Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251112_001
Post CABG Left Main Occlusion With Posterolateral Infarction
By Thomas George
Presenter
Thomas George
Authors
Thomas George1
Affiliation
Caritas Heart Institute, India1
View Study Report
CASE20251112_001
Coronary - ACS/AMI
Post CABG Left Main Occlusion With Posterolateral Infarction
Thomas George1
Caritas Heart Institute, India1
Clinical Information
Relevant Clinical History and Physical Exam
72 year old man post-CABG LIMA->LAD, SVG->D1, PDA in 2008 and PCI->RCA and ramus 2019 presented with intermittent lower chest discomfort with multiple episodes of vomiting and fatigue. He had past history of left thalamic infarct in 2022 and right corona radiata infarct in 2024. He had diabetes, hypertension, and atrial fibrillation in a previous holter. On examination he was conscious, alert, BP 130/90, PR 112/min, regular, heart sounds normal, respiratory system examination normal.

 echo inferior wall mi.mp4
echo inferior wall mi.mp4
left main occlusion.mp4
rca.mp4
Relevant Test Results Prior to Catheterization
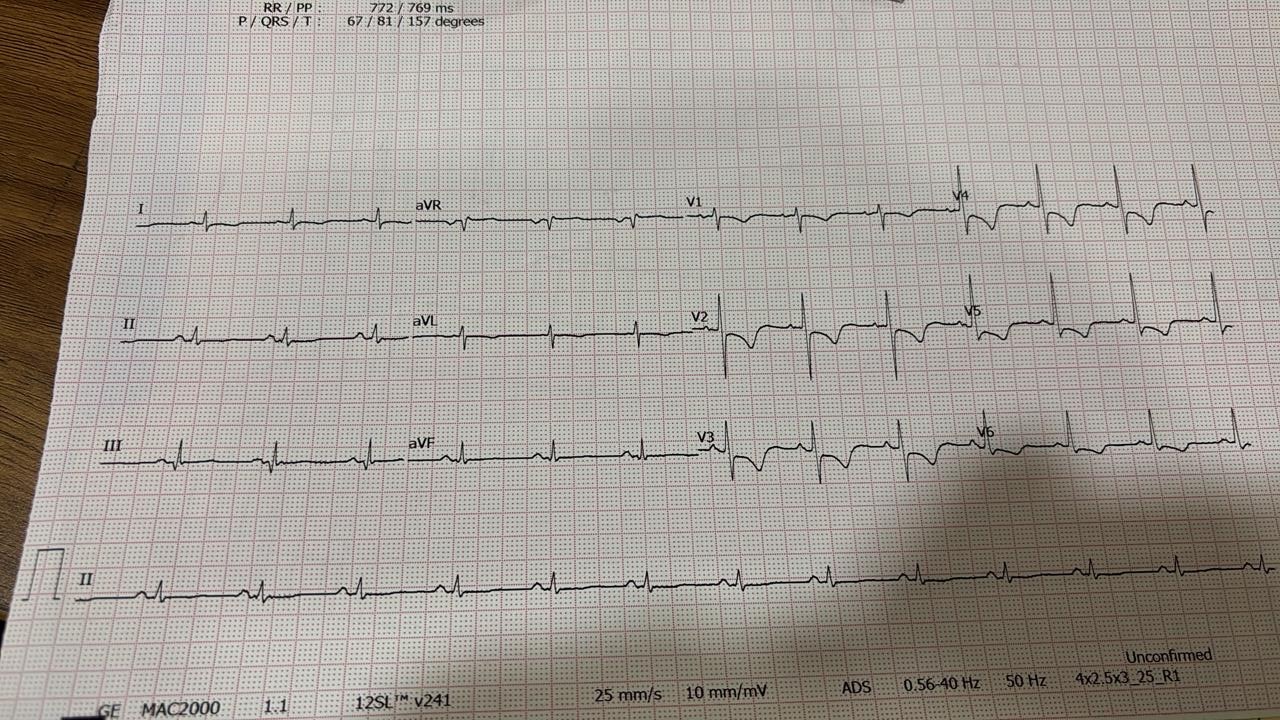
Hb - 12.7Na - 142K - 4Cr - 1.8TropI >10ECG showed sinus tachycardia, ST depression in L1, avL, V2-V6Echo - noted LV dysfunction, inferior posterolateral RWMA
echo inferior wall mi.mp4
Relevant Catheterization Findings
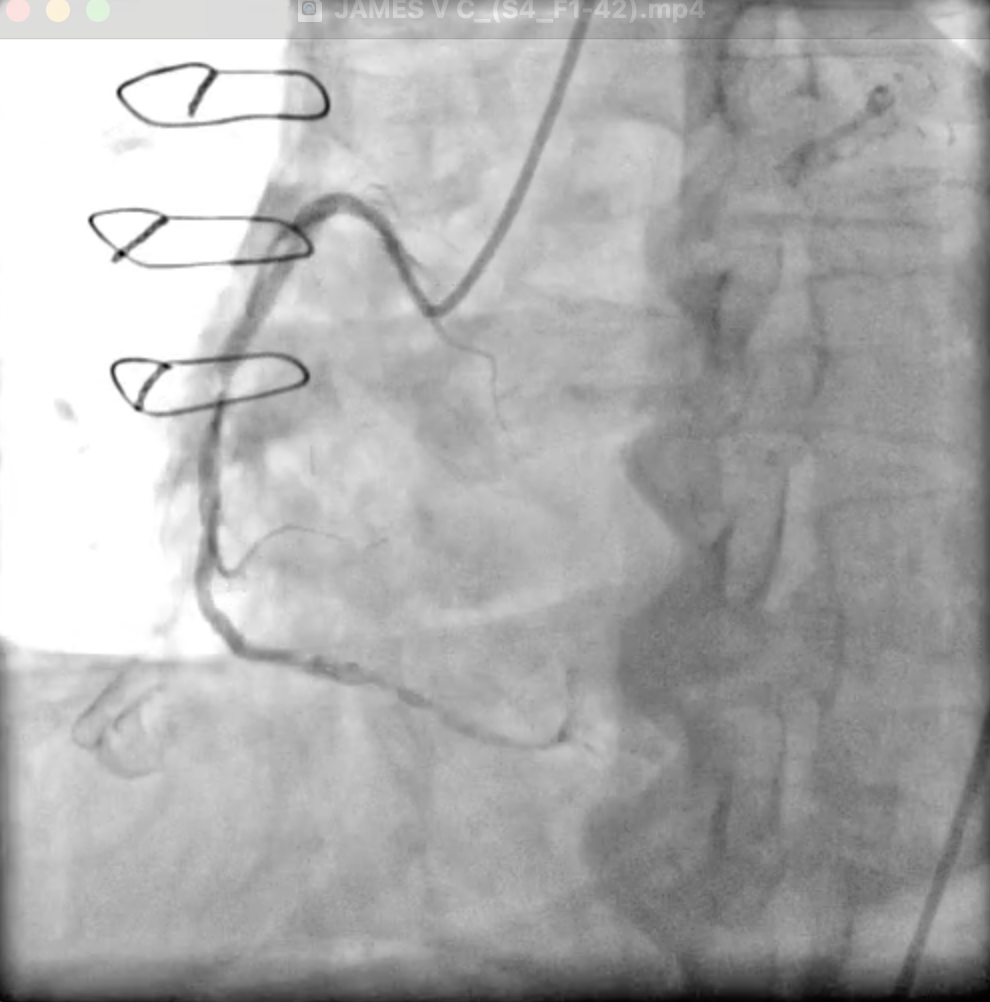
LMCA occluded from the ostium. LAD - ostioproximal occlusion. LCX - ostioproximal occlusion. RCA-dominant, stent with ISR 90%. LIMA to LAD patent, flows well. SVG to D1 and PDA diagonal occluded.
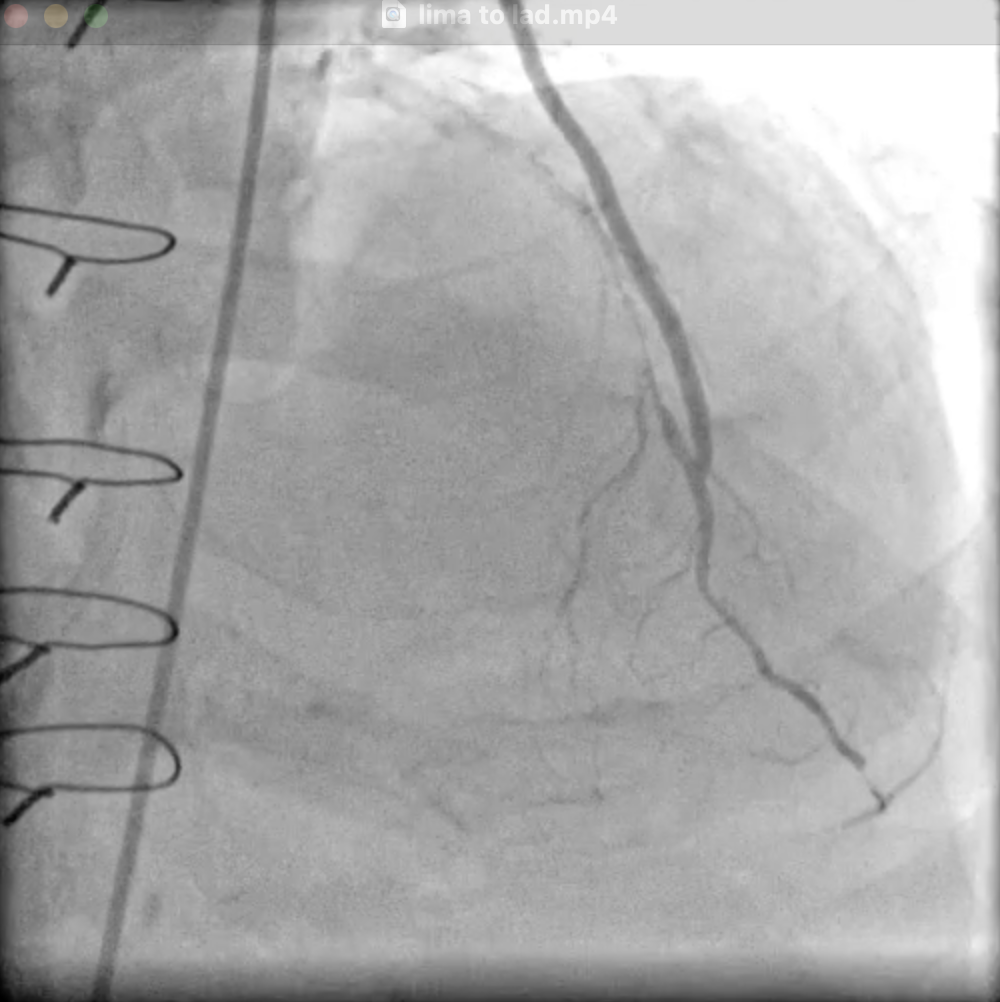
lima to lad.mp4
rca mid segment instant restenosis.mp4
post wiring lm to l6.mp4
Interventional Management
Procedural Step
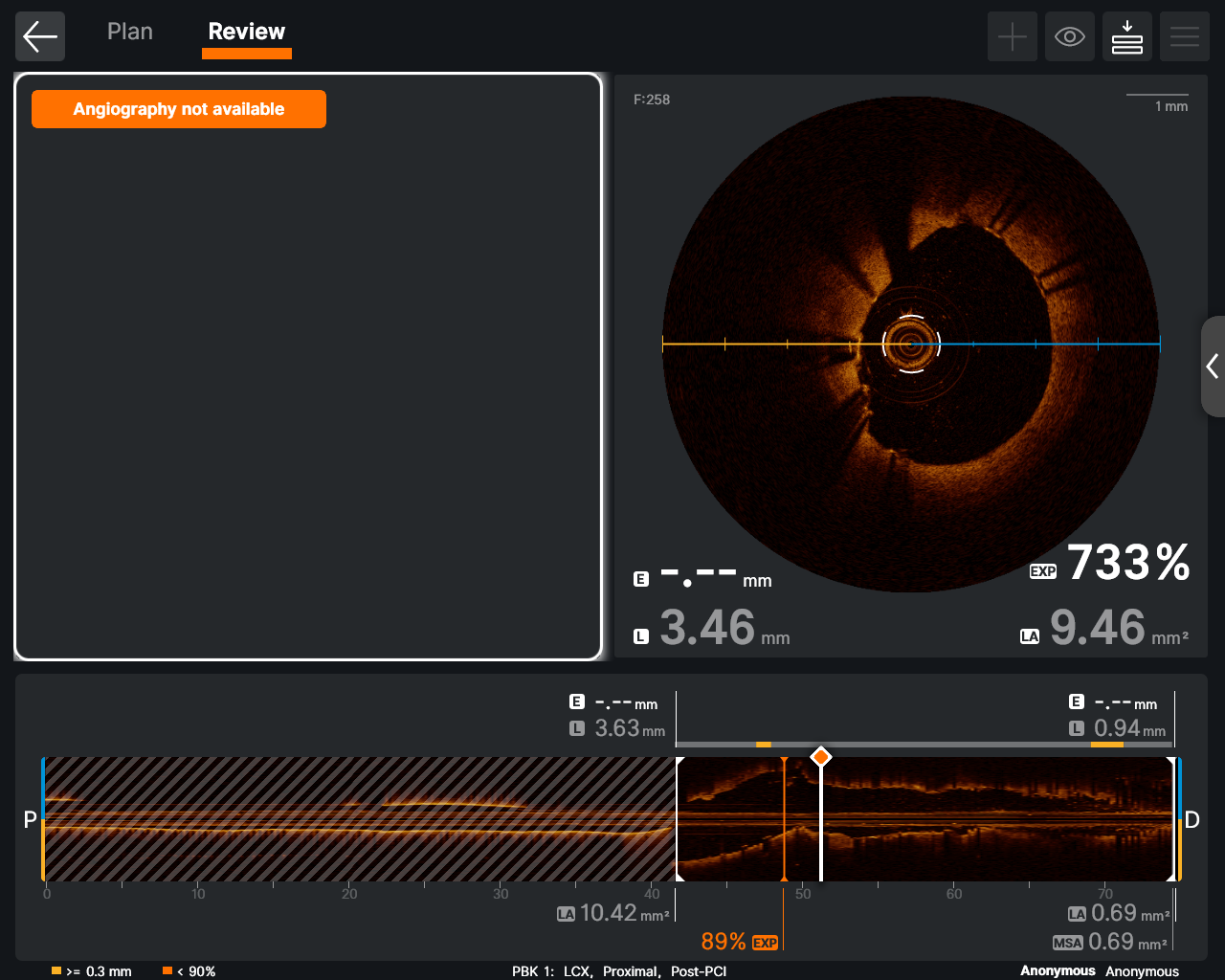
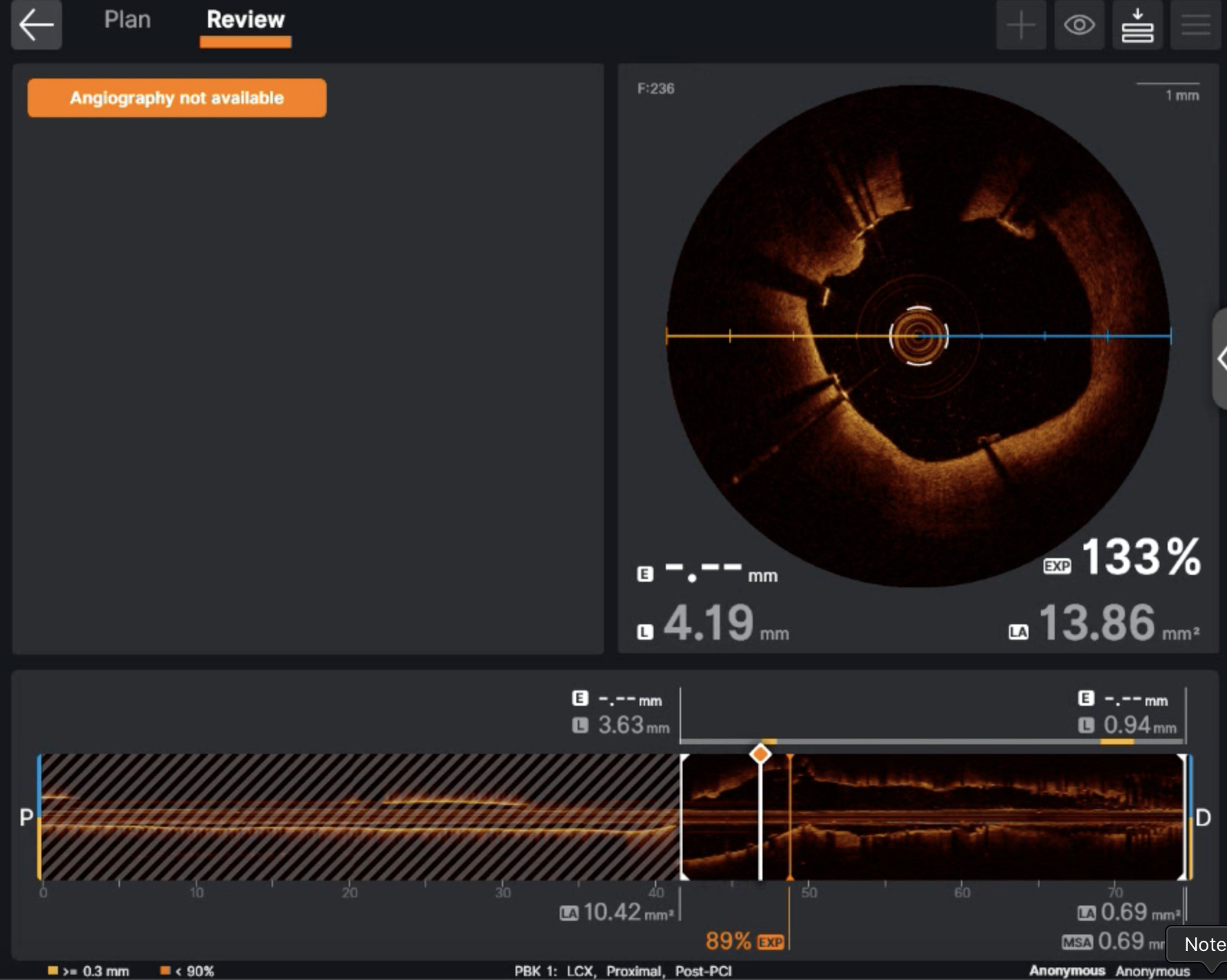
Right femoral access. 6Fr EBU 3.5 guide. LCX lesion crossed. Lesion in left main and LCX was crossed with Fielder FC wire and serially predilated with 2x15 and 2.5x15 NC balloons. Then we used cutting balloon 3x13 NSE Aperta balloon at 14-18atm. Mid LCX lesion was stented with 2.75x40 Ultimaster Nagomi and LM-LCX was stented with 3.5x23 Xience Xpedition at 14atm with an overlapping fashion with support of guide+. Stented segment was post-dilated with 3.5x12 NC balloon at 18-20atm and LM POT was done with 4.5x6 NC balloon at 18atm. Post OCT evaluation of LM-LCX was done which revealed stent well apposed with no distal dissection and no malapposition with an LCX MSA of 9.28mm and LM MSA of 11.92mm. Final result - TIMI 3 flow.

2.75x40 DES placed with guide support.mp4
lm to lcx implanted.mp4
result.mp4
Case Summary
This was a unique case of post cabg native left main occlusion presenting as inferolateral MI. LIMA to LAD was patent and other two grafts occluded. There was critical instant restenosis of RCA. We could successfully revascularize the left main to LCX. Adjuvant devices like cutting balloon and guide extension catheters helped achieve good results. We reduced the contrast during procedures in view of his CKD. Final OCT images showed well apposed stents with good MSA. Post CABG patients with occlusion of LCX can present with significant ongoing chest pain,heart failure ,subtle ECG changes and echo evidence of significant ischemia in inferior poslat segment. Being proactive improved outcome.