Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251112_009
Balancing Safety and Success: Ultra-Low-Contrast PCI for LAD CTO in Advanced CKD
By Vimean Sey, Doni Firman
Presenter
Vimean Sey
Authors
Vimean Sey1, Doni Firman2
Affiliation
Cambodia China Friendship Preah Kossamak Hospital, Cambodia1, National Cardiovascular Center Harapan Kita, Indonesia2
View Study Report
CASE20251112_009
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Balancing Safety and Success: Ultra-Low-Contrast PCI for LAD CTO in Advanced CKD
Vimean Sey1, Doni Firman2
Cambodia China Friendship Preah Kossamak Hospital, Cambodia1, National Cardiovascular Center Harapan Kita, Indonesia2
Clinical Information
Relevant Clinical History and Physical Exam
A 75-year-old woman with history of hypertension, type 2 diabetes, and CKD stage IV presented with exertional angina CCS class III despite receiving optimal medical therapy, resulting in repeated hospitalizations. Six months earlier, she experienced a late-onset myocardial infarction, which was managed with optimal medical therapy due to significantly low eGFR.
Relevant Test Results Prior to Catheterization
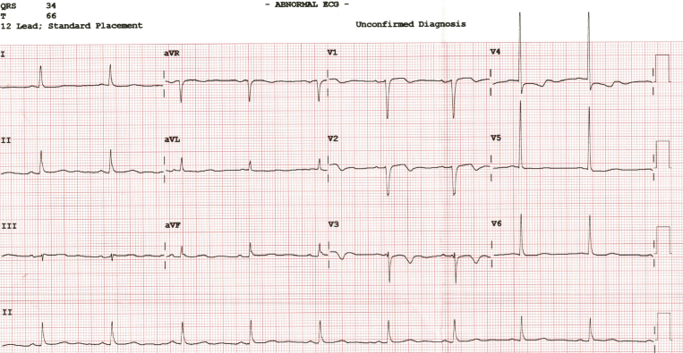
Investigations revealed sinus rhythm with poor R-wave progression and T-wave inversion in leads V1–V4 on ECG. Echocardiography demonstrated a left ventricular ejection fraction of 35–40% with hypokinesia of the anterior and antero-septal walls. Laboratory studies showed hemoglobin of 11.2 g/dL, platelet count of 270 ×10⁹/L, and an eGFR of 20 ml/min/1.73m².
Relevant Catheterization Findings
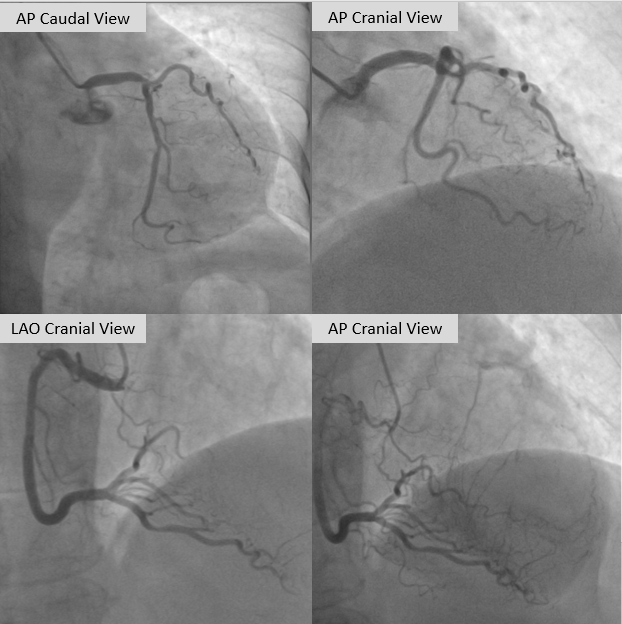
Coronary angiography demonstrated a normal left main artery. The left anterior descending (LAD) artery was totally occluded from the ostium, with distal segments receiving collateral supply from the contralateral circulation, Rentrop grade III. The left circumflex (LCX) artery showed a moderate lesion in its distal portion, while the right coronary artery (RCA), a dominant vessel, has moderate lesion from the proximal to mid segments. PCI for the LAD CTO was stagged within the next two weeks.
 Media1.mp4
Media1.mp4
Media2.mp4
Media4.mp4
Interventional Management
Procedural Step
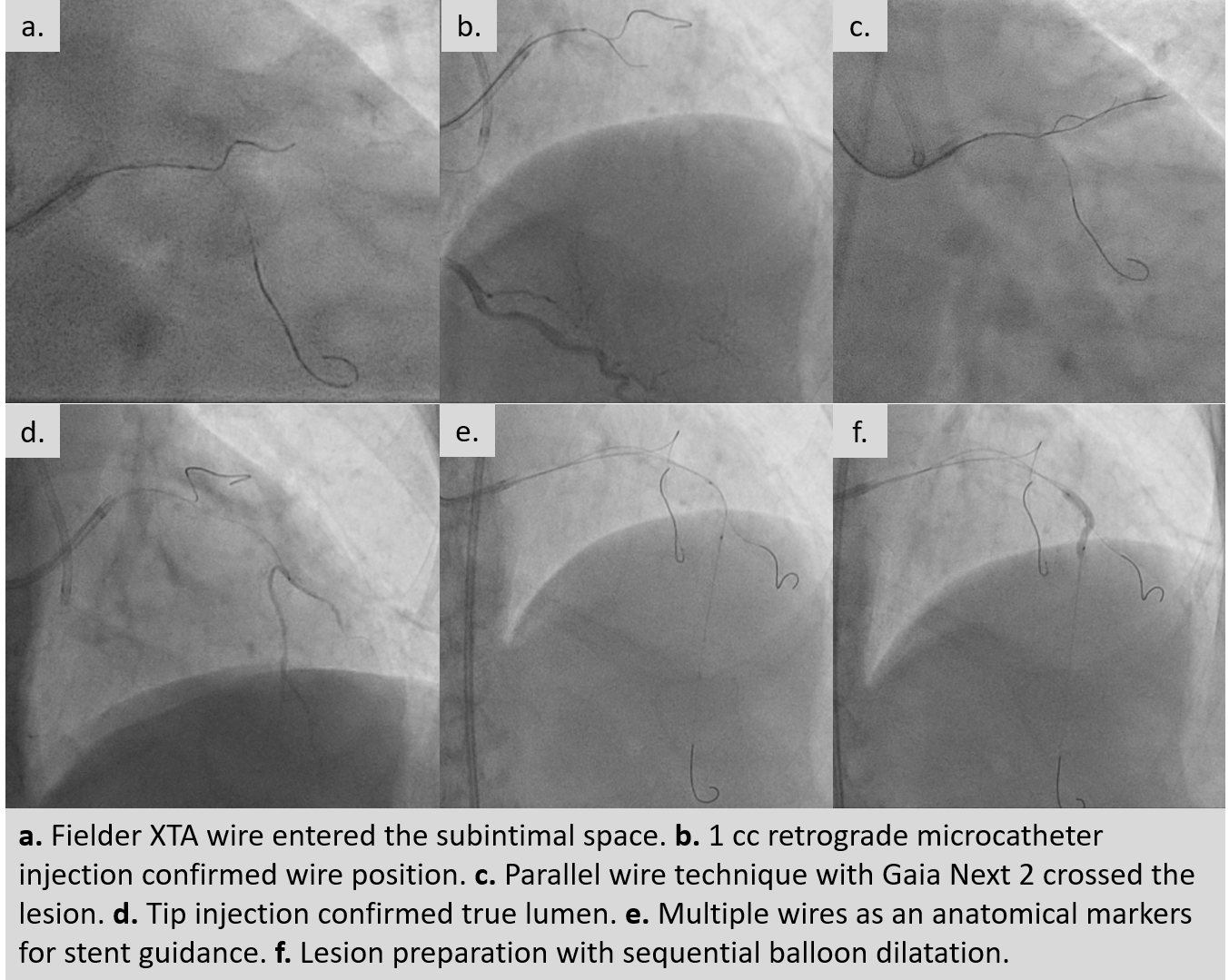
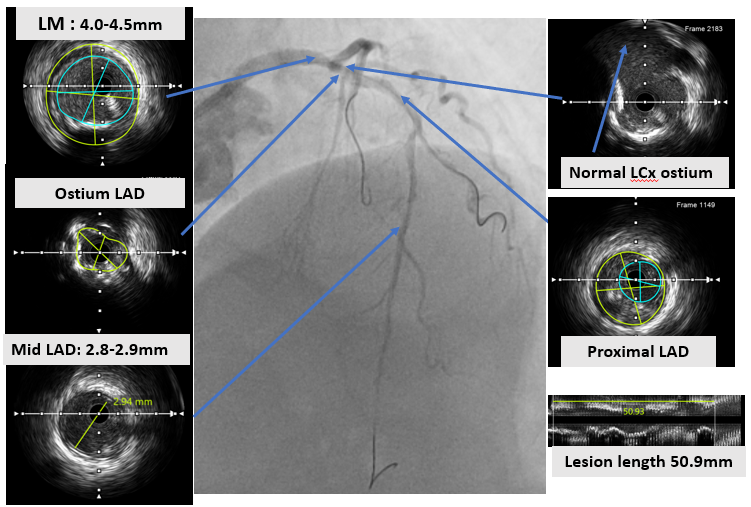
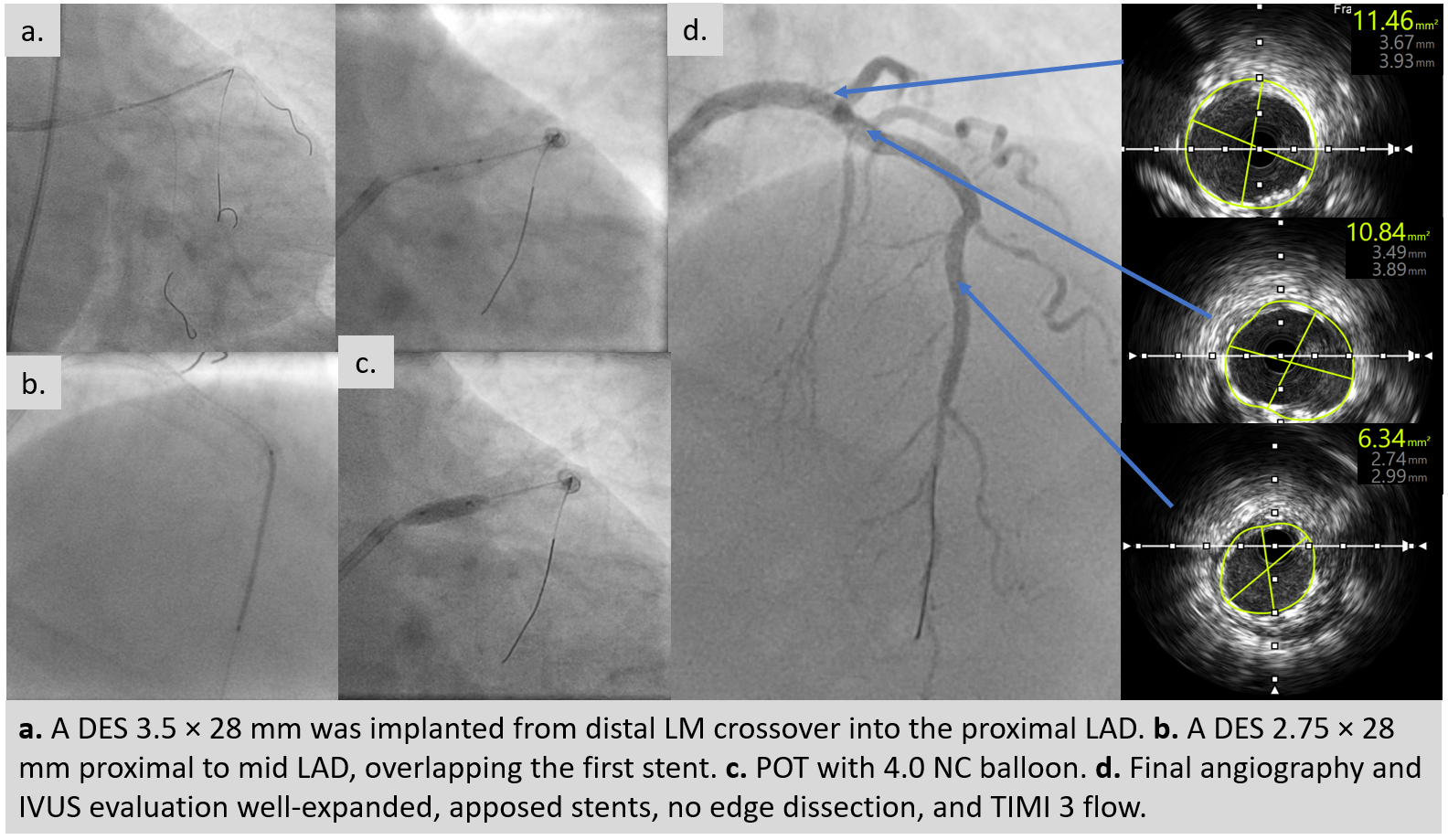
An ultra low contrast PCI of the LAD was performed using dual puncture with EBU 3.5/7F and JR 3.5/6F catheters via radial and femoral access. Saline was used for engagement, with contrast restricted to microcatheter injections of 1 cc each as a sparing strategy. Antegrade proximal cap puncture with Finecross and Fielder XTA tracked subintimally, and a parallel wire technique with Gaia Next 2 successfully crossed the lesion, confirmed by retrograde injection. Lesion preparation was achieved with a semicompliant balloon (2.5 × 15 mm) from mid to proximal LAD and a cutting balloon (2.75 × 18 mm) from mid to ostium LAD. IVUS pullback revealed a long diffuse lesion with proximal and ostial calcification, showing calcium cracks after preparation. MLA at the ostium LAD was 2.5 mm², distal reference diameter 2.8 mm, and LM diameter 4.5 mm. Stent deployment was guided by multiple wires as anatomical landmarks without contrast. A DES (3.5 × 28 mm) was implanted from distal LM crossover to proximal LAD, followed by POT with a 4.0 × 9 mm NC balloon. A second DES (2.75 × 28 mm) was placed in proximal to mid LAD overlapping the first, with post-dilation using a 3.0 × 15 mm NC balloon. IVUS confirmed well-expanded, well-apposed stents without edge dissection. Final MSA was 12 mm² in LM, 10.8 mm² in ostium LAD, and 6.3 mm² in mid LAD. Final angiography with diluted contrast demonstrated TIMI 3 flow, with total contrast use limited to 12 cc.
Case Summary
Ultra low contrast PCI guided by IVUS is feasible and safe in patients with advanced CKD and complex LAD CTO. Careful wire strategies, contrast-sparing techniques, and intravascular imaging allow precise stent deployment while minimizing risk of kidney injury. This case highlights that with meticulous planning and imaging guidance, complete revascularization can be achieved using only 12 cc of contrast, preserving kidney function and ensuring optimal coronary outcomes.