Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251112_010
Critical Calcified Left Main Disease Presenting With Acute Myocardial Infarction and Cardiogenic Shock
By Jin Hien Wong, Zhan Yun Lim
Presenter
Jin Hien Wong
Authors
Jin Hien Wong1, Zhan Yun Lim1
Affiliation
Khoo Teck Puat Hospital, Singapore1
View Study Report
CASE20251112_010
Coronary - Complex PCI - Calcified Lesion
Critical Calcified Left Main Disease Presenting With Acute Myocardial Infarction and Cardiogenic Shock
Jin Hien Wong1, Zhan Yun Lim1
Khoo Teck Puat Hospital, Singapore1
Clinical Information
Relevant Clinical History and Physical Exam
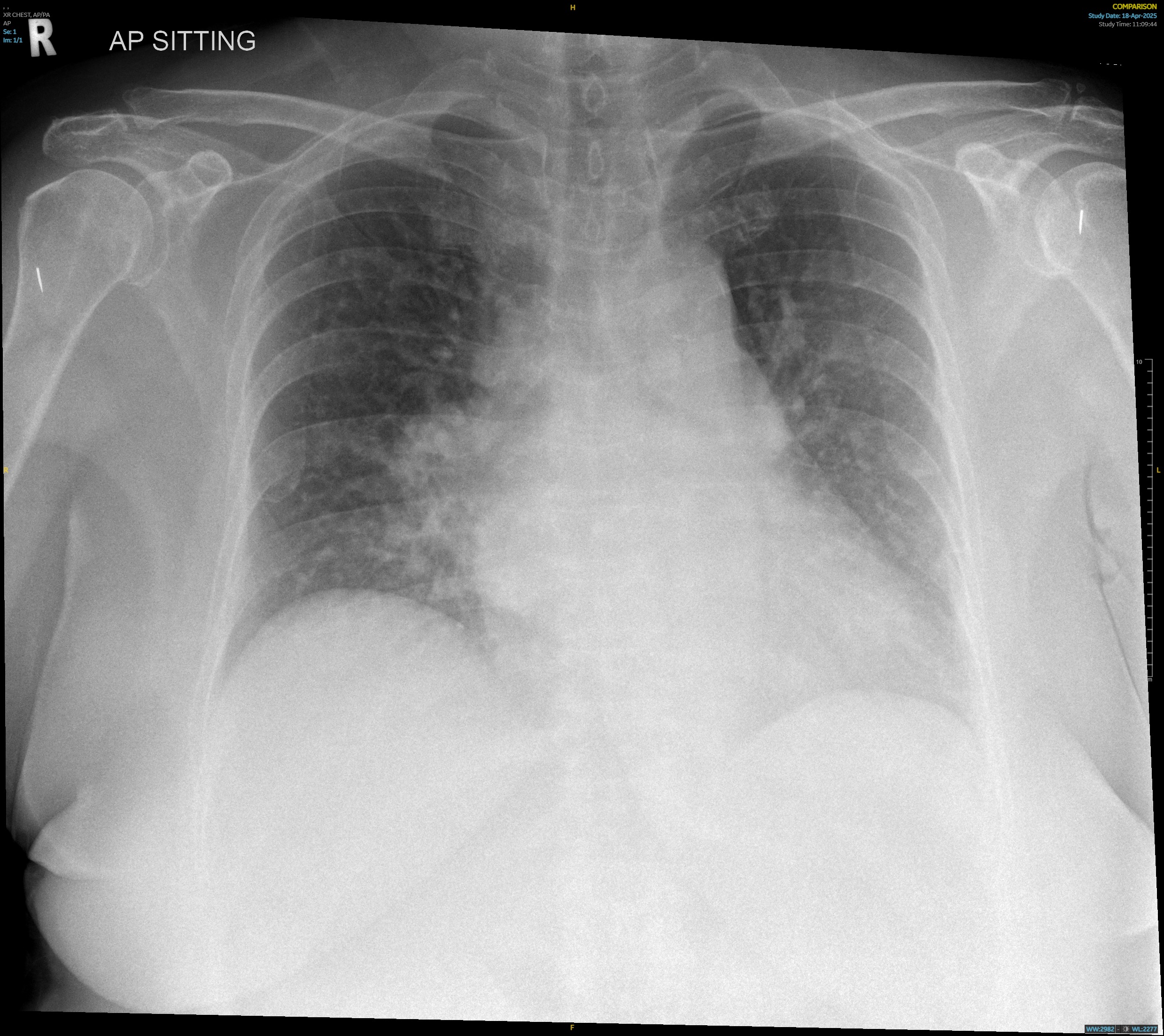
A 71-year-old female presented to theemergency department overnight with shortness of breath. High sensitivityTroponin T was elevated at 3415ng/L. She rapidly developed worsening hypoxiarequiring intubation, and clinical picture was consistent with worseningcardiogenic shock and acute pulmonary oedema. Due to her rapidly deterioratingcondition, she was taken to the cardiac catheterisation lab early forconsideration of upfront revascularisation and mechanical circulatory support.
Relevant Test Results Prior to Catheterization
Troponin T continued to uptrend post-intubation and repeat12-lead electrocardiogram (ECG) showed worsening widespread depressions withAVR elevation. Chest X-Ray post-intubation showed rapidly worsening bilateralinfiltrates compared to admission. Bedside ultrasound showed a severely reducedleft ventricular ejection fraction.

Relevant Catheterization Findings
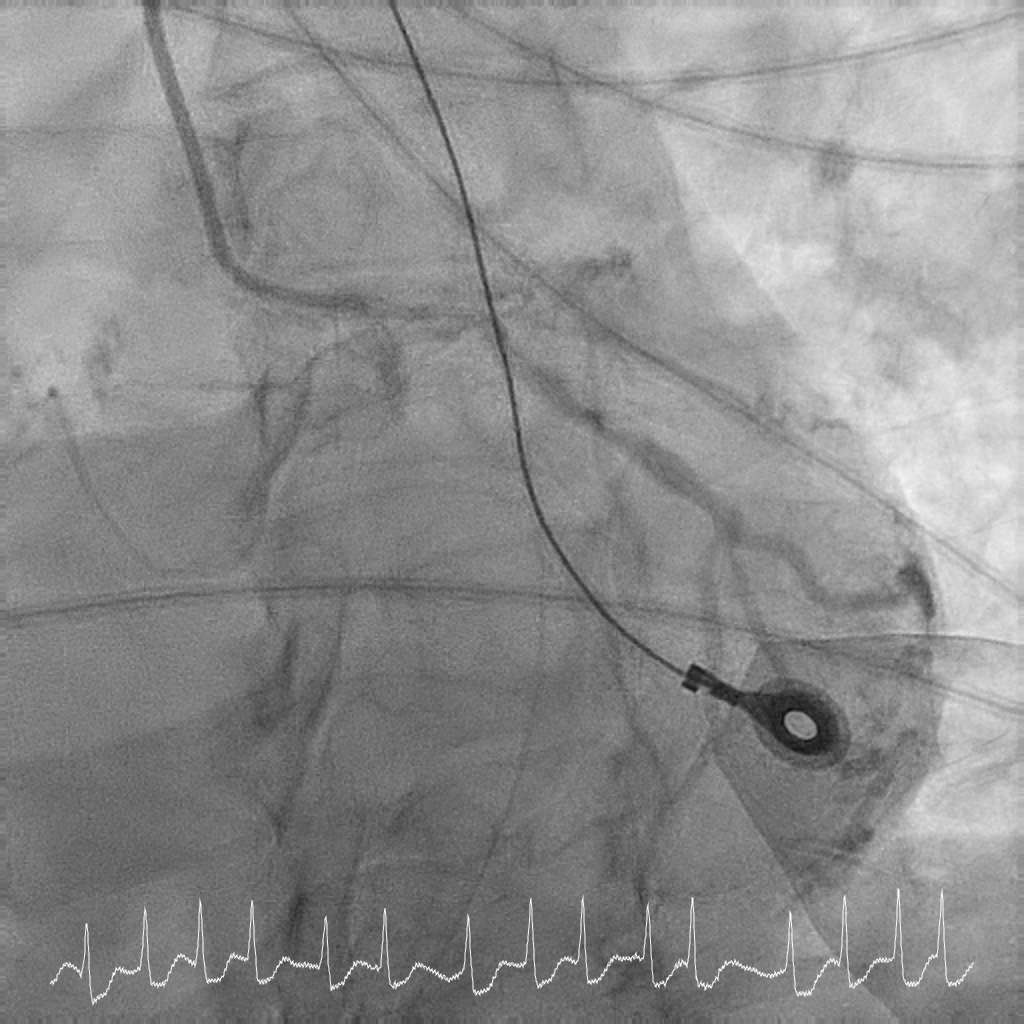
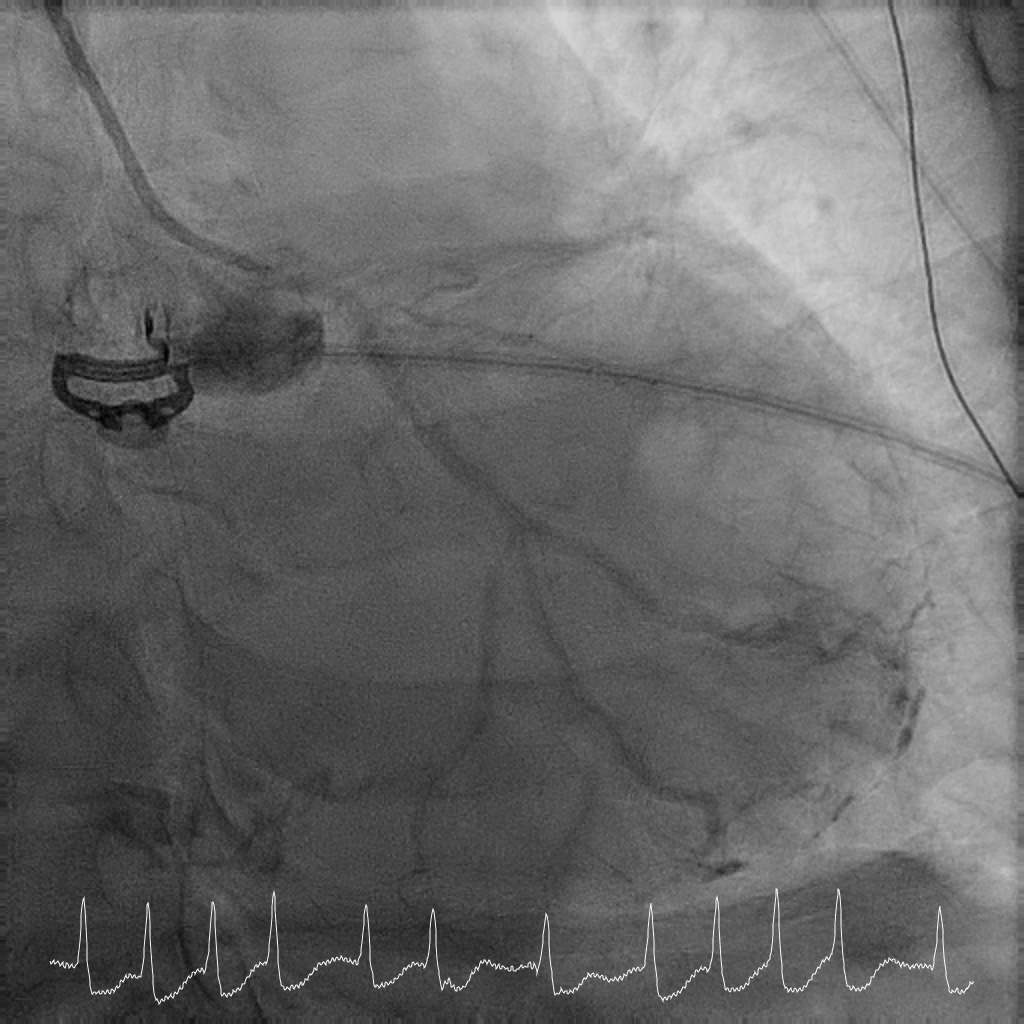
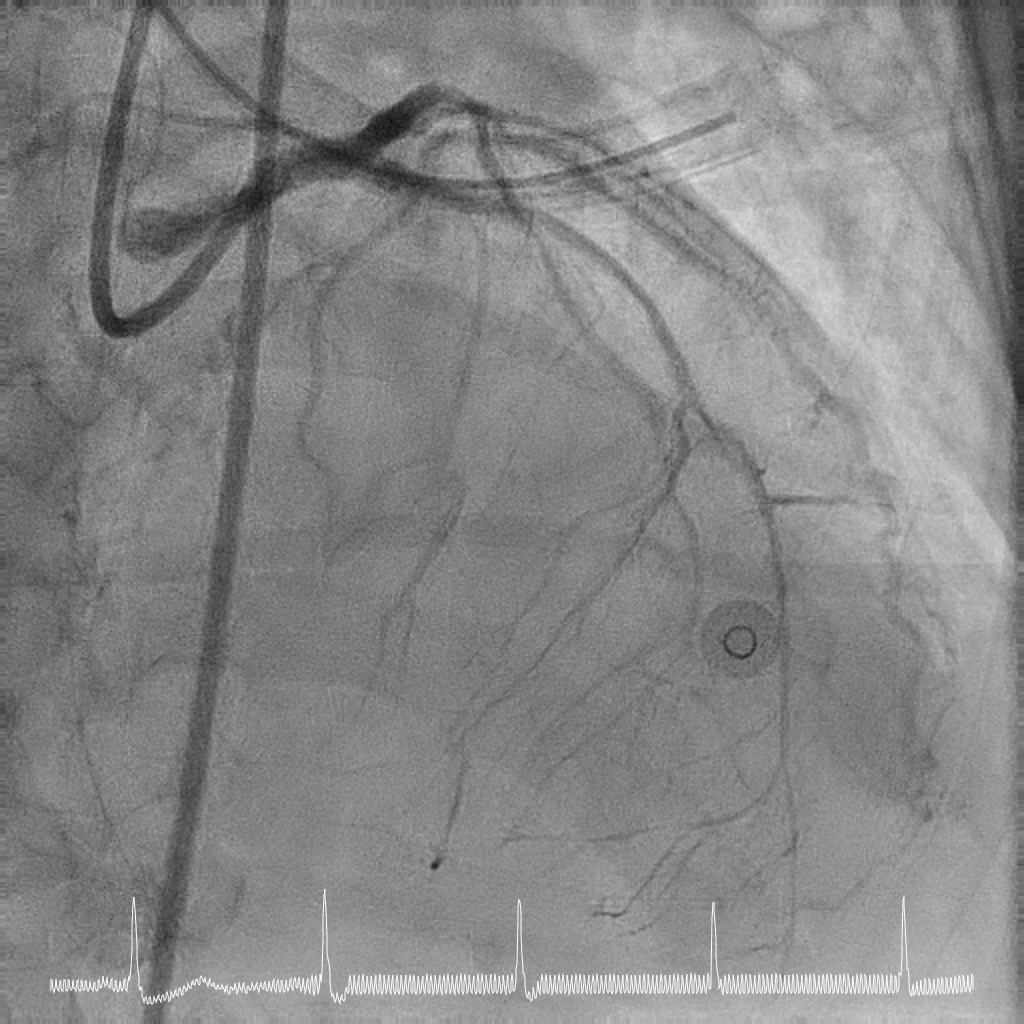
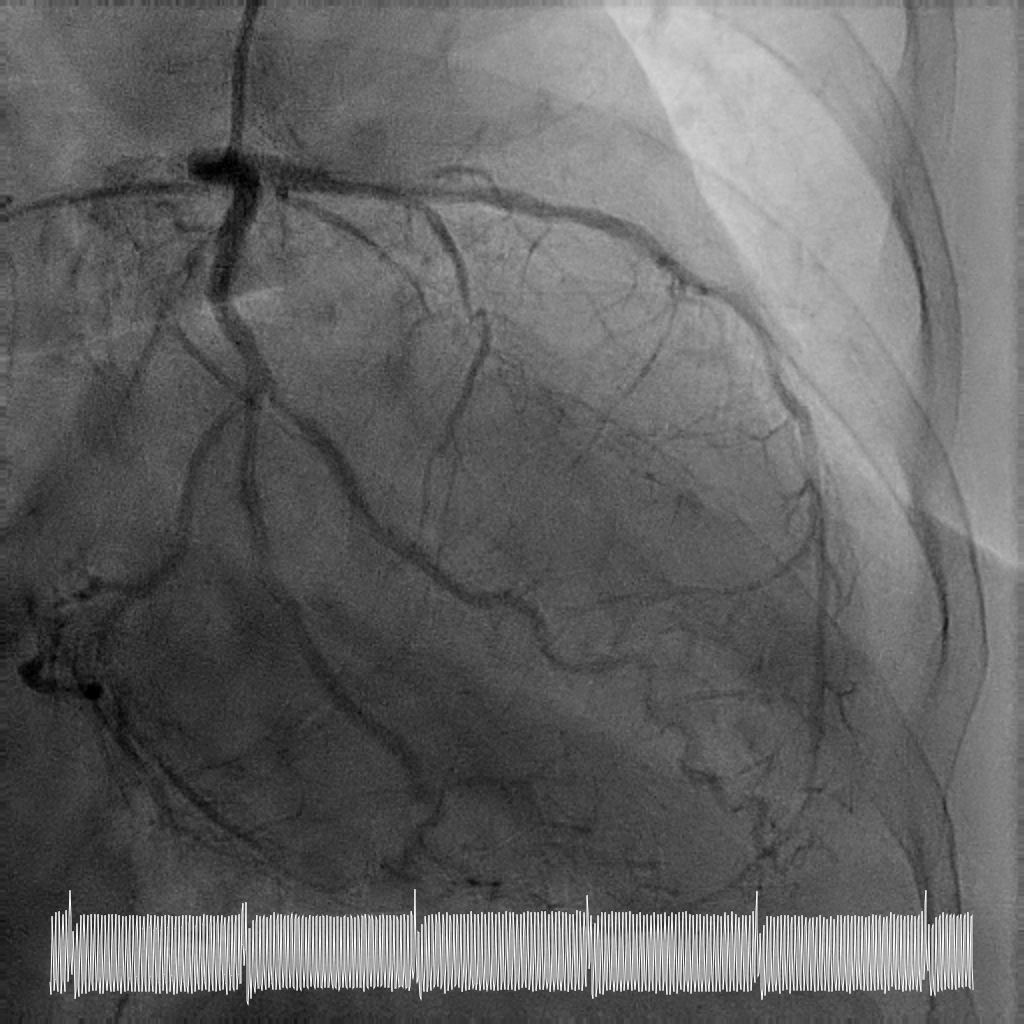
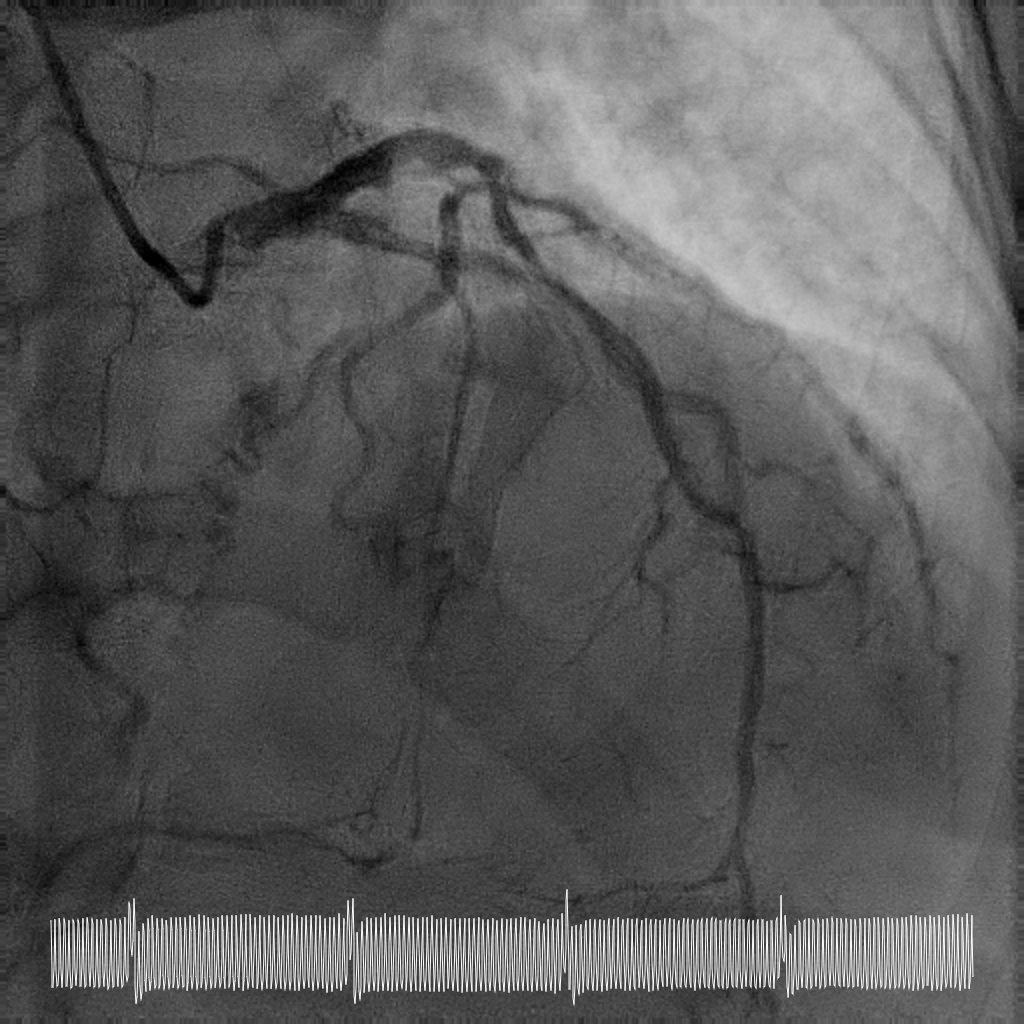
Coronary angiography showed critical calcified LM into both LAD and LCx. LAD was noted to be calcified and occluded at the ostium, with collaterals from LCx filling the distal LAD. RCA was a long segment CTO (occluded at the ostium) and showed retrograde filling from LCx collaterals. There was moderate proximal disease of the LCx. Cardiac surgery was consulted for consideration of urgent CABG, but surgical risk was prohibitive. After discussion with family, decision was for high-risk complex PCI.

Interventional Management
Procedural Step
Rotational atherectomy with 1.5mm and then 2mm was performedfrom ostial LM to proximal LCx. Wiring of the LAD was only successful till midLAD with a separate distal LAD occlusion. LAD lesion was balloon uncrossableand half-way rotational atherectomy with 1.5mm burr. The distal LAD CTO wasthen crossed and balloon angioplasty undertaken.
Case Summary
This case illustrates the feasibility of a hybridrevascularisation strategy combining two-burr rotational atherectomy, left mainbifurcation stenting with DK crush, and downstream drug-coated balloonangioplasty in a patient with prohibitive surgical risk. Careful lesionpreparation and strategic device selection resulted in sustained long-termvessel patency and recovery of ventricular function in a patient with extreme-riskanatomy.