Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251112_008
Complex Left Main Bifurcation CTO PCI Using Dual Access and Intravascular Imaging in a Surgical Turn-Down Patient
By Muhammad Farid Mohd Fauad, Afifah Suhailah Suhailah Awang Soh, Dhani Darshan Francis
Presenter
Muhammad Farid Mohd Fauad
Authors
Muhammad Farid Mohd Fauad1, Afifah Suhailah Suhailah Awang Soh1, Dhani Darshan Francis1
Affiliation
Hospital Tengku Ampuan Afzan, Kuantan, Malaysia1
View Study Report
CASE20251112_008
Coronary - Complex PCI - CTO
Complex Left Main Bifurcation CTO PCI Using Dual Access and Intravascular Imaging in a Surgical Turn-Down Patient
Muhammad Farid Mohd Fauad1, Afifah Suhailah Suhailah Awang Soh1, Dhani Darshan Francis1
Hospital Tengku Ampuan Afzan, Kuantan, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
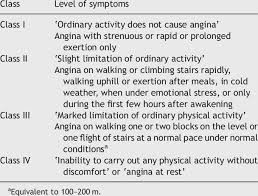
A 73-year-old man, ex-smoker, with hypertension, dyslipidemia, and ischemic heart disease was electively admitted for staged percutaneous coronary intervention (PCI) to a chronic total occlusion (CTO) of the left anterior descending artery (LAD). The patient refused coronary artery bypass grafting (CABG). He reported occasional angina, Canadian Cardiovascular Society (CCS) Class II. Physical examination was unremarkable with blood pressure 145/65 mmHg and pulse rate 67 bpm.
Relevant Test Results Prior to Catheterization
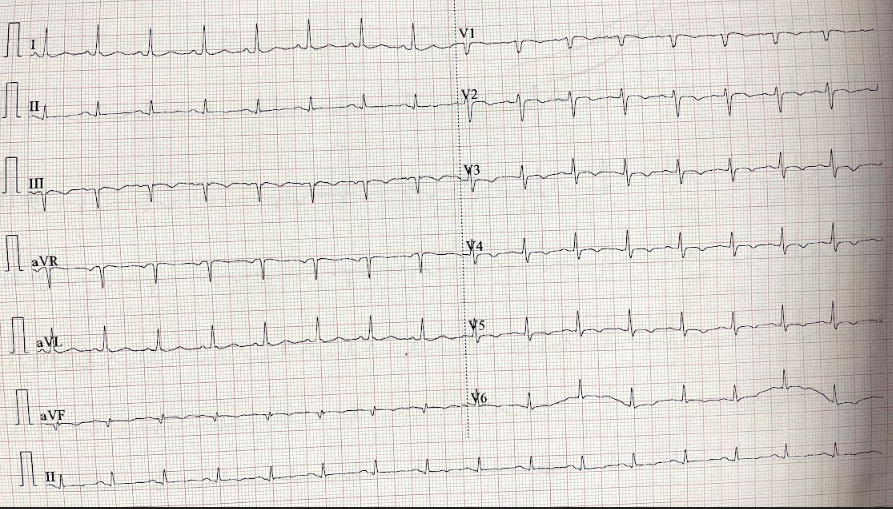
Hemoglobin 13 g/dL, urea 6.7 mmol/L, and creatinine 114 µmol/L. Electrocardiogram showed sinus rhythm, and chest radiograph revealed clear lung fields.
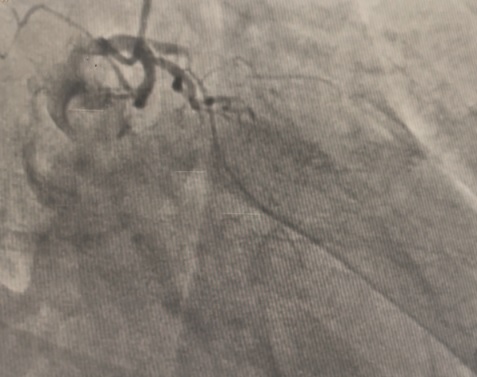
Relevant Catheterization Findings
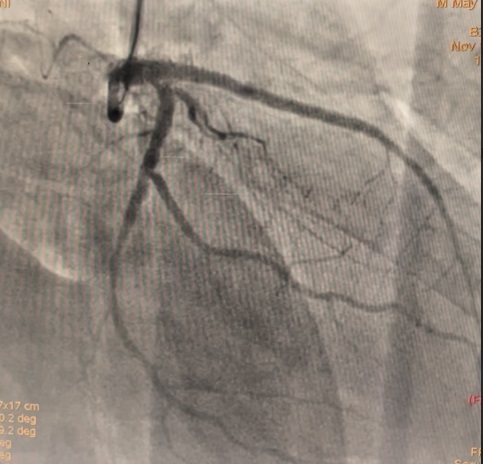
The LM had 50% ostial stenosis. LAD showed proximal CTO with bridging collaterals from the right coronary artery. LCx demonstrated proximal CTO with contralateral collaterals from the RCA. The right coronary artery was dominant with mild disease. The case represented complex dual CTO with LM involvement, posing both technical and procedural challenges due to tortuosity and calcification.
 RAO Caudal COROS video.mov
RAO Caudal COROS video.mov
RAO Cranial video COROS.mov
LAO caudal Coros Video.mov
Interventional Management
Procedural Step
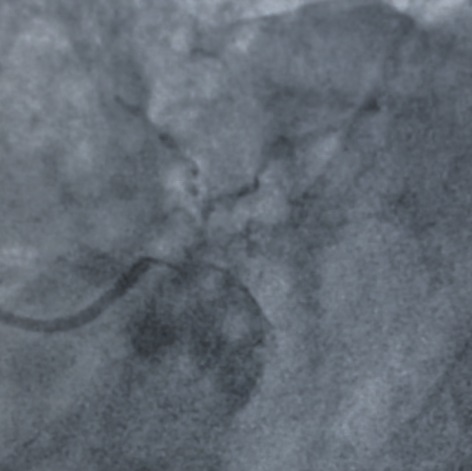
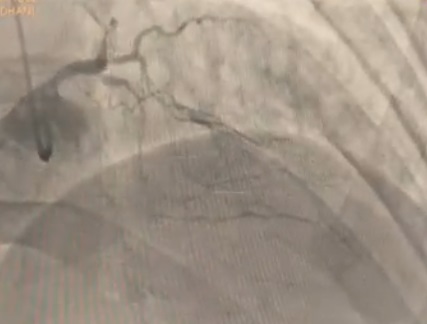
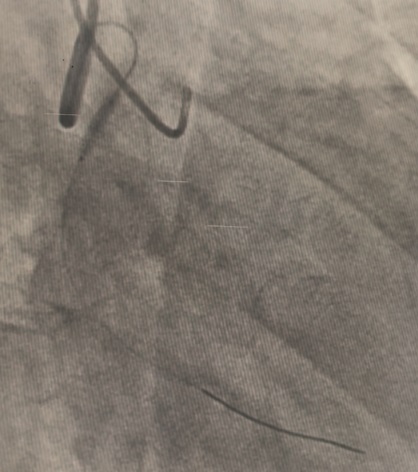
A dual access strategy was used: right radial for RCA and right femoral for LCA. For LCx CTO PCI, a Finecross microcatheter (Terumo, Japan) was advanced to the distal LCx. Predilation was done using a 2.5 × 15 mm Firefighter balloon (Medtronic, USA) at 8 atm, followed by stenting with a 3.5 × 30 mm Orsiro Mission drug-eluting stent (Biotronik, Germany) at 16 atm. Postdilation was performed with a 3.0 × 15 mm Accuforce non-compliant (NC) balloon (Terumo, Japan) at 14 atm.For LAD CTO PCI, Finecross with Fielder wire (Asahi, Japan) failed to cross; Gaia First (Asahi, Japan) successfully reached the distal LAD. Predilation was performed using NC Sapphire 24 (OrbusNeich, Hong Kong) 3.5 × 12 mm and Wedge NC (Boston Scientific, USA) 3.0 × 15 mm. A 3.0 × 40 mm Biofreedom Ultra stent (Biosensors, Singapore) was deployed at 14 atm. Proximal dissection into LM was noted, requiring LM–LAD stenting with 3.5 × 22 mm Orsiro Mission and proximal optimization technique (POT) using 4.5 × 18 mm NC Emerge balloon (Boston Scientific, USA). Intravascular ultrasound (IVUS) revealed ostial–proximal LCx disease, confirming a bifurcation lesion. Ostial LCx was predilated with a 3.5 × 12 mm NC Sapphire balloon and stented with a 3.5 × 14 mm Biofreedom Ultra. Final kissing balloon inflation was done with NC Sapphire 3.5 × 12 mm (LAD) and 3.5 × 14 mm (LCx), followed by final POT with NC Emerge 4.5 × 8 mm balloon at 18 atm. Final shot revealed TIMI 3 flow with no dissection or perforation.
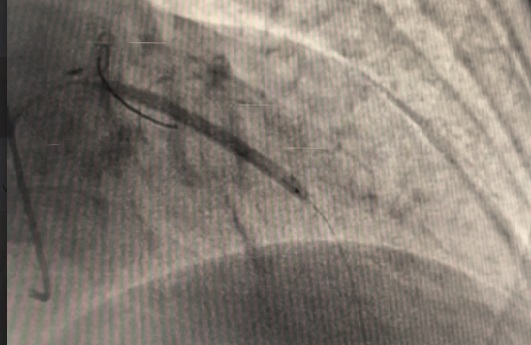
Stent lcx video.mov
Stent LAD video.mov
Final flow.mov
Case Summary
This complex case of dual CTO involving LM bifurcation was successfully treated using a dual access approach, multiple wire strategies, and IVUS-guided optimization. The procedure demonstrates that percutaneous revascularization can be a feasible alternative for surgical turn-down patients when performed with meticulous planning and imaging guidance. Optimal outcomes were achieved with POT and final kissing balloon techniques, restoring full coronary flow. This case highlights the evolving capability of complex PCI to address high-risk anatomy traditionally managed by CABG.