Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251113_013
LAMPOON-Assisted Transcatheter Mitral Valve-in-Valve Replacement
By Ravinder Singh Rao, Ganesan Nambirajan
Presenter
Ganesan Nambirajan
Authors
Ravinder Singh Rao1, Ganesan Nambirajan1
Affiliation
Meenakshi Mission Hospital and Research Centre, India1
View Study Report
CASE20251113_013
Structural - Mitral Valve Intervention - Transcatheter MV Replacement
LAMPOON-Assisted Transcatheter Mitral Valve-in-Valve Replacement
Ravinder Singh Rao1, Ganesan Nambirajan1
Meenakshi Mission Hospital and Research Centre, India1
Clinical Information
Relevant Clinical History and Physical Exam
"Our patient was a 76-year-old male with a history of Mitral Valve Replacement (MVR) and Coronary Artery Bypass Grafting (CABG) in 2009. He presented with bioprosthetic valve dysfunction associated with severe mitral stenosis and regurgitation, alongside a critical finding: a narrow LVOT.
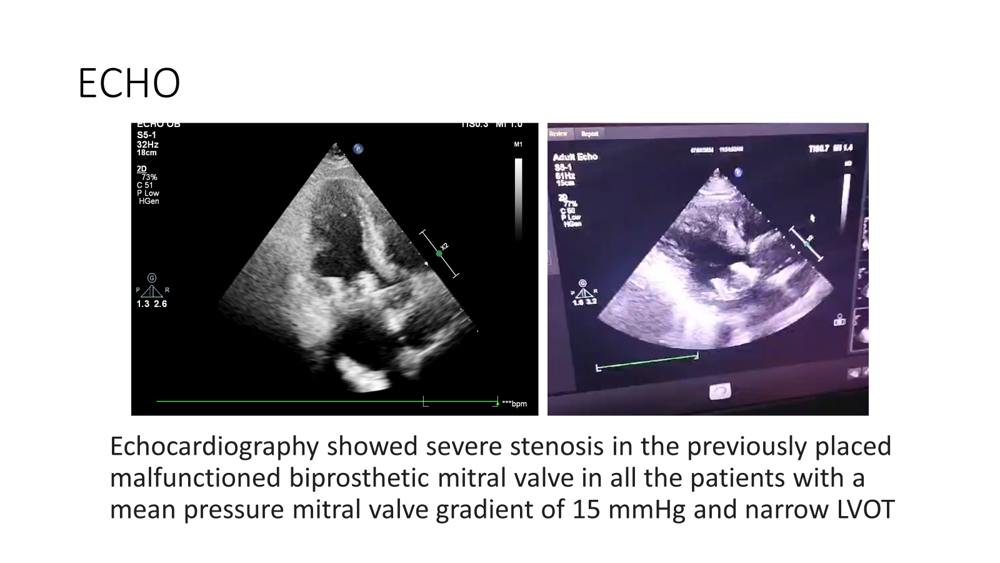
Relevant Test Results Prior to Catheterization
Considering his overall surgical risk—with a Society for Thoracic Surgery (STS) score ranging between 4.2 and 6.2, and a preoperative mean mitral valve pressure gradient of 12–18 mmHg—a redo MVR would have been a high-risk surgery. Therefore, a Lampoon-assisted TMVR was planned."
Relevant Catheterization Findings
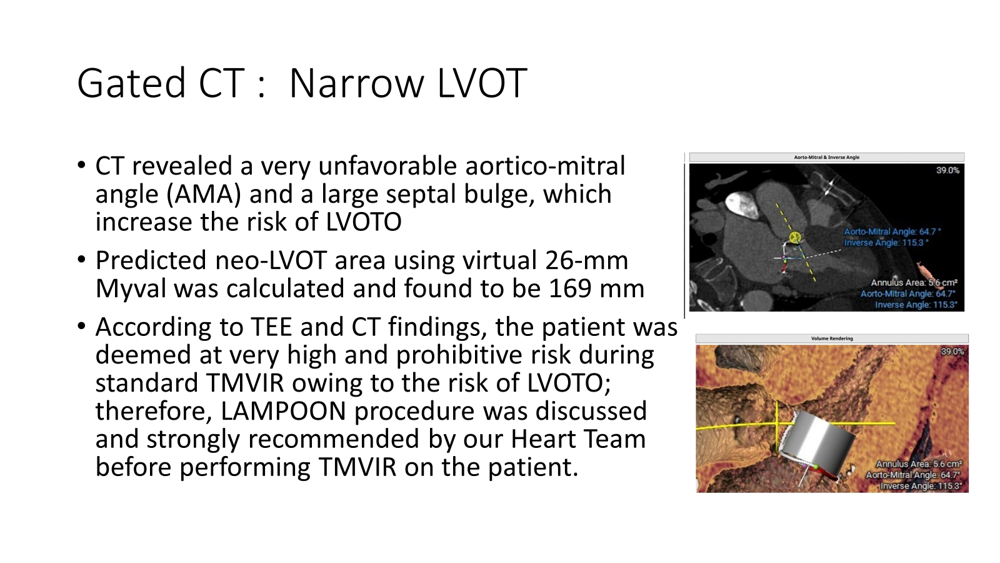
"The Gated CT was crucial in risk assessment. It confirmed the narrow LVOT and revealed a very unfavorable aortico-mitral angle (AMA) and a large septal bulge, factors which significantly increase the risk of LVOT Obstruction (LVOTO).
The predicted neo-LVOT area, calculated using a virtual 26-mm Myval valve, was found to be 169 mm2."
Interventional Management
Procedural Step
"The entire procedure was performed under GA, guided by fluoroscopy and TEE.
* Access: We used a transfemoral/transseptal approach.
Transseptal postero-inferior puncture was achieved through the right femoral vein under TEE guidance.
* The left femoral vein was maintained for temporary rapid pacing during valve implantation. Radial artery access was also established for pressor monitoring.
* A Left Atrial (LA) steerable sheath (Agilis NxT) was placed into the LA after a successful inferoposterior transseptal puncture. The intra-atrial septum was dilated with a 24 mm balloon.
* Venoarterial Loop: A balloon wedge end-hole catheter was floated through the mitral ring and into the LV. A 0.035 Terumo guidewire was advanced through this catheter, snared in the aorta, to create the first venoarterial loop."
A 6F guiding catheter was inserted through the femoral artery over the existing wire loop and advanced into the Agilis sheath.
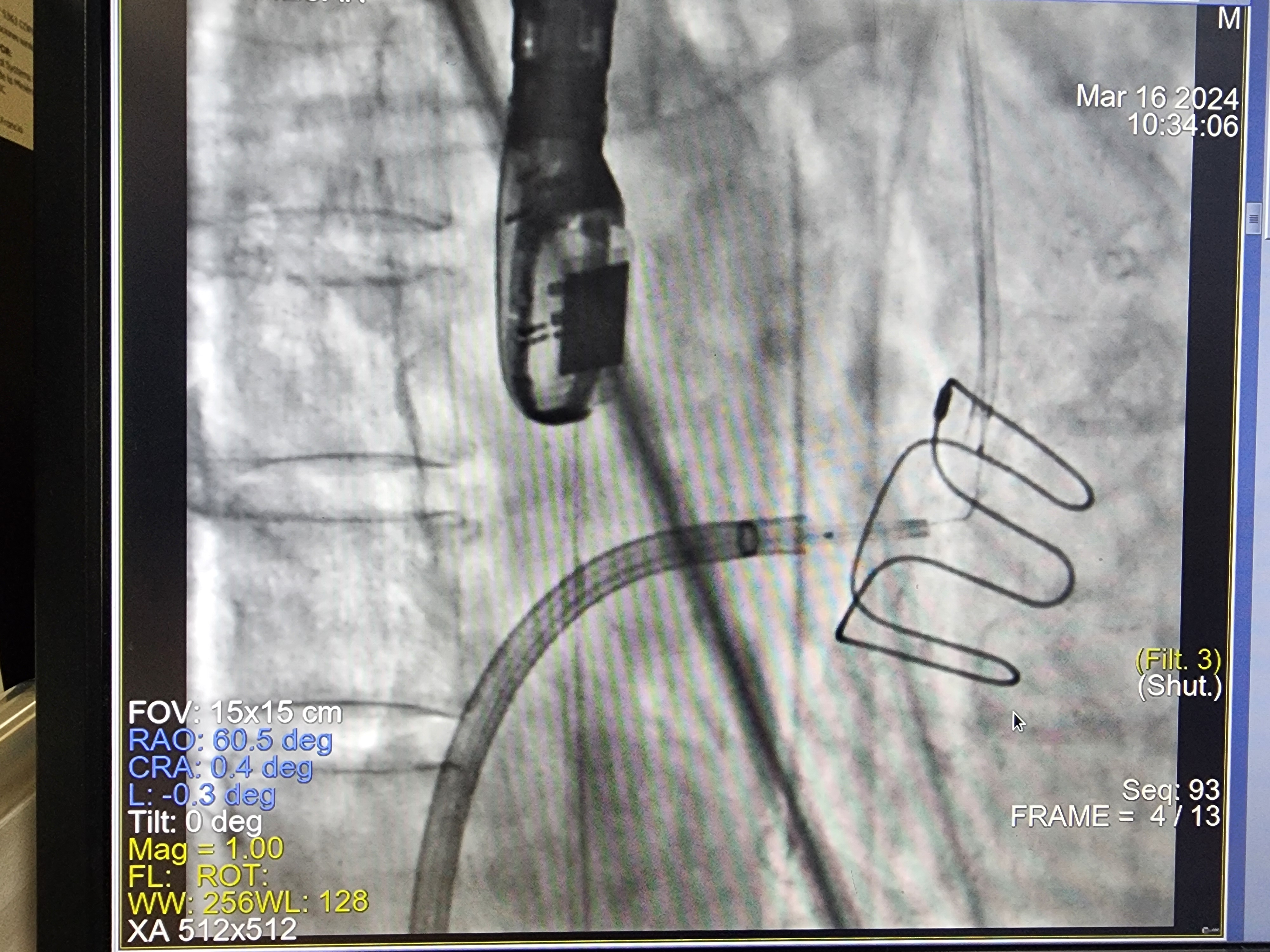
* A 0.014-inch Astato XS20 wire was prepared: its mid-segment was kinked and focally denuded outside to form a 'Flying V'.
Transcatheter Tip to base LAmpoon was completed as per standard technique. TEE confirmed the successful tip-to-base laceration of the mitral leaflet.
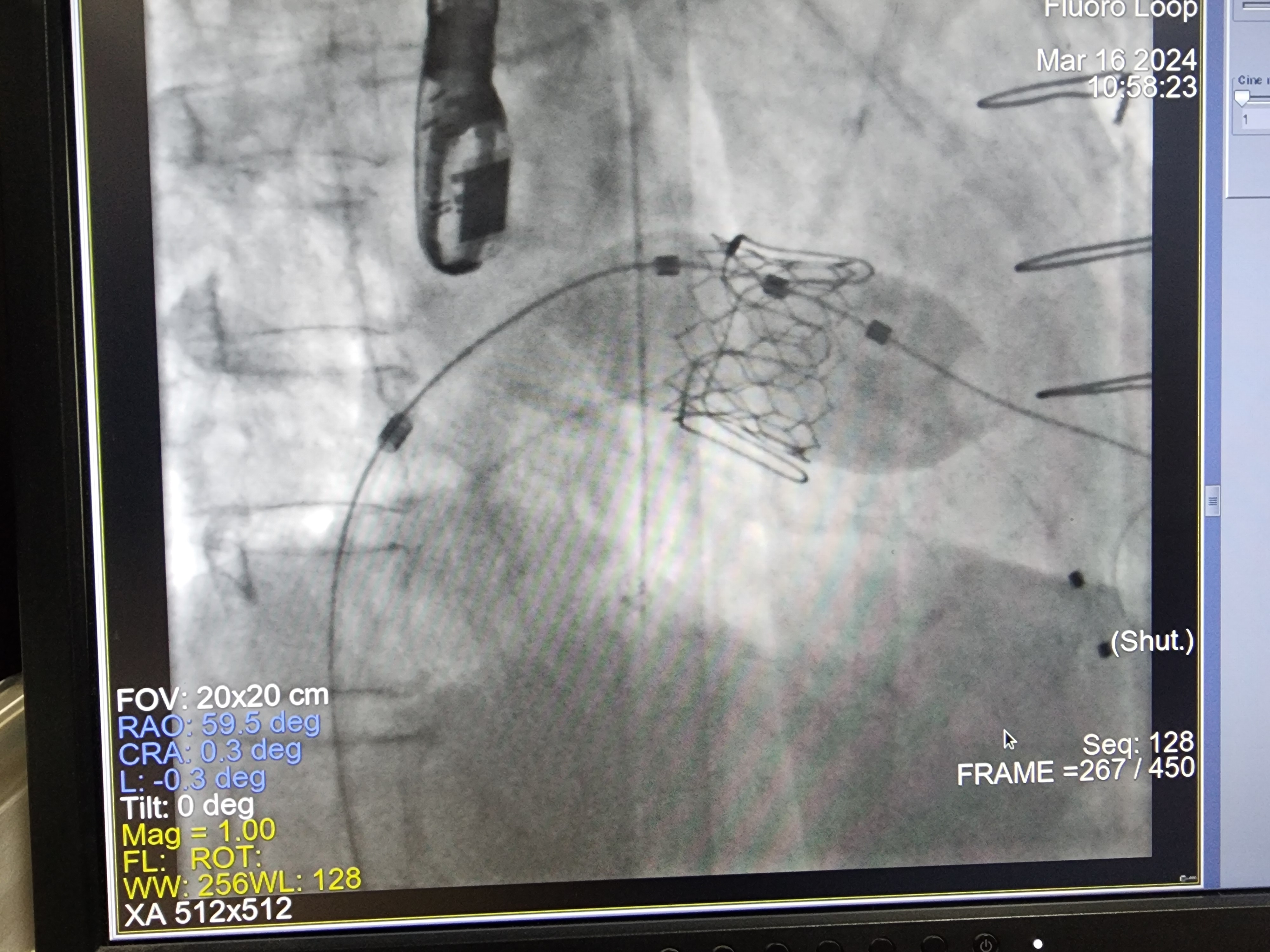
The Transcatheter Mitral Valve in Valve Replacement (TMVIR) was then successfully performed using a 26-mm Myval™ transcatheter heart valve. This was carried out under rapid pacing at 180 bpm.
Case Summary
"TMVR is a vital therapeutic option for high-risk, inoperable patients with severe mitral disease. However, displacement of the native anterior mitral leaflet toward the interventricular septum can cause acute LVOT obstruction, a common complication with high mortality. Predicting and preventing this is essential.
LAMPOON is a transcatheter electrosurgical technique designed to split the anterior mitral valve leaflet immediately prior to TMVR, preventing this obstruction. It is a novel, life-saving therapy."