Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251112_011
Bifascicular Block in Severe Aortic Stenosis: Real-Time Intracardiac Echocardiography–Guided Transcatheter Aortic Valve Implantation to Prevent Complete Atrioventricular Block
By Chia-Hai Chen, Ke-Wei Chen, Ju-Hsin Chang
Presenter
Chia-Hai Chen
Authors
Chia-Hai Chen1, Ke-Wei Chen1, Ju-Hsin Chang1
Affiliation
China Medical University Hospital, Taiwan1
View Study Report
CASE20251112_011
Structural - Aortic Valve Intervention - Complex TAVR
Bifascicular Block in Severe Aortic Stenosis: Real-Time Intracardiac Echocardiography–Guided Transcatheter Aortic Valve Implantation to Prevent Complete Atrioventricular Block
Chia-Hai Chen1, Ke-Wei Chen1, Ju-Hsin Chang1
China Medical University Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 79-year-old male with a history of type 2 diabetes mellitus and end-stage renal disease on maintenance hemodialysis presented with progressive exertional dyspnea over three months. As his symptoms worsened, he sought evaluation at our cardiovascular clinic. Physical examination revealed a grade 4/6 ejection systolic murmur at the aortic area radiating to the apex and both carotid arteries.

Relevant Test Results Prior to Catheterization
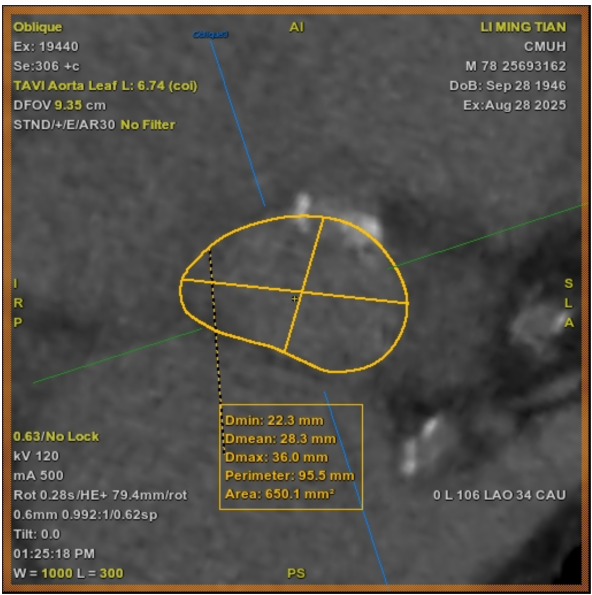
Transthoracic echocardiography revealed severe aortic stenosis (stage D2) with a mean pressure gradient of 24 mmHg and left ventricular ejection fraction 45% showing global hypokinesia. Dobutamine stress echocardiography confirmed severe stenosis (mean gradient 46 mmHg, Vmax 4.45 m/s). CT angiography showed a calcified aortic valve and coronary heights of 14.0 mm (left) and 8.8 mm (right). Coronary angiography revealed no significant disease.
 echo 1.mp4
echo 1.mp4
Relevant Catheterization Findings
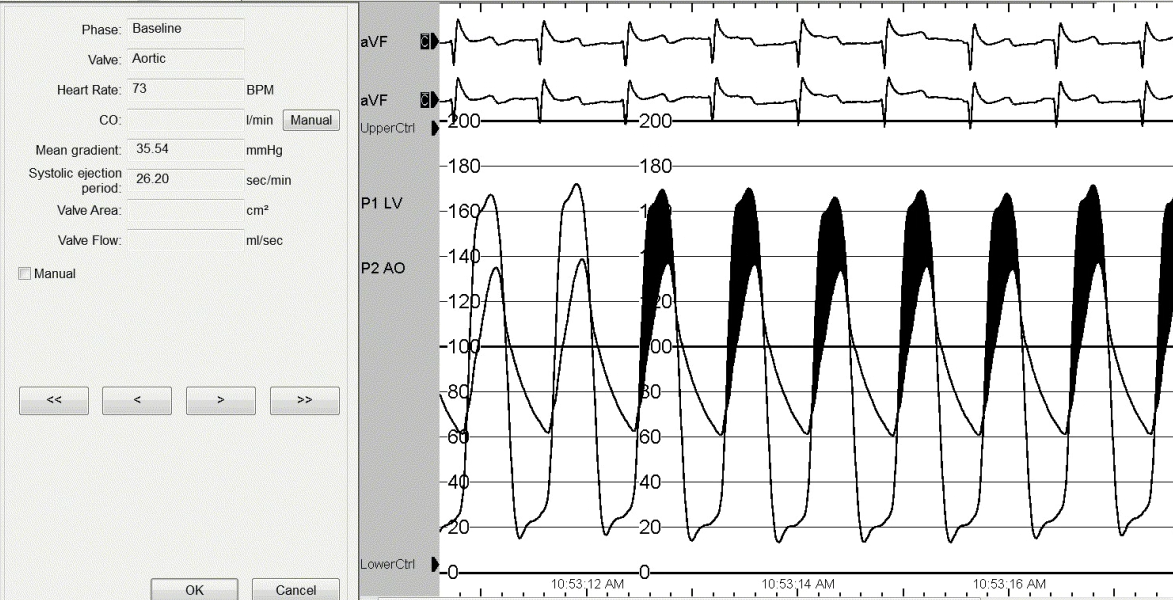
Pre-procedural electrocardiography showed a bifascicular block. Given the high surgical risk and concern for conduction disturbance, a 26-mm short-frame Sapien 3 valve was selected. Intracardiac echocardiography was used for real-time monitoring of valve position and anatomic relationships during implantation. The mean aortic valve pressure gradient measured by catheterization was 35.5 mmHg before valve deployment.

Interventional Management
Procedural Step
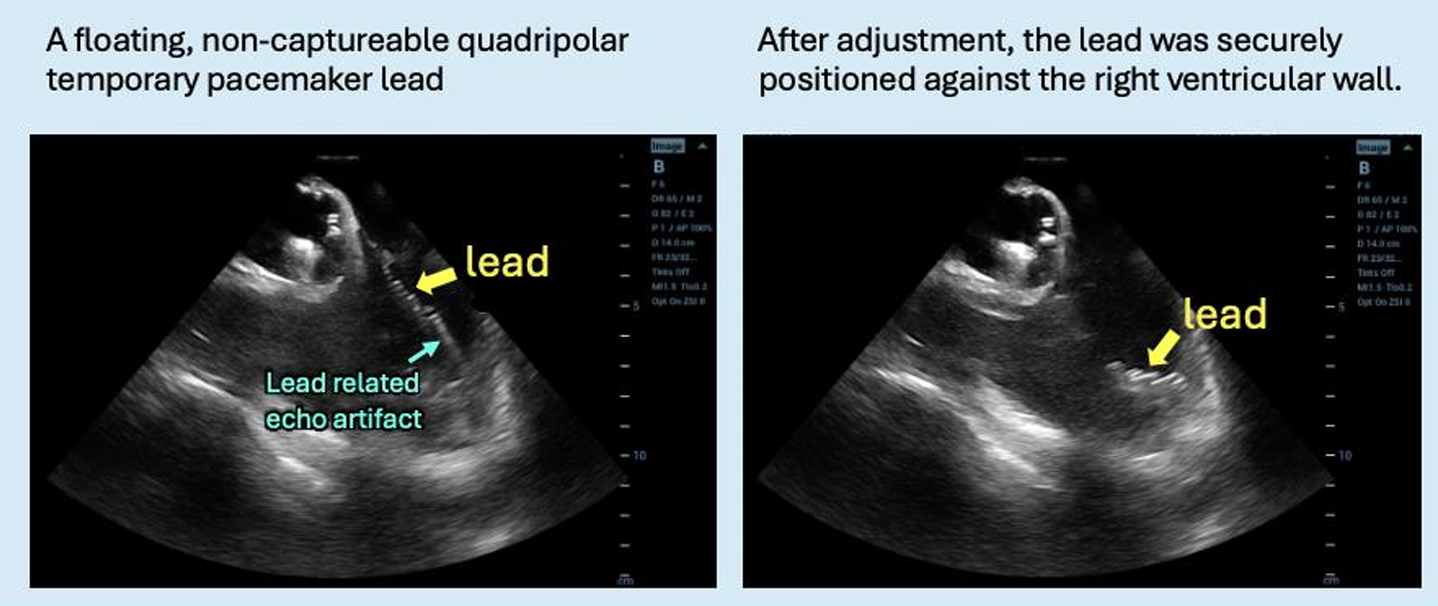
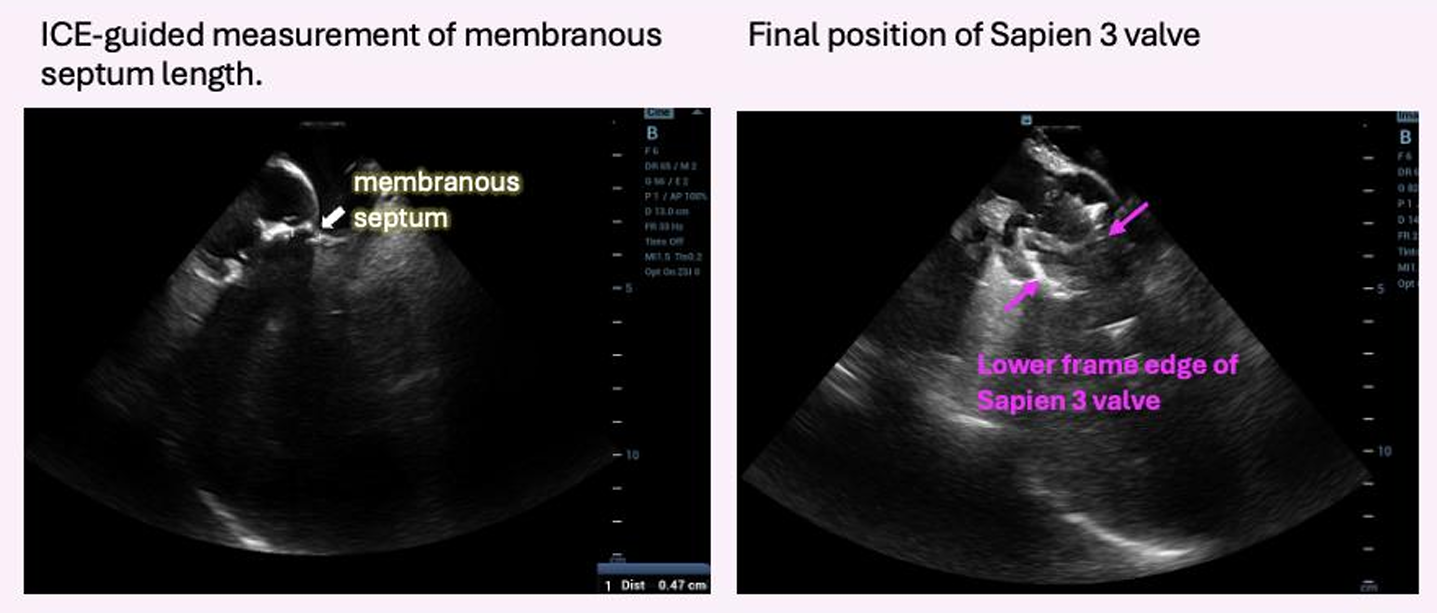
Under general anesthesia, arterial and venous access were obtained via the right femoral artery and vein. A temporary pacing lead was inserted for rapid pacing; however, consistent capture could not be achieved under fluoroscopic guidance. Therefore, intracardiac echocardiography (ICE) was advanced into the right heart to allow precise, close-range localization of the pacing lead. ICE was continuously used to provide real-time monitoring of valve positioning, implantation depth, and the spatial relationship between the transcatheter valve and the membranous septum. A 26-mm Sapien 3 valve was successfully deployed under temporary pacing. Post-deployment angiography and ICE confirmed optimal valve position without conduction disturbance, paravalvular leak, or other complications. The mean aortic valve pressure gradient decreased from 35.5 to 11.2 mmHg. The patient recovered uneventfully after the procedure.
ICE TAVI guided.PNG
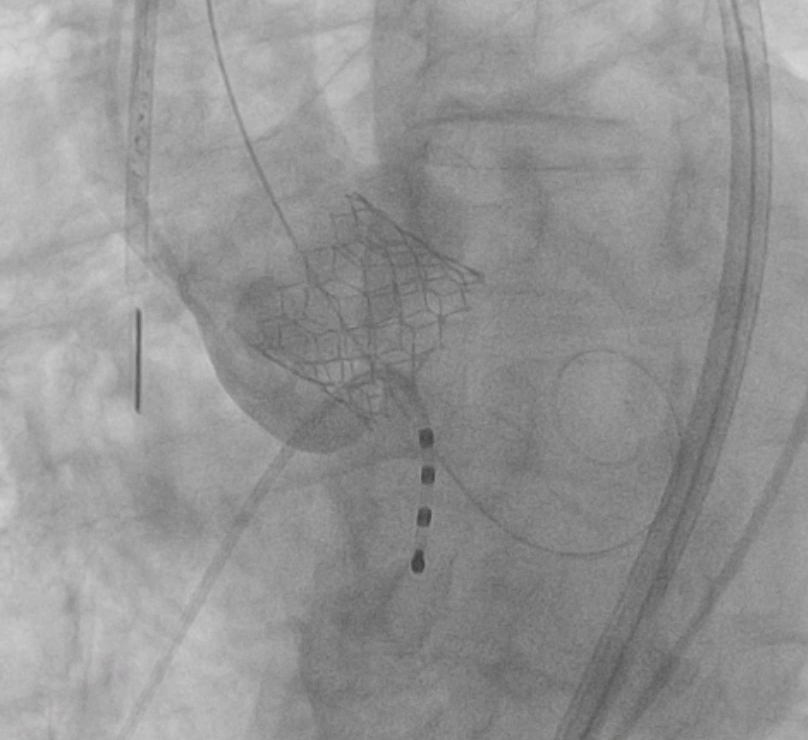
TAVI deploy.PNG
Case Summary
Bifascicular block is a strong predictor of permanent pacemaker implantation after transcatheter aortic valve implantation. Because the conduction system runs through the membranous septum, real-time intracardiac echocardiography (ICE) guidance enables precise depth control and may reduce the risk of new conduction block. In this case, ICE allowed accurate localization of the temporary pacing lead and continuous monitoring of valve positioning during transcatheter heart valve deployment. Postoperative electrocardiography showed no new conduction abnormalities, supporting the role of ICE in improving procedural precision and safety in high-risk patients.