Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251112_012
The Constricting Current: Unraveling Central Vein Occlusive Disease
By Aaron Christian Earl Vidad, Ricardo Jose Quintos II
Presenter
Aaron Christian Earl Vidad
Authors
Aaron Christian Earl Vidad1, Ricardo Jose Quintos II2
Affiliation
Cardinal Santos Medical Center Cardiovascular Institute, Philippines1, Cardinal Santos Medical Center- Cardiovascular Institute, Philippines2
View Study Report
CASE20251112_012
Endovascular - Venous Disease Intervention
The Constricting Current: Unraveling Central Vein Occlusive Disease
Aaron Christian Earl Vidad1, Ricardo Jose Quintos II2
Cardinal Santos Medical Center Cardiovascular Institute, Philippines1, Cardinal Santos Medical Center- Cardiovascular Institute, Philippines2
Clinical Information
Relevant Clinical History and Physical Exam
80/F with 3 week left arm swelling. Complex history of multiple left arm vascular access procedures (s/p brachioaxillary graft, 2025; s/p brachiocephalic fistula creation, left 2023), complicated by prior infected pseudoaneurysm excision of left brachiocephalic fistula and permanent catheter removal for infective endocarditis. Also s/p PPI for sick sinus syndrome (2023)
Physical findings of dilated superficial veins on anterior chest wall and unilateral left arm swelling and edema

Physical findings of dilated superficial veins on anterior chest wall and unilateral left arm swelling and edema
Relevant Test Results Prior to Catheterization
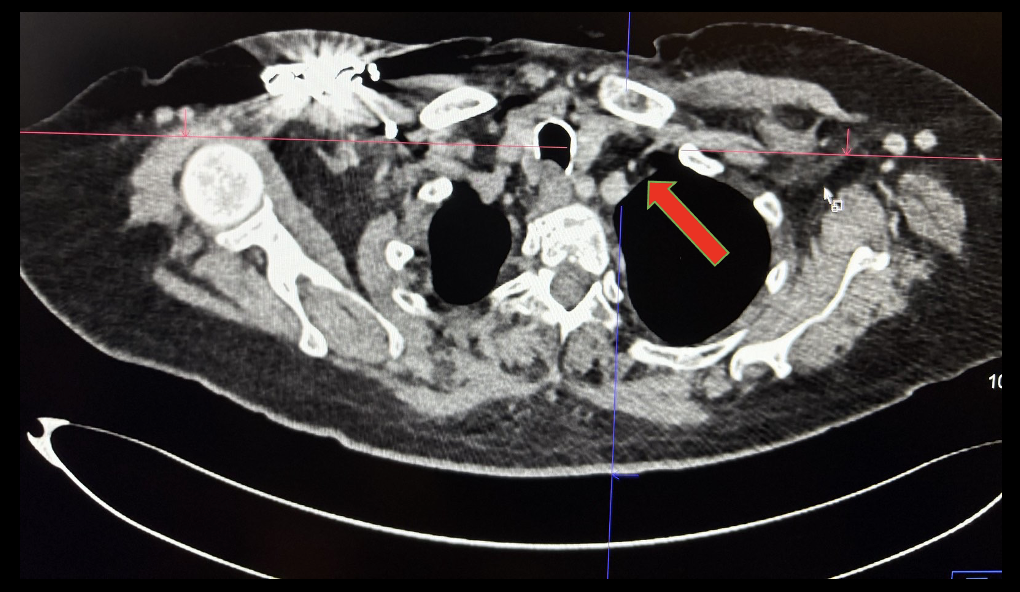
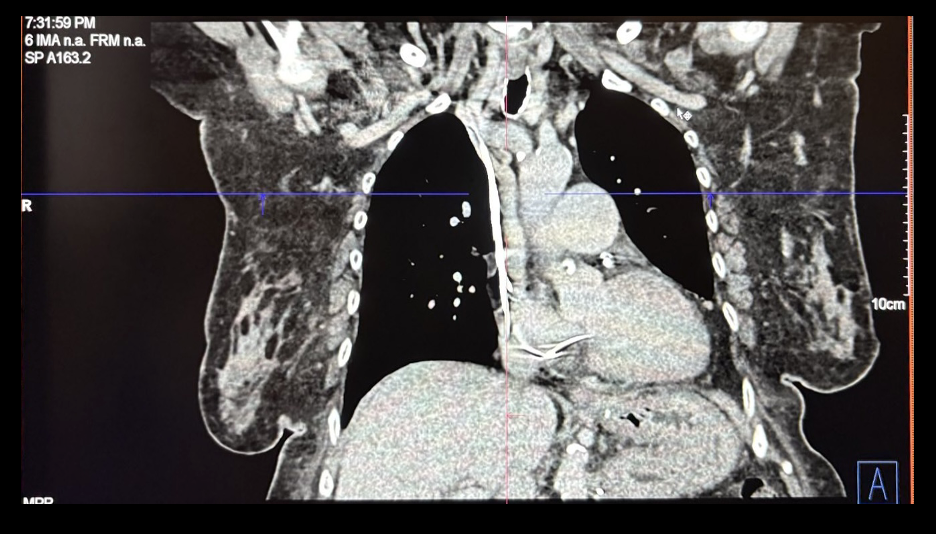
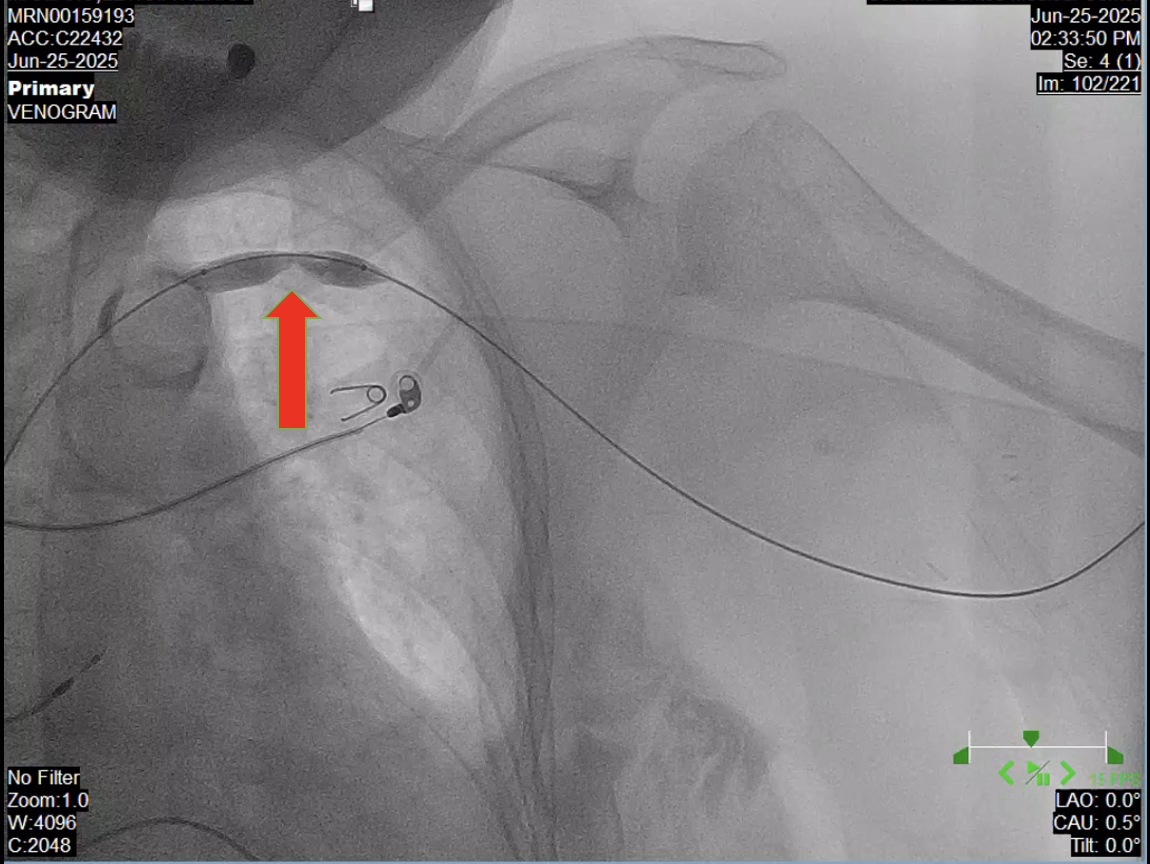
Chest CT venography revealed apparent narrowing of the left subclavian vein (red arrow) just proximal to where it crosses the first anterior ribDuplex Study of the Arteriovenous graft, left brachioaxillary graft noted patent AV fistula with computed flow rate of 2509 mL/min at the mid graft. No evidence of hemodynamically significant stenosis and thrombosis; Honeycombing pattern suggestive of subcutaneous edema
 Duplex Study of Arteriovenous graft, brachioaxillary .mov
Duplex Study of Arteriovenous graft, brachioaxillary .mov
Relevant Catheterization Findings
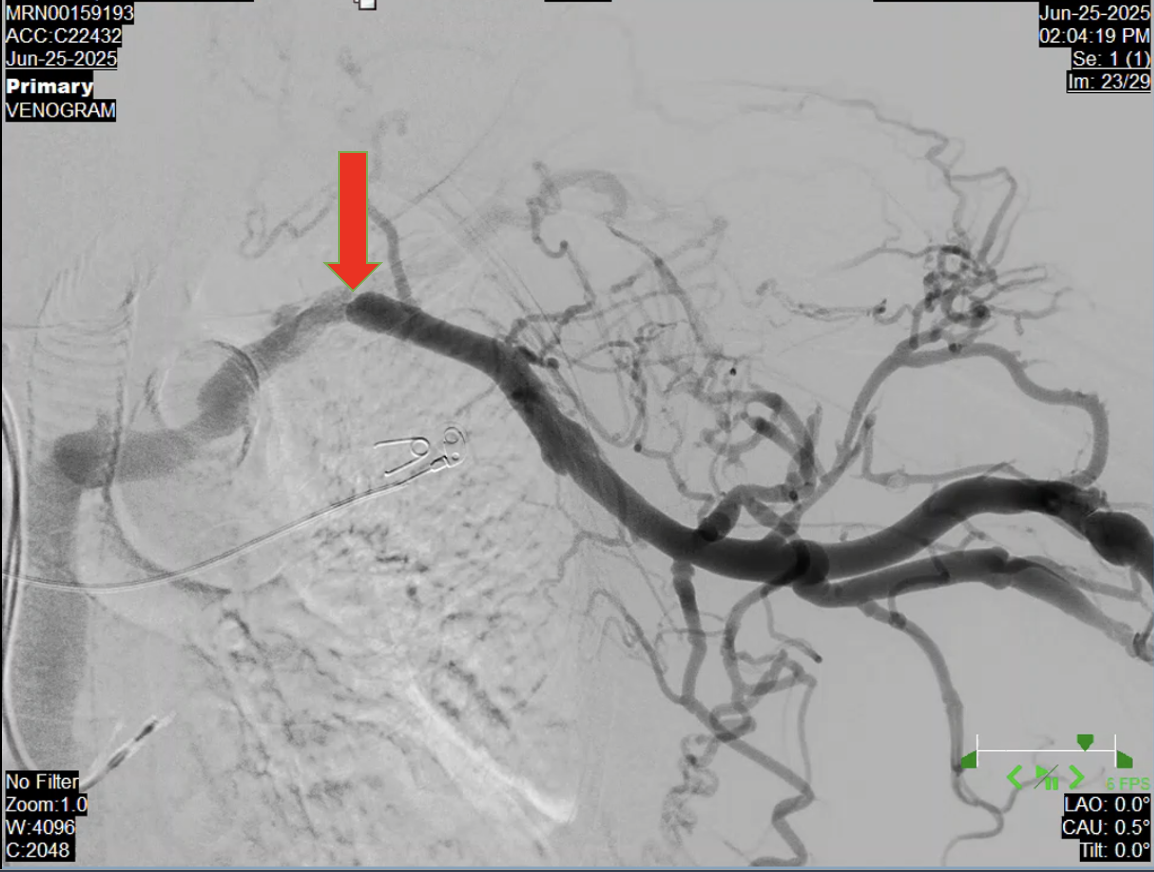
Digital subtraction venography revealed near total occlusion of the left subclavian vein at the level of the first rib wherein measurements taken on the lesion which was noted 90-95% stenosis. Multiple venous collateral formation with faint and sluggish antegrade collateral flow distal to the stenosis.
Digital Subtraction Venography.mov
Interventional Management
Procedural Step
Left brachioaxillary graft was accessed using a Fr 4 hemostatic sheath. Venography done showing stenosis at the left subclavian vein at the level of the first rib. Mesurements taken with a degree of stenosis more than 95%. A balloon catheter was deployed using 10.0 x 40.0 mm Armada Abbott Catheter inflated at 10 atm for 30 seconds with gradual resolution of stenosis. Post venoplasty shots revealed normal contrast flow with disappearance of venous collaterals. No intraprocedural complications noted.

Venoplasty.mov
Post venoplasty.mov
Case Summary
Central vein stenosis is a known complication of indwelling intravascular and cardiac devices such as peripherally inserted central catheters, long term cuffed HD catheters and pacemaker wires. Symptoms such as ipsilateral arm swelling, leading to severe venous dilatation, tortuous collateral veins at the chest may gives us a clue that central occlusive disease may be considered. Duplex ultrasound should be initially done to diagnose and digital subtraction angiography to confirm the case. Endovascular interventions such in this case, percutaneous transluminal angioplasty approach as the promary approach with a primary patency rates of 81% according to literatures.