Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251113_009
Breaking Within Limits
By Felix Maverick Rubillar Uy Uy, Rahul Kurup
Presenter
Felix Maverick Rubillar Uy Uy
Authors
Felix Maverick Rubillar Uy Uy1, Rahul Kurup1
Affiliation
Liverpool Hospital, Australia1
View Study Report
CASE20251113_009
Coronary - Complication Management
Breaking Within Limits
Felix Maverick Rubillar Uy Uy1, Rahul Kurup1
Liverpool Hospital, Australia1
Clinical Information
Relevant Clinical History and Physical Exam
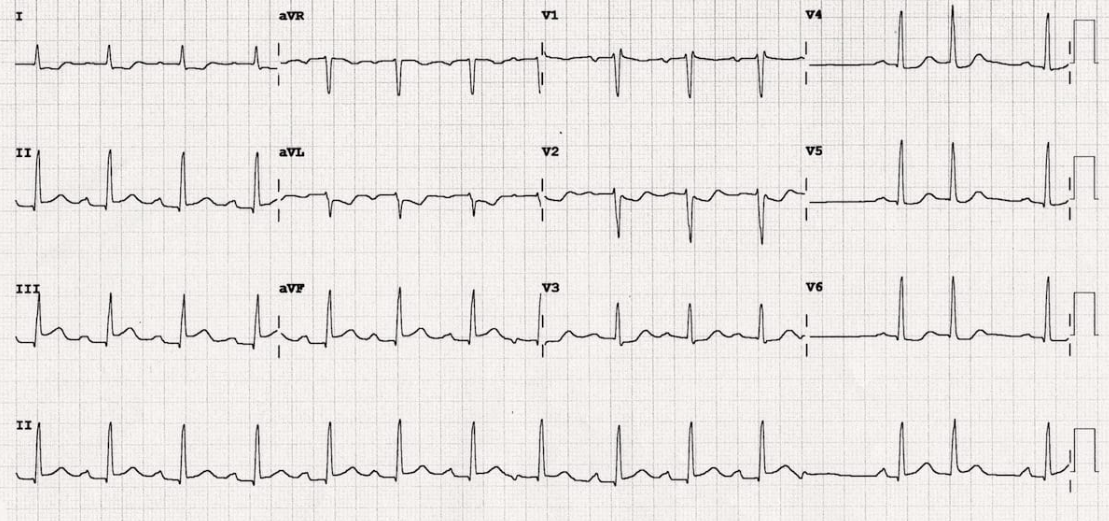
A 53yr old male with a past medical history of hypertension and no known cardiovascular history was brought in by ambulance with a 2-hour history of chest pain. His ECG on arrival was consistent with inferior ST elevation myocardial infarction. He was hemodynamically stable, cardiovascular examination revealed normal dual heart sounds and no adventitious lung sounds.
Relevant Test Results Prior to Catheterization
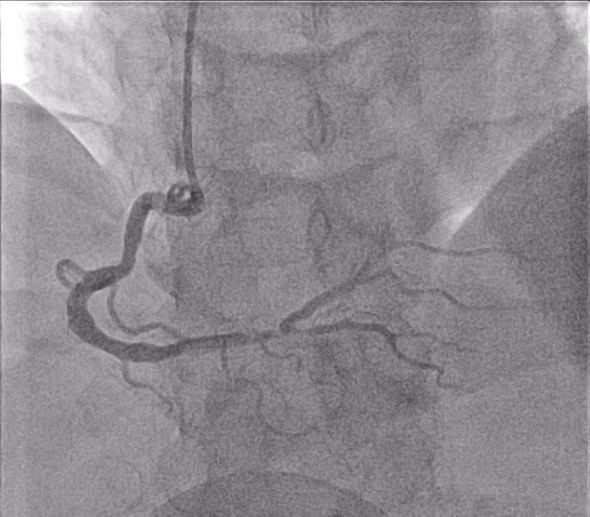
ECG showed normal sinus rhythm with ST elevation in II, III and AvF. Complete blood count, electrolytes and kidney function were within normal limits. Troponin-t was not available before catheterization. Coronary angiogram through a right radial approach showed single vessel disease with a diffuse critical stenosis at the distal RCA bifurcation (Medina 1,1,0) with a severe size mismatch between the distal RCA and RPDA.
Relevant Catheterization Findings
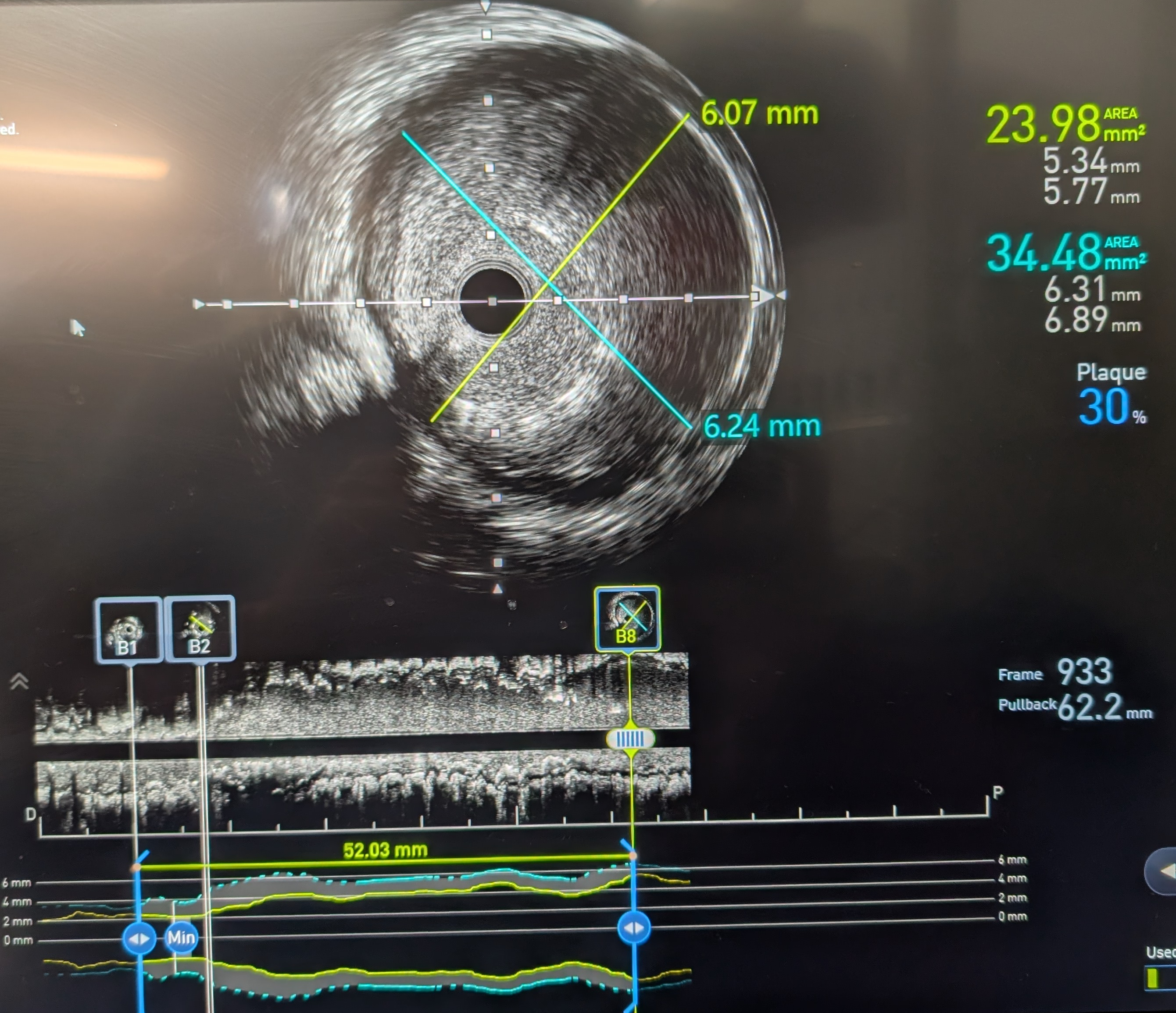
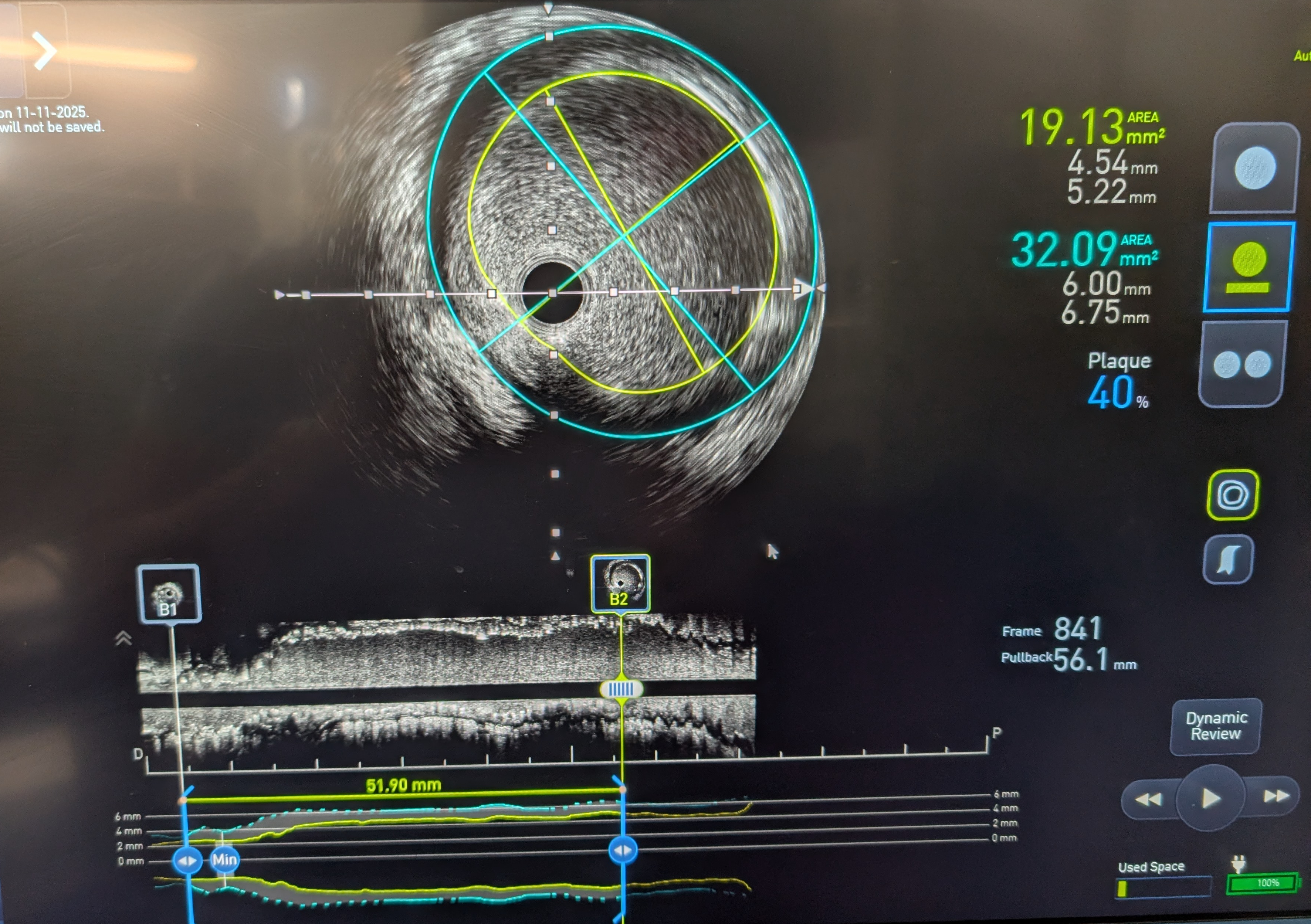
Intracoronary GTN was given after predilatation. IVUS showed mostly fibrous plaque with plaque extending from the distal RCA to the proximal RPDA. Reference diameters (EEL) were 4.5mm proximally in the distal RCA and 2.75mm distally in the RPDA. PCI to the distal RCA to RPDA with a provisional approach, using a stent with high postdilatation limits across the bifurcation.


 RCA AP Cranial stent prox edge postdiln.mp4
RCA AP Cranial stent prox edge postdiln.mp4
IVUS after postdilatation showed unravelling and severe malapposition.mp4
Interventional Management
Procedural Step
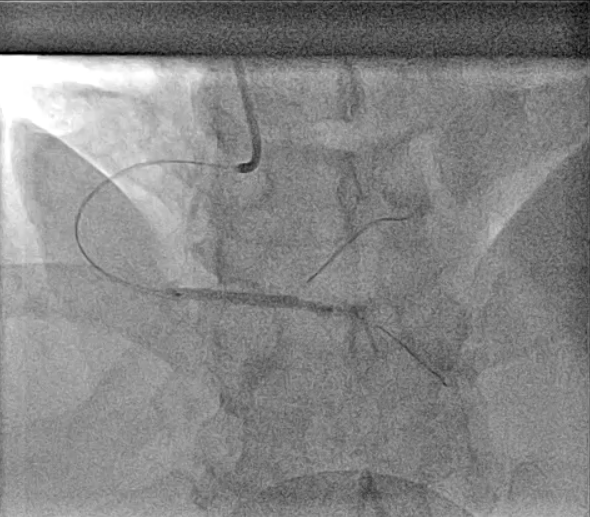
PCI was performed with a 7Fr JR4 Guide with wires in the RPDA and RPL. Lesion was predilated and stented with a 2.75x33m DES and postdilated with a 4.5mm NC proximal to the RCA bifurcation. IVUS showed underexpansion distally and severe malapposition proximally hence the stent was further postdilated with 2.75mm NC distally and 4.5mm in the distal RCA. ClearStent showed unravelling of the stent, which was confirmed on IVUS with a new total stent length of 52mm. The distal RCA diameter had grown in size to 5mm at the site of the proximal stent edge. A 4.5x24mm DES was implanted in the distal RCA to cover the unravelled stent struts, which was postdilated with a 5mm NC balloon. Final IVUS showed the stent to have adequate apposition with no immediate complications.


IVUS final.mp4
RCA AP Cranial Final angio.mp4
Case Summary
This case demonstrates complexities in stenting bifurcation lesions with severe size mismatch. Stents with high postdilatation limits are designed for such cases but despite staying within the limits, the stent architecture may still be compromised due to a variety of reasons. Techniques that can be used to avoid stent unravelling are to stay within postdilatation limits, postdilate from proximal edge to carina, and to wait for full balloon deflation before movement. Vigilance on stent architecture, particularly during ClearStent can aid to detect unravelling early. Once detected, options are to postdilate the proximal stent or to implant a new stent to cover the unravelled stent struts.