Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251113_005
Catastrophic Forearm Compartment Syndrome Following Transradial PCI: How Early Detection and Emergent Fasciotomy Saved the Limb
By Mohammad Satyabhisma
Presenter
Mohammad Satyabhisma
Authors
Mohammad Satyabhisma1
Affiliation
CKU - International St. Mary Hospital, Korea (Republic of)1
View Study Report
CASE20251113_005
Coronary - Complication Management
Catastrophic Forearm Compartment Syndrome Following Transradial PCI: How Early Detection and Emergent Fasciotomy Saved the Limb
Mohammad Satyabhisma1
CKU - International St. Mary Hospital, Korea (Republic of)1
Clinical Information
Relevant Clinical History and Physical Exam
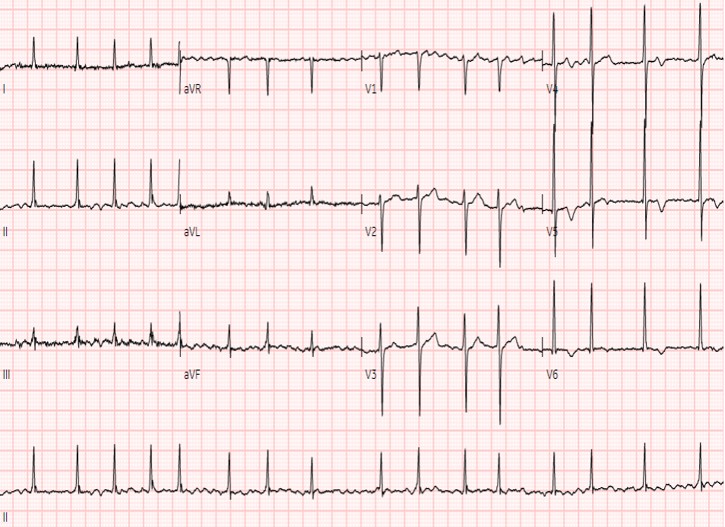
A 58-year-old woman with a 2-week history of exertional chest pain was referred for new-onset atrial fibrillation. She had history of smoking cigarettes about 10 cigarettes per day and drank alcohol several days per week. On arrival she was hemodynamically stable and afebrile, with an irregularly irregular pulse, no heart failure signs, clear lungs, and mild cardiomegaly on chest X-ray.

Relevant Test Results Prior to Catheterization
ECG showed atrial fibrillation with a moderate ventricular response and no ST-segment elevation. Serial cardiac troponin levels were elevated, consistent with non–ST-elevation myocardial infarction. Baseline hemoglobin, platelet count, creatinine, and coagulation profile were normal. Transthoracic echocardiography demonstrated preserved LV systolic function and no visible left atrial thrombus.
Relevant Catheterization Findings
Coronary angiography via a right radial 4 Fr sheath showed a normal right coronary artery. The left system revealed abrupt occlusion of a distal ramus intermedius branch with a smooth proximal segment and no other significant stenoses, favoring coronary embolism related to atrial fibrillation. After upsizing to a 6 Fr guiding catheter and wiring the branch with a 0.014″ coronary guidewire, gentle wire manipulation restored TIMI 3 flow.
 ap0 cra 30.mp4
ap0 cra 30.mp4
Media1LCAAWAL.mp4
rao30cra30.mp4
Interventional Management
Procedural Step
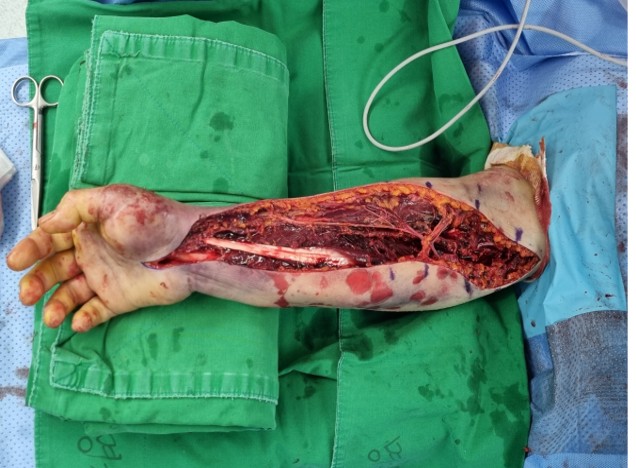
PCI was performed via right radial access using a 4 Fr sheath for diagnostic angiography, which showed an embolic-appearing distal ramus intermedius (RI) occlusion with otherwise non-obstructive coronaries. The sheath was upsized to 6 Fr and a 6 Fr extra-backup guiding catheter was used to wire the RI with a 0.014" workhorse guidewire. Gentle wire manipulation fragmented the embolus and restored TIMI 3 flow without ballooning or stent implantation. The sheath was removed and a radial compression band applied; the forearm was soft with intact pulses. Because the infarct was judged AF-related, an intravenous unfractionated heparin infusion was started about 20:30 in addition to dual antiplatelet therapy. Within an hour, oozing at the puncture site led to repeated tightening of the band, addition of an elastic bandage, and a progressively enlarging forearm hematoma. Heparin was discontinued only around 23:00, roughly 3 hours after bleeding was first recognized. Overnight, the patient developed recurrent numbness, then sudden excruciating pain, tense swelling, and loss of active hand motion at 04:00, consistent with acute compartment syndrome. CT angiography showed a large volar hematoma and non-visualization of the distal brachial artery, prompting emergent dual-incision forearm fasciotomy with evacuation of hematoma and ligation of an injured radial artery segment.


mecha fragmentation.mp4
Case Summary
Forearm compartment syndrome is a rare but limb-threatening complication of transradial PCI, particularly in anticoagulated patients. In this AF-related embolic NSTEMI, sheath upsizing, ongoing heparin, and tight compression allowed an access-site bleed to progress to compartment syndrome. Pain out of proportion, recurrent paresthesia, tense swelling, and bullae were key warning signs. Rapid recognition and emergent fasciotomy led to full neurologic recovery.