Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251113_003
A Triple Complex and High-Risk PCI: Rotacut Strategy for Heavily Calcified Right Coronary Artery CTO on IABP Support
By Shamshad Alam Alam, Sushil Kumar
Presenter
Shamshad Alam Alam
Authors
Shamshad Alam Alam1, Sushil Kumar1
Affiliation
Jayprabha Medanta Superspeciality Hospital, India1
View Study Report
CASE20251113_003
Coronary - Hemodynamic Support
A Triple Complex and High-Risk PCI: Rotacut Strategy for Heavily Calcified Right Coronary Artery CTO on IABP Support
Shamshad Alam Alam1, Sushil Kumar1
Jayprabha Medanta Superspeciality Hospital, India1
Clinical Information
Relevant Clinical History and Physical Exam
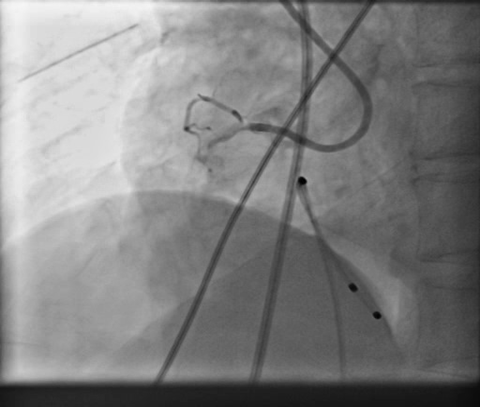
•Thisa case of 72 years male who presented to us with inferior wall STEMI, completeheart block with delayed presentation in cardiogenic shock and severe LV dysfunction. Patientwas put on temporary pacing support, IABP support and coronary angiogram wasdone which revealed TVD with rightcoronary artery had near total occlusion with extensive calcification alongwithsignificant calcified stenosis in left system. Heart team meeting done urgently and planned to go for high risk PCI.
Relevant Test Results Prior to Catheterization
patient being a high risk was taken for catheterisation and PCI and was on temporary pacing support as well as IABP support. his troponin levels were very high and a bedside echocardiogram revealed severe LV dysfunction with LVEF - 25% with moderate to severe mitral regurgitation.
Relevant Catheterization Findings
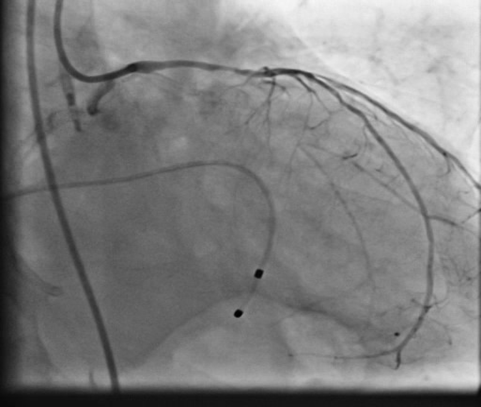
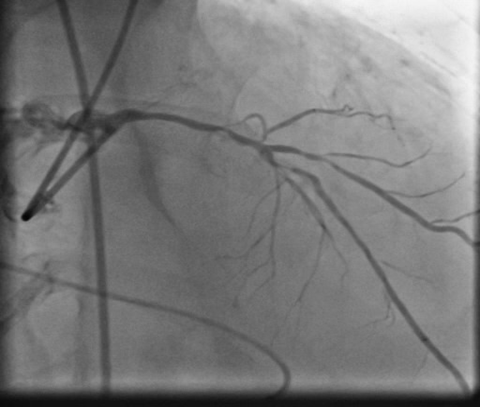
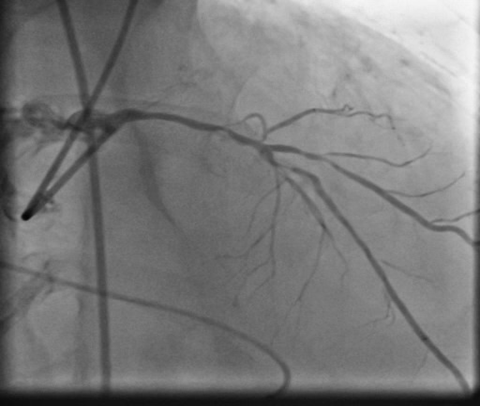
patient underwent coronary angiogram which revealed calcified triple vessel disease with near total occlusion of proximal RCA and 80% calcified stenosis in mid LAD with diseased small circumflex artery. In view of very high surgical risk he was turned down by surgical team and was advised for a high risk PCI of infarct related artery on hemodynamic support in form of IABP which was only mechanical circulatory support available apart from VA-ECMO.
Interventional Management
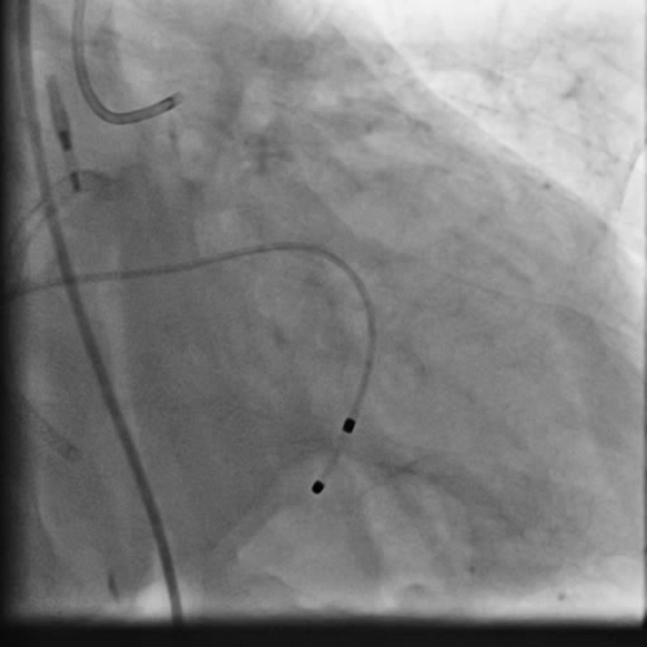
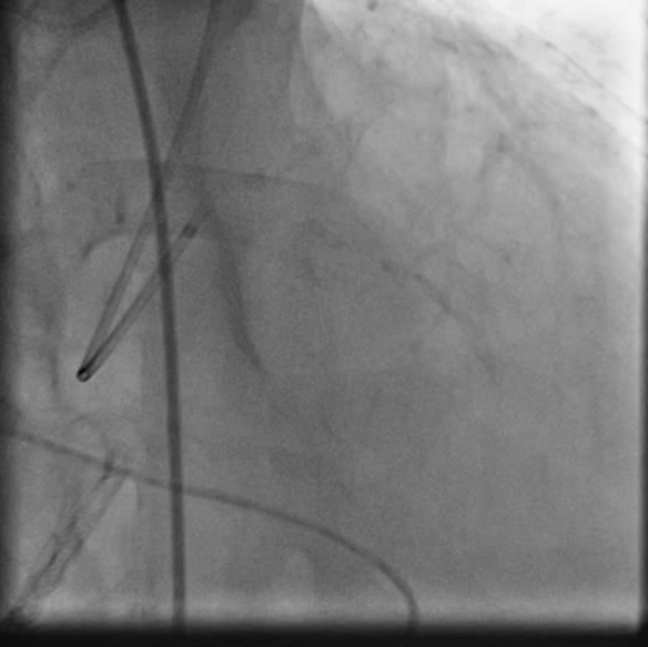
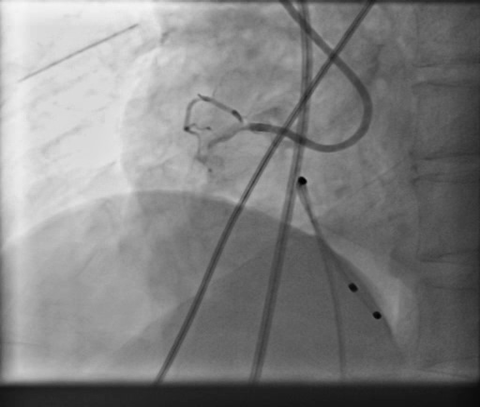
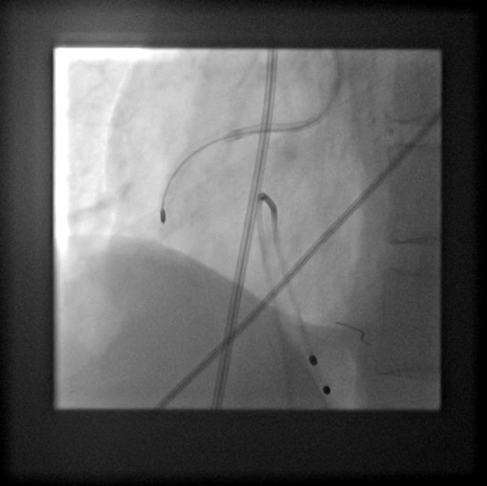
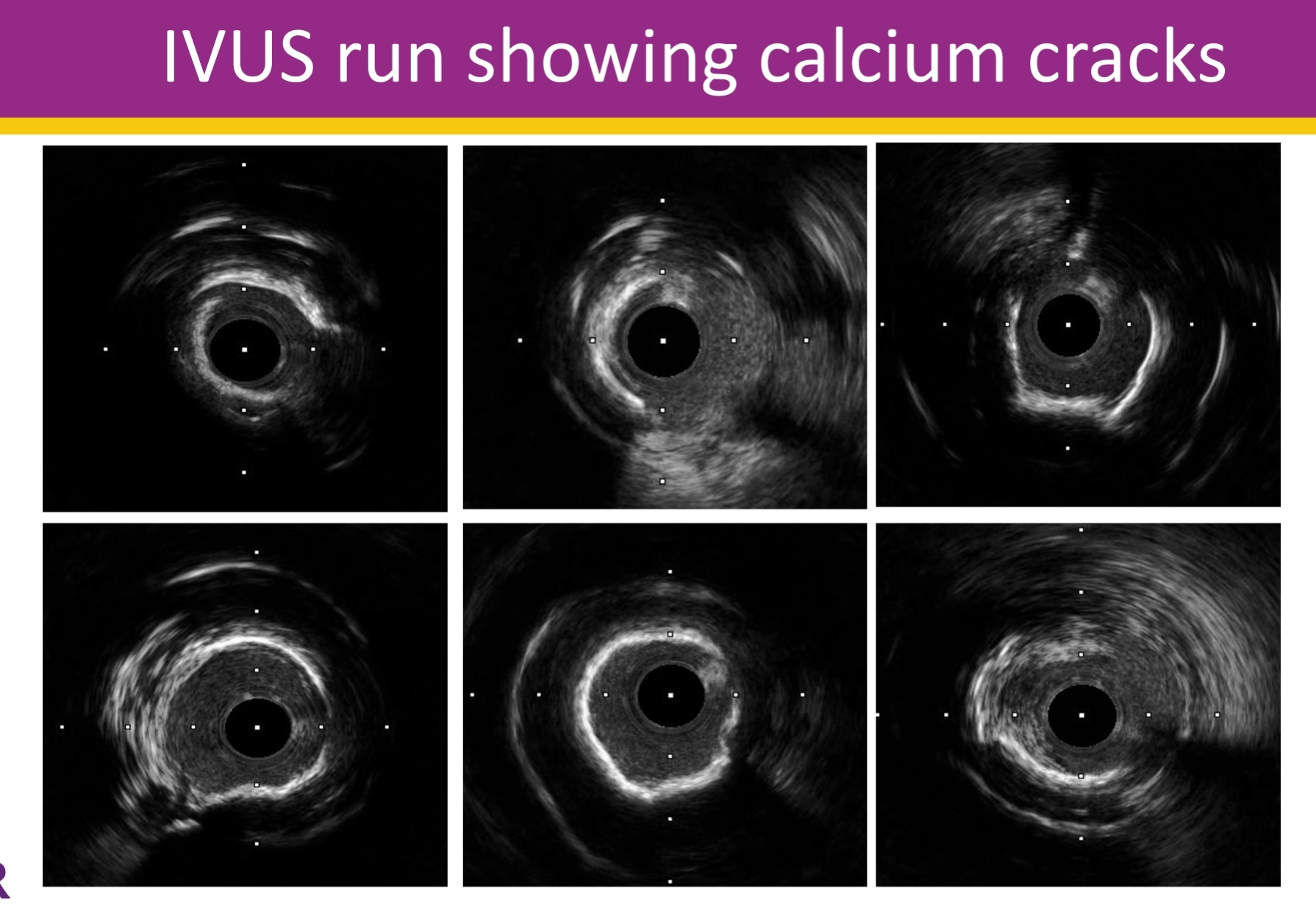
Procedural Step
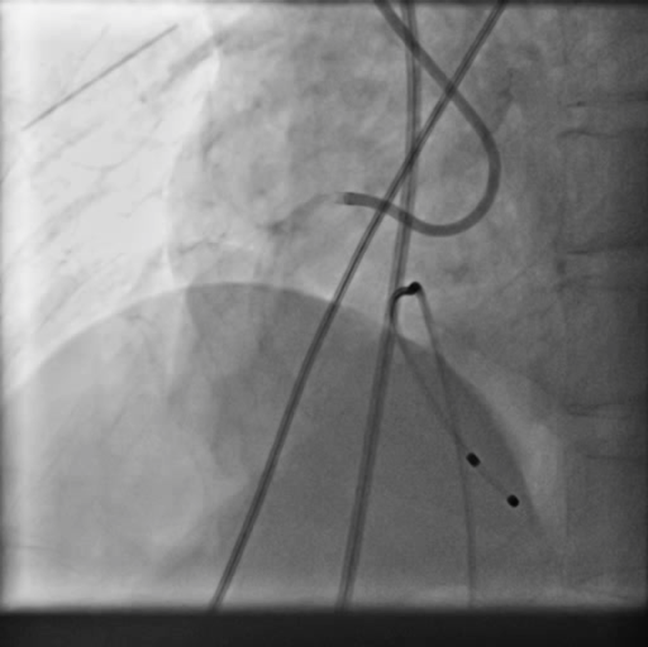
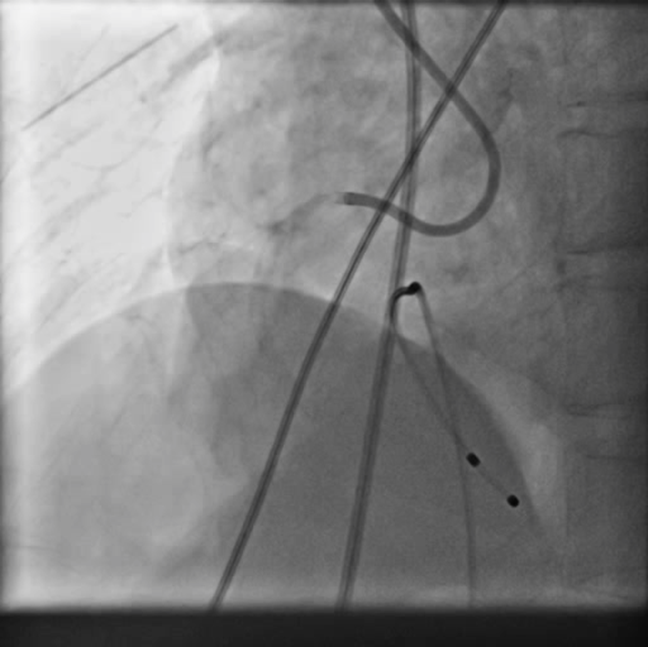
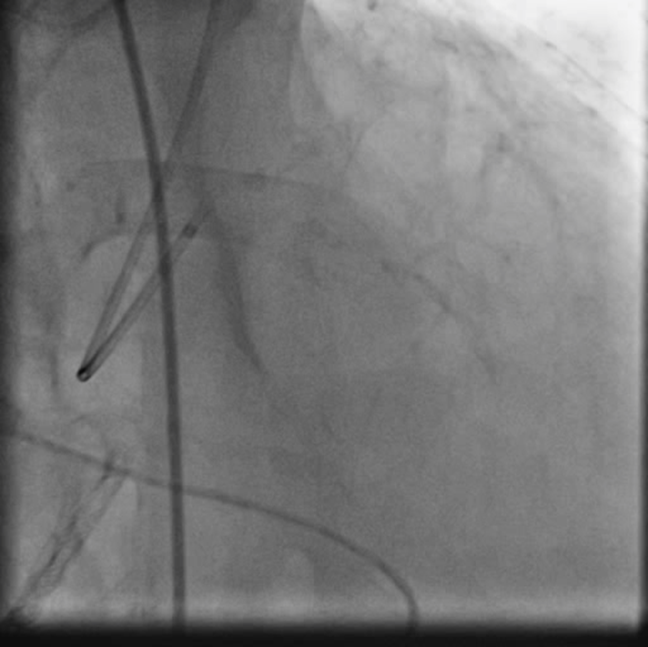
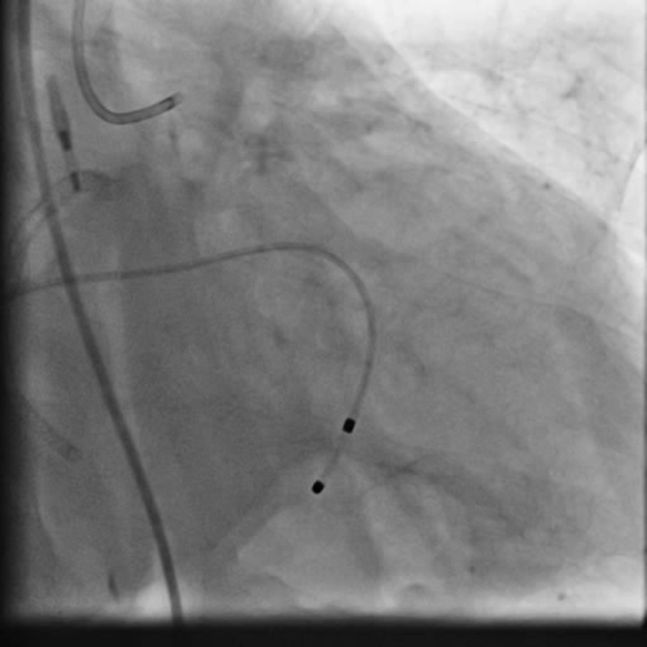
PCIof right coronary artery was initiated on IABP support with amplatz left1 guided catheter and vessel was crossed with great difficulty in repeatedattempts by fielder XT followed by GAIA 2 wire over corsair microcatheter. Microcathetercould not be crossed beyond mid segment calcified CTO, so balloon dilation with0.75 mm balloon was done after which again microcatheter could not be trackedbeyond mid part. Butwe were able to exchange wire to allstar followed by rotawire byplacing microcatheter in mid segment after balloon dilation by 0.75 mm balloon. Rotablation wasdone with 1.25 mm burr at 1,60,00 rpm repeatedly from proximal to mid distalpart. Lesionstill looked unprepared as repeated postdilation with2.25*15 mm followed by 2.5*15 mm non compliant balloon at high pressures showedunexpanded balloon. Againlesion preparation was done with 2.5*15 mm wolverine cutting balloon repeatedlyat high pressures which led to adequate luminal gain and calcium cracks as seenon IVUS run. AfterIVUS run again high pressure balloon dilation was done with wolverine 2.5*15 mmballoon followed by 2.5*12 mm non compliant balloon at 28 atm toadequately prepare the lesion before stent deployment. Stentingwas done with 2.5*32 mm DES, 2.75*32 mm DES, and 3*24 mm DES from distal toproximal in overlapping fashion. Thenfinally high pressure post dilation was done with 2.75*15 mm followed by 3*15mm non compliant balloon and adequate stent expansion was achieved with TIMI 3 flow.
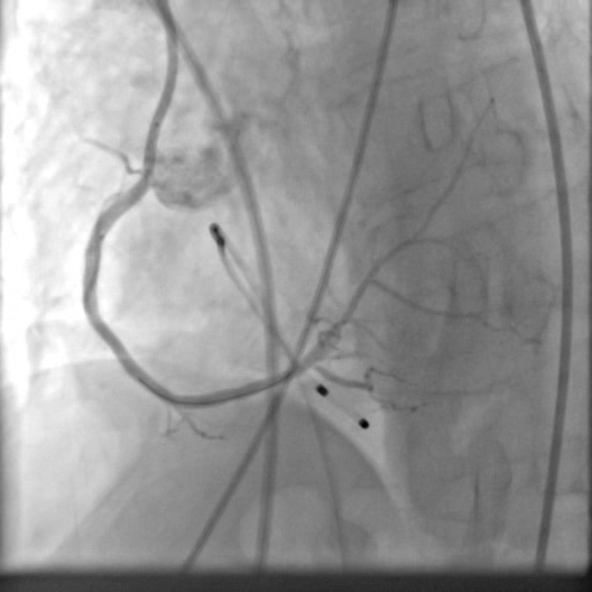
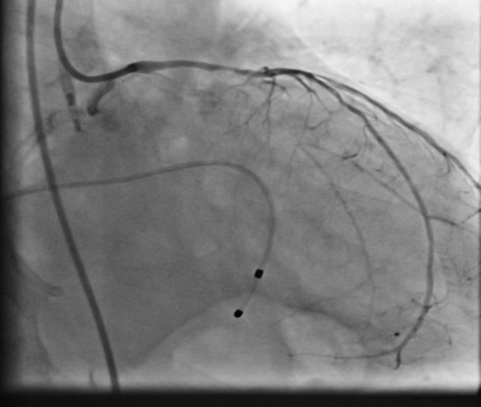
Case Summary
Rightcoronary artery was well revascularized with adequate stent expansion and nosignificant complications. Patientwas weaned off from IABP support next day and regained his rhythm after 2 daysand then temporary pacemaker support was removed. Hewas planned for a staged rotablationguided PCI to left coronary system as he developed mild renal dysfunction whichgradually improved in hospital before discharge.
Ideally Impella should be the choice as mechanical circulatory support system and IABP or ECMO should be used only in case of its availability. in cardiogenic shock infarct related vessel should only be dealt when a complex procedure is required by non infarct related vessels too.