Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251113_012
The Hemodynamic Cost of a Hidden Shunt: A Challenging Case of Chronic Heart Failure as a Consequence of an Unrecognized Renal Arteriovenous Fistula (rAVF) Successfully Managed With Renal Artery Covered Stenting
By Kevin Paul Enriquez, Ramon Abiera, Jeffrey Mendoza, Ricardo Jose Quintos
Presenter
Kevin Paul Enriquez
Authors
Kevin Paul Enriquez1, Ramon Abiera1, Jeffrey Mendoza1, Ricardo Jose Quintos1
Affiliation
Cardinal Santos Medical Center, Philippines1
View Study Report
CASE20251113_012
Endovascular - Other Endovascular Interventions
The Hemodynamic Cost of a Hidden Shunt: A Challenging Case of Chronic Heart Failure as a Consequence of an Unrecognized Renal Arteriovenous Fistula (rAVF) Successfully Managed With Renal Artery Covered Stenting
Kevin Paul Enriquez1, Ramon Abiera1, Jeffrey Mendoza1, Ricardo Jose Quintos1
Cardinal Santos Medical Center, Philippines1
Clinical Information
Relevant Clinical History and Physical Exam
A 59 y/o male had a remote history of exploratory laparotomy for a right upper abdominal stab wound. Years later, he developed heart failure with multiple hospitalizations for decompensation. With a normal coronary angiogram, he was managed as idiopathic cardiomyopathy. In the interim, he developed persistent bloating and abdominal discomfort hence further workup was done. Patient had signs of bi-ventricular failure (edema, distended neck veins, displaced apex beat). No abdominal bruit was noted

Relevant Test Results Prior to Catheterization
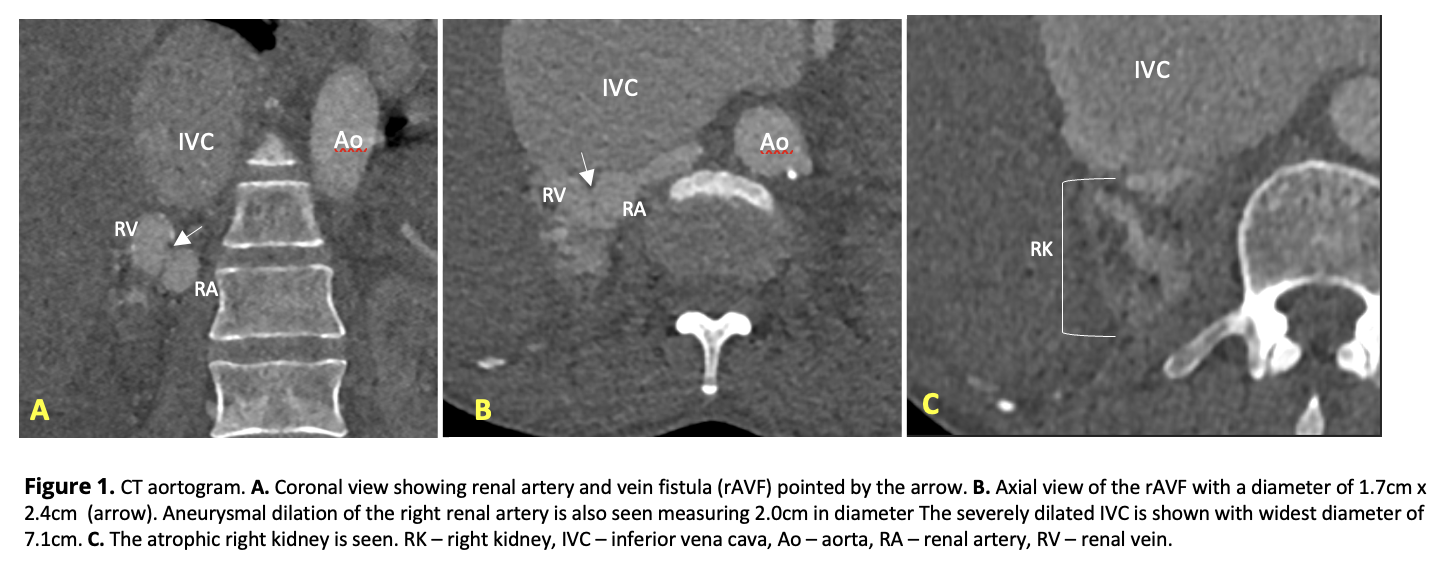
CT aortogram showed an atrophic right kidney with aneurysmal dilation of the distal right renal artery and vein with a fistulous communication in between (1.7x2.4cm, WxAP). The inferior vena cava was severely dilated at 7.1cm. Renal scintigram showed poor right kidney function (6%) and compensatory enlargement of the left (94% function). Echocardiogram showed global hypokinesia, ejection fraction (EF) of 21% with marked dilatation of all chambers and severe pulmonary hypertension (sPAP 48mmHg).
Relevant Catheterization Findings
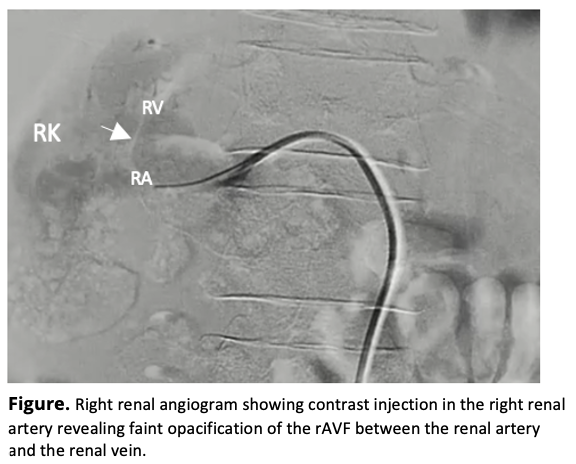
Right renal angiogram revealed a renal artery with an aneurysmal dilatation at its distal segment with a faint opacification of a single fistulous connection to the renal vein, confirming the rAVF seen in the CT aortogram. The fistula measures approximately 3cm in length and 1.7cm in diameter consistent with the CT findings. Based on epidemiology (more commonly acquired than congenital), morphology (single communication, aneurysmal), and chronology of events, the rAVF is considered acquired.
 rAVF video angio.mp4
rAVF video angio.mp4
Interventional Management
Procedural Step
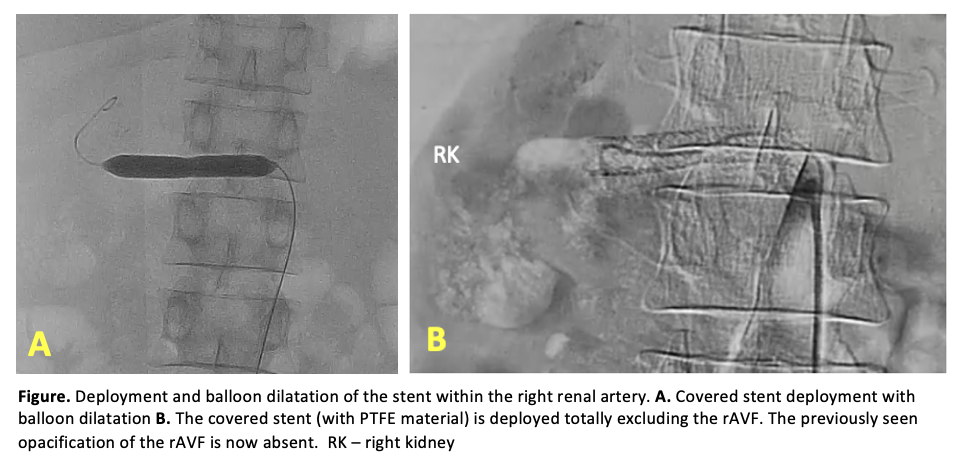
Intervention to interrupt the shunt that is diverting blood flow to the inferior vena cava and causing high output heart failure was necessary. Surgical treatment such as nephrectomy or renal artery ligation, known to be standard treatments, were deemed high risk procedures in our patient that has a prohibitive cardiac status. Transcatheter coil embolization, the most commonly used intervention, was also not an option in this case due to the presence of a large fistula which increases the risk of coil migration and embolic events. Hence, after shared decision making, percutaneous renal angioplasty was done using a 9mm Advanta PTFE balloon-expandable covered stent to exclude the fistula and interrupt the shunt. With the patient already on an anticoagulant (apixaban) for atrial fibrillation, a single antiplatelet (aspirin) was started. Heart failure medication regimen for the reduced EF was continued. 5 months after, there was significant clinical improvement with resolved edema and increased exercise tolerance. EF improved from 21% to 49%. Surveillance renal duplex scan revealed significantly elevated velocities within the stent suggestive of in-stent stenosis. This was an anticipated and accepted complication of the intervention, as the ultimate goal was alleviation of central volume overload and not restoration of renal perfusion. The patient remains well and euvolemic.

rAVF stenting done.mp4
Case Summary
This case highlights a rare but important hemodynamic cause of long-standing high-output heart failure that should be considered even in the absence of overt clinical findings that suggest a vascular etiology and more so in patients lacking conventional cardiovascular risk factors. Data on covered stent exclusion of a rAVF is limited with only two published cases existing to date. While surgery and embolization remain standard treatment, this case demonstrates endovascular exclusion of rAVF using a covered stent to be an effective alternative to surgery or embolization, particularly in cases where the kidney function on the side of the fistula is already negligible.