1,1,1)
Left Anterior Descending :
- P: 99% stenosis
- D: 90% stenosis
Left Circumflex :
- P: 99% stenosis
- D: 70% stenosis
- OM: 70% stenosis
Right Coronary :
-P: 90% stenosis over proximal instent
2_LCA AP caudal.mp4
3_LCA AP cranial.mp4
1_IVUS.mp4
Interventional Management
Procedural Step
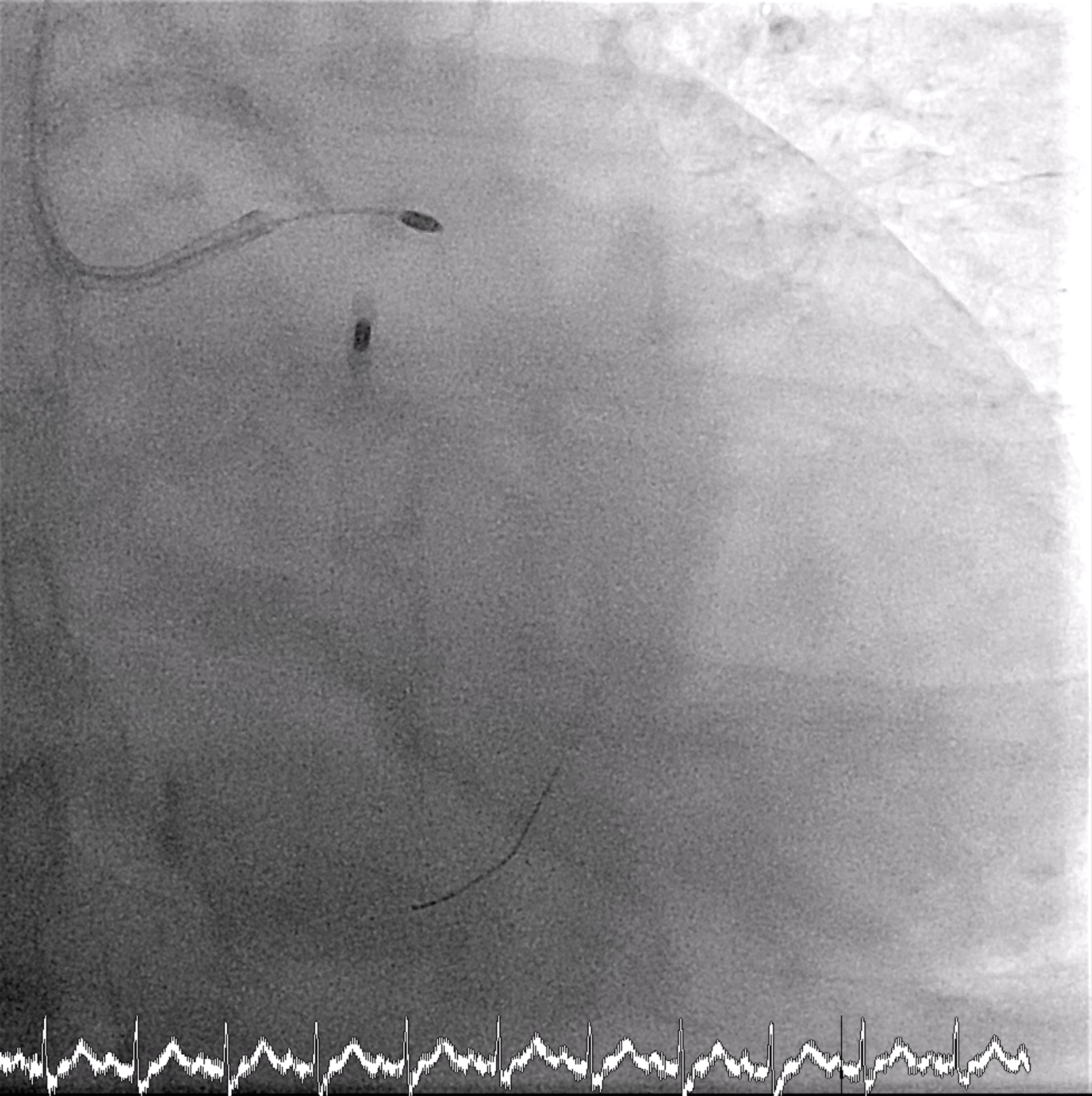
An 8 Fr IABP sheath was inserted via the right femoral artery under fluoroscopic guidance. The guidewire was advanced to the aortic root, and an ARROW IABP catheter was positioned in the descending aorta at the level of the aortic knob with good augmentation. Left femoral access was left for possible mechanical circulatory support. PCI was then initiated via right radial access using a 6/7 Fr APT sheath. The LMCA was engaged with an XB 3.5/7 GC, and an Anyreach wire was advanced to the LAD. IVUS could not cross the heavily calcified LM bifurcation, so rotational atherectomy was performed. After exchanging to a Rotadrive floppy wire, rotablation with a 1.75 mm burr was performed from LM to LAD for three runs at 147,000–166,000 rpm. POBA was carried out along LAD-D and LAD-P, followed by IVUS confirming circumferential calcification.Attention was then turned to the LCx. Due to uncrossable IVUS, the wire was exchanged for a Rotadrive floppy wire and rotablation was repeated from LM to LCx for seven runs at 136,000–166,000 rpm. Balloon dilation was performed, and IVUS again showed heavy LM–LCx calcification. A 3.0×26 mm Frontier DES was placed from LM to LCx, followed by post-dilatation. Then a 3.0×34 mm Frontier DES was deployed from LM to LAD-P, with sequential post-dilatation using NC balloons up to 18 atm. The bifurcation was optimized with rewiring and final kissing balloon inflation using 3.5 mm and 3.0 mm NC balloons, and proximal optimization with a 4.0 mm NC balloon.


5_rota LAD.mp4
5_IVUS.mp4
17_LAD stent.mp4
Case Summary
This case highlights the successful use of IABP-supported high-risk PCI to treat a critically ill 86-year-old woman with NSTEMI and heavily calcified Medina 1,1,1 LM bifurcation disease. Dual-vessel rotablation, IVUS guidance, and culotte technique for LM bifurcation reconstruction achieved full revascularization with TIMI 3 flow. Despite multiple comorbidities and hemodynamic instability, prompt intervention restored coronary perfusion and stabilized the patient, demonstrating the feasibility of complex LM PCI in extreme-risk settings.