Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251113_001
Transforming the Impossible Into the Feasible: A Contemporary PCI Approach to True Left Main Trifurcation Disease (Medina 1-1-1-1) Using Trissing Technique
By Lidya Pertiwi Suhandoko, Dwi Ariyanti, Rachmat Ageng Prastowo, Suryo Ardi Hutomo, I Gde Rurus Suryawan
Presenter
Lidya Pertiwi Suhandoko
Authors
Lidya Pertiwi Suhandoko1, Dwi Ariyanti1, Rachmat Ageng Prastowo1, Suryo Ardi Hutomo1, I Gde Rurus Suryawan1
Affiliation
Cardiology and Vascular Medicine, Airlangga University, Soetomo General Hospital, Surabaya, Indonesia1
View Study Report
CASE20251113_001
Coronary - Complex PCI - Bifurcation
Transforming the Impossible Into the Feasible: A Contemporary PCI Approach to True Left Main Trifurcation Disease (Medina 1-1-1-1) Using Trissing Technique
Lidya Pertiwi Suhandoko1, Dwi Ariyanti1, Rachmat Ageng Prastowo1, Suryo Ardi Hutomo1, I Gde Rurus Suryawan1
Cardiology and Vascular Medicine, Airlangga University, Soetomo General Hospital, Surabaya, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A 78-year-old male with stable angina, hypertension, overweight, and mild acute kidney injury presented with significant left main and three-vessel coronary artery disease. He had a 13-year history of coronary artery disease, had previously declined CABG, and was managed medically with clopidogrel, atorvastatin, bisoprolol, and candesartan. Echocardiography revealed a preserved ejection fraction (54%) with segmental hypokinesis. Laboratory tests showed mild renal impairment and normal hemoglobin levels.
Relevant Test Results Prior to Catheterization
Electrocardiography revealed sinus bradycardia 54 bpm, incomplete right bundle branch block, and pathological Q waves in inferior leads suggestive of prior inferior myocardial infarction. Transthoracic echocardiography confirmed preserved left ventricular ejection fraction with segmental hypokinesis in LAD and LCx territories. Laboratory values: hemoglobin 13.6 g/dL, serum creatinine 1.19 mg/dL (eGFR 63), Kalium 4.4, Albumin 4.42, LDL cholesterol 64, SYNTAX score 34.
Relevant Catheterization Findings
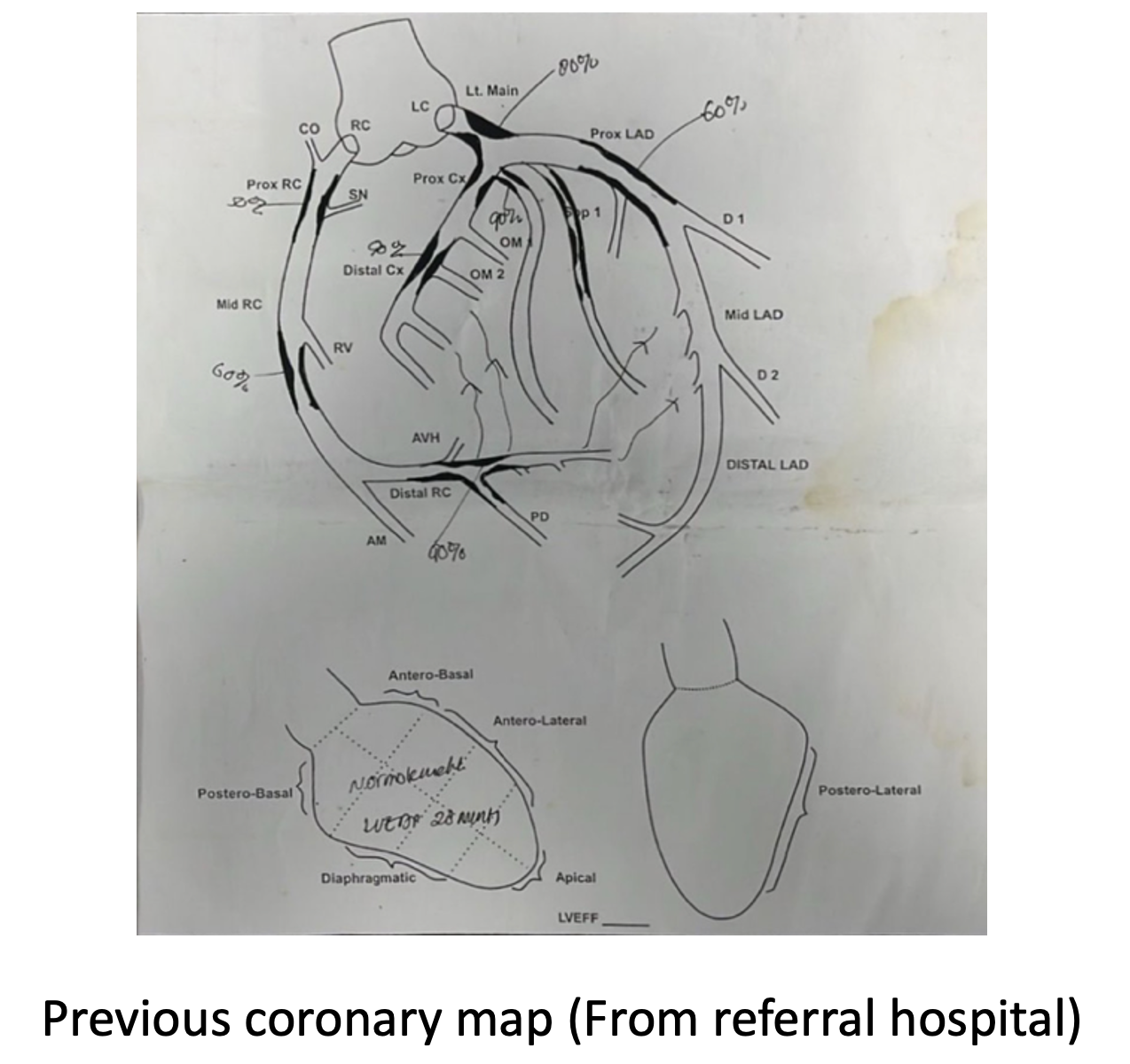
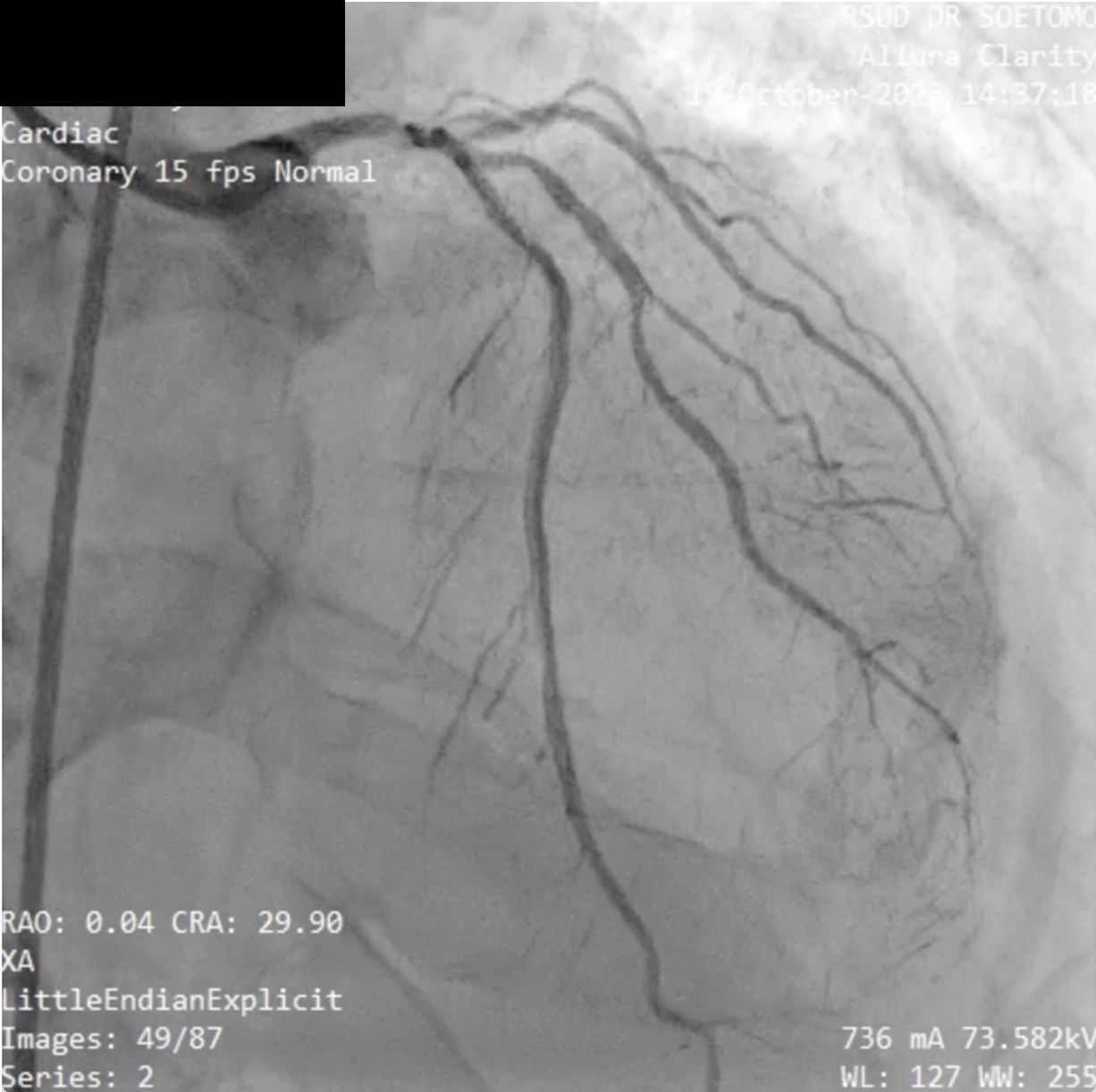
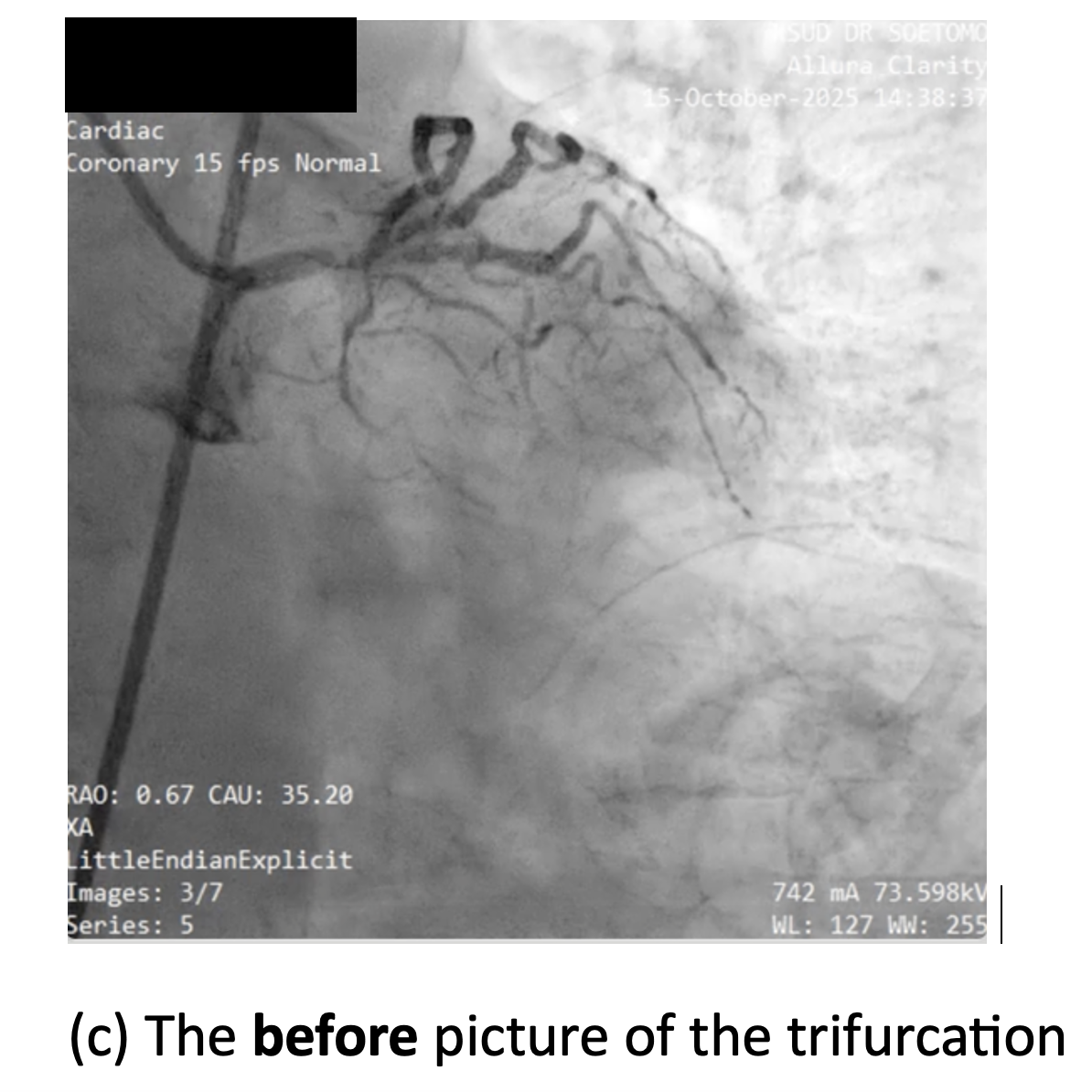
Diagnostic coronary angiography revealed a right-dominant coronary circulation with 80% distal left main stenosis involving the LAD, LCx, and Ramus Intermedius (Medina 1-1-1-1 true trifurcation). The LAD showed 90% ostial-proximal stenosis, the LCx 90% ostial stenosis, and the RI 90% proximal stenosis. There was a non-significant 40% stenosis at the mid-distal RCA with extensive collateral flow to the distal LCx, LAD, and septal branches via the conus branch, RPLB, and RPDA.
 WhatsApp Video 2025-11-14 at 20.47.20.mp4
WhatsApp Video 2025-11-14 at 20.47.20.mp4
WhatsApp Video 2025-11-14 at 20.47.36.mp4
WhatsApp Video 2025-11-14 at 20.47.58.mp4
Interventional Management
Procedural Step
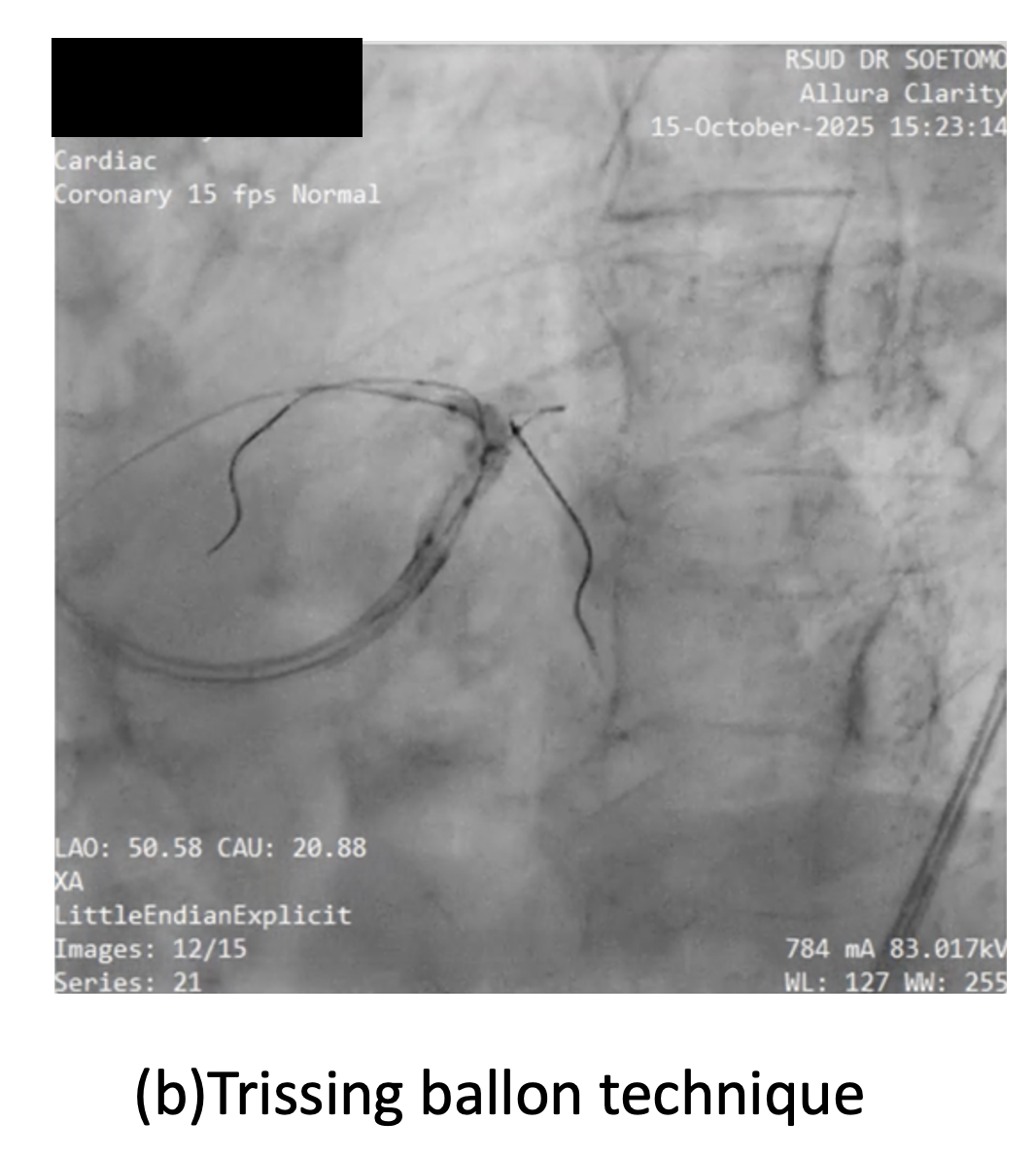
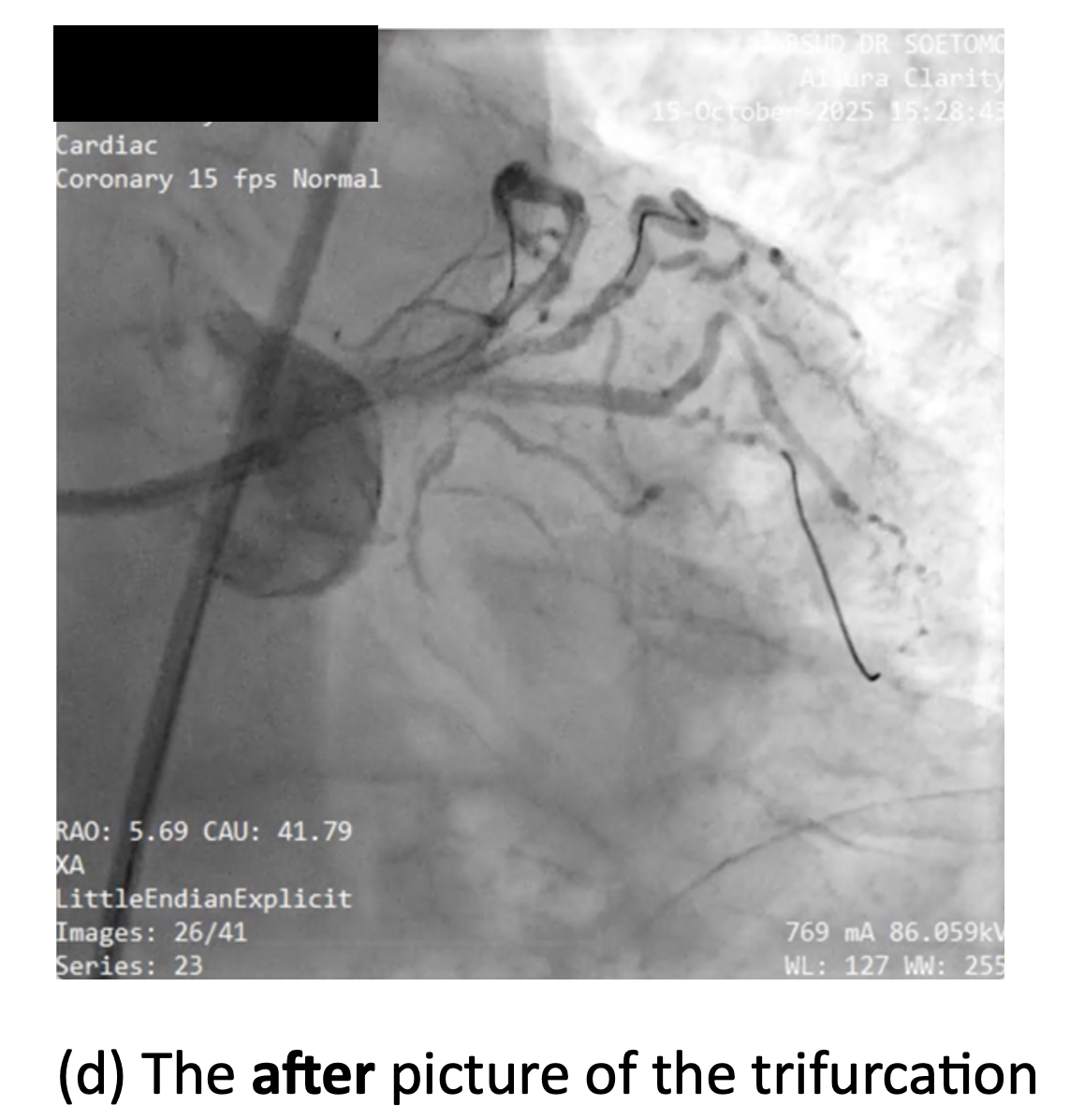
Using right femoral access with 7F long sheath, elective PCI was performed employing a Triple-kissing-balloon (Trissing) technique used for trifurcation lesions. The technique consisted of:
1.mp4
2.mp4
3.mp4
Case Summary
This case demonstrates the feasibility and safety of the Trissing technique (simultaneous three-balloon inflation) for true left main trifurcation disease (Medina 1-1-1-1) in a high SYNTAX score patient. The three-stent strategy, achieved complete revascularization with optimal angiographic results and no complications. The Trissing technique proved essential for preserving all three branch ostia and ensuring proper stent apposition at the trifurcation polygon of confluence. This technique is feasible when CABG is declined, with careful selection and planning. Further studies are needed to standardize this technique for wider usage in complex left main trifurcation PCI.