Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251111_003
Reversal of Diffuse Pulmonary Arteriovenous Malformations After Glenn: A Case Report
By Mengqi Zhao, Junxiang Pan, Xuechen Liu, Xinyu Cong, Zonghui Hou, Feiyang Wang, Yongqiang Jin, Lianyi Wang
Presenter
Mengqi Zhao
Authors
Mengqi Zhao1, Junxiang Pan2, Xuechen Liu1, Xinyu Cong1, Zonghui Hou1, Feiyang Wang1, Yongqiang Jin1, Lianyi Wang1
Affiliation
The First Hospital of Tsinghua University, School of Clinical Medicine, Tsinghua University, China1, The First Hospital of Tsinghua University, China2
View Study Report
CASE20251111_003
Structural - Surgical Therapy (Structural)
Reversal of Diffuse Pulmonary Arteriovenous Malformations After Glenn: A Case Report
Mengqi Zhao1, Junxiang Pan2, Xuechen Liu1, Xinyu Cong1, Zonghui Hou1, Feiyang Wang1, Yongqiang Jin1, Lianyi Wang1
The First Hospital of Tsinghua University, School of Clinical Medicine, Tsinghua University, China1, The First Hospital of Tsinghua University, China2
Clinical Information
Relevant Clinical History and Physical Exam
A male infant was diagnosed at 42 days with complex congenital heart disease, including double outlet right ventricle, large ventricular septal defect, atrial septal defect, and pulmonary stenosis. At 6 months, he underwent a bidirectional Glenn procedure with main pulmonary artery ligation, improving SpO₂ from 85 % to 90 %. Six months later, progressive cyanosis and poor growth developed. At age five, he showed severe cyanosis, digital clubbing, and SpO₂ of 58–69 %.
Relevant Test Results Prior to Catheterization
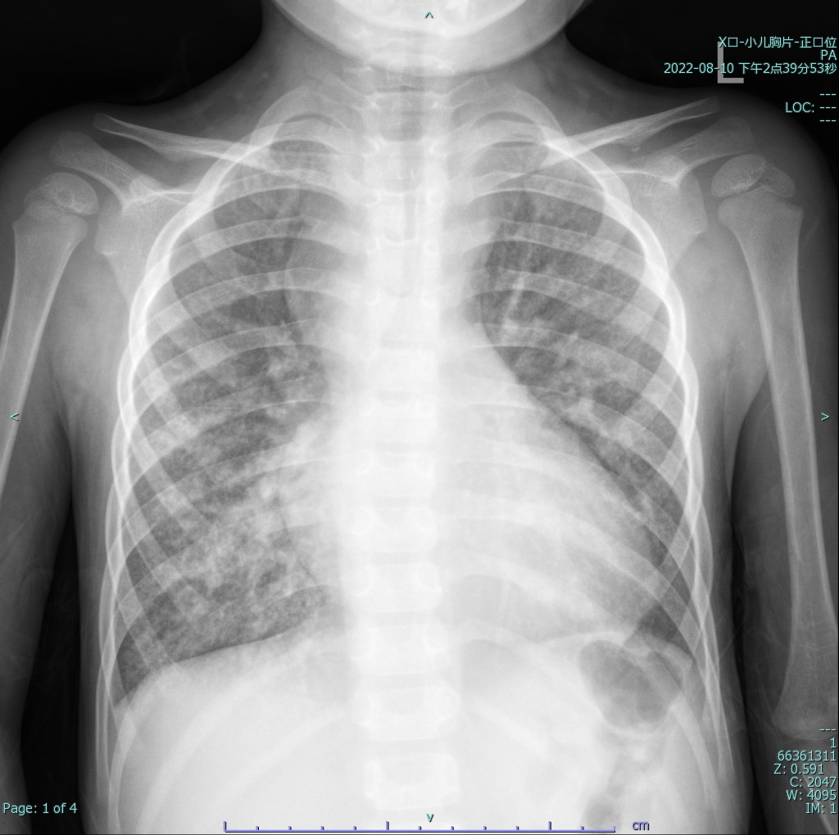
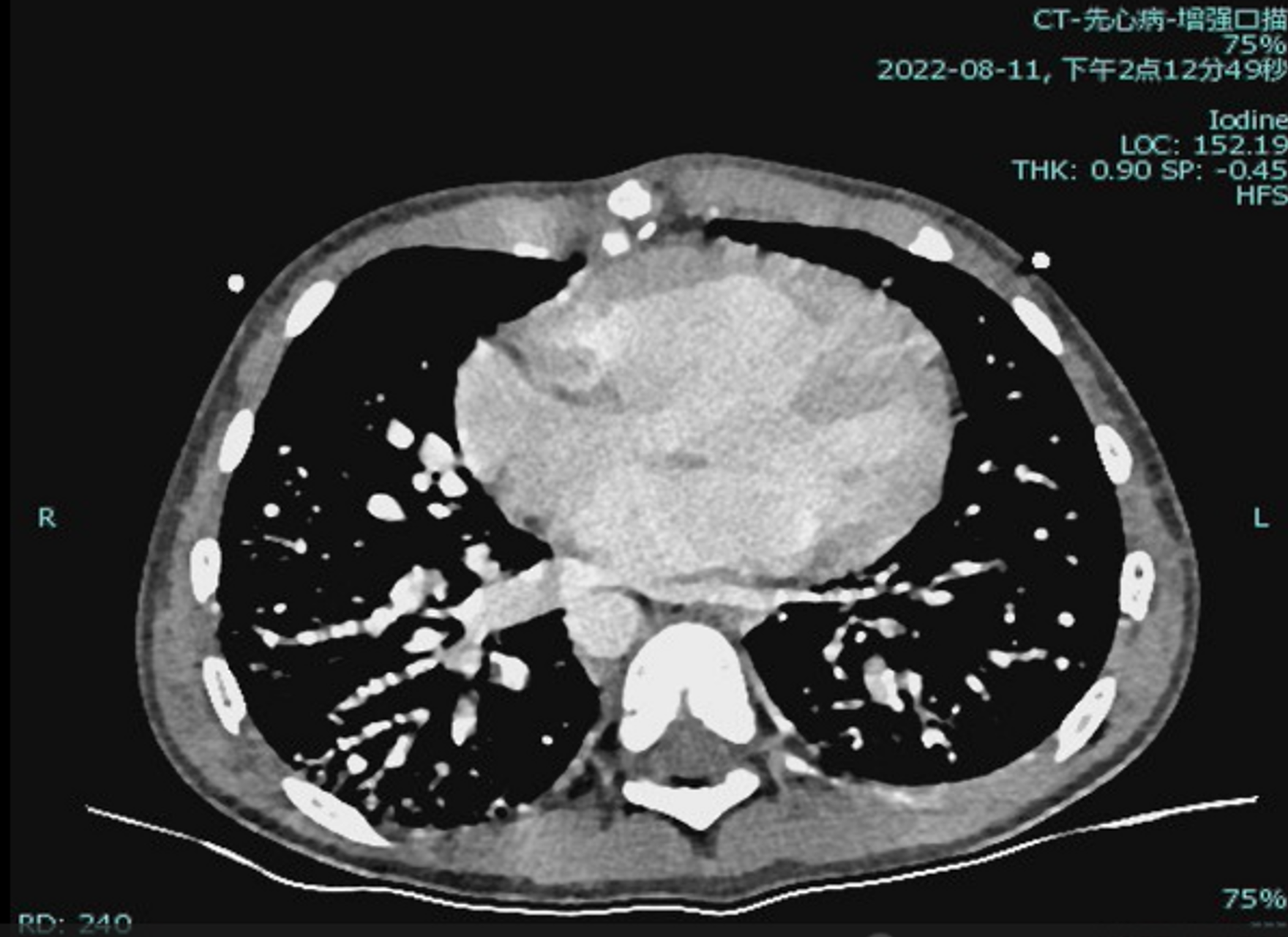
Laboratory testing showed hemoglobin 225 g/L and hematocrit 73.3%. Arterial blood gas revealed PO₂ 30.7 mmHg and SO₂ 58.1%. Chest X-ray showed cardiomegaly (cardiothoracic ratio 0.6) and increased pulmonary markings. Echocardiography demonstrated a patent Glenn anastomosis. Contrast-enhanced CT revealed absence of the main pulmonary artery and diffuse pulmonary arteriovenous malformations (PAVMs) in both lungs, most prominent in the lower lobes.
Relevant Catheterization Findings
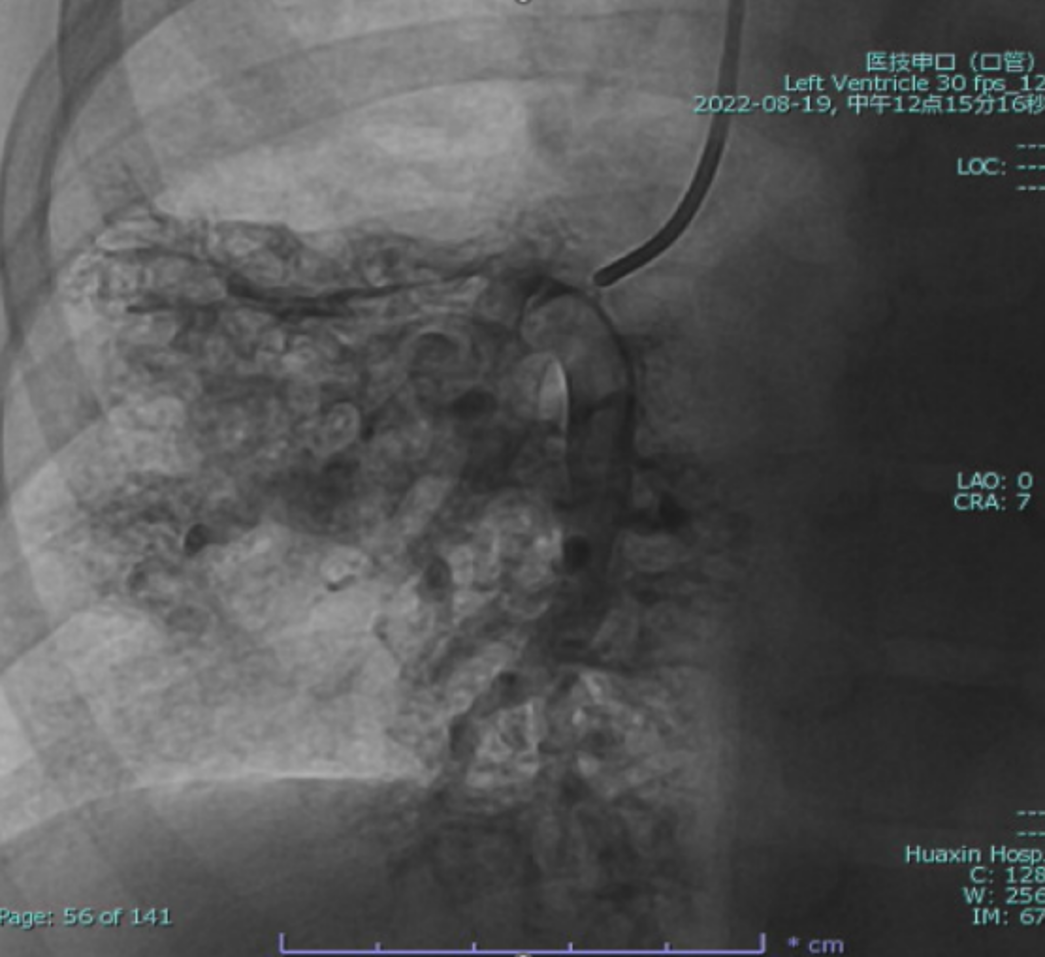
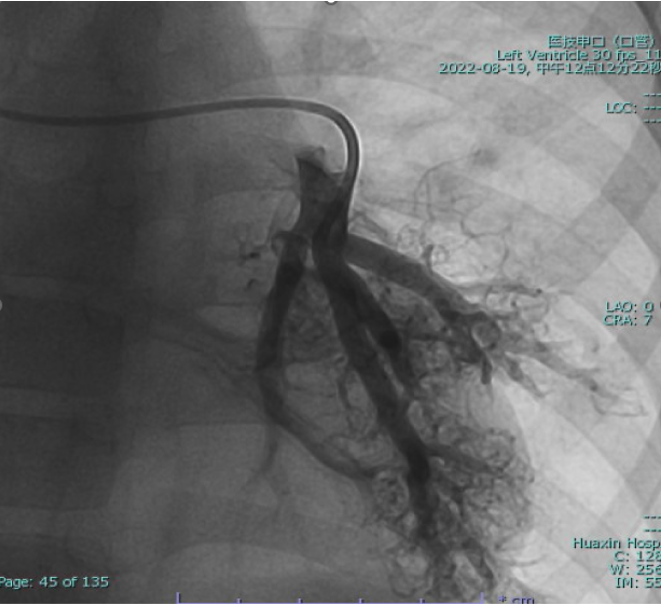
Cardiac catheterization confirmed absence of antegrade pulmonary flow with well-developed bilateral pulmonary arteries. Distal pulmonary arteries and pulmonary venous branches were markedly dilated, some showing a granular or “string-of-beads” appearance. Pulmonary circulation time was shortened, indicating significant right-to-left intrapulmonary shunting consistent with diffuse PAVMs. Pulmonary artery pressure was 17/9/13 mmHg.

Interventional Management
Procedural Step
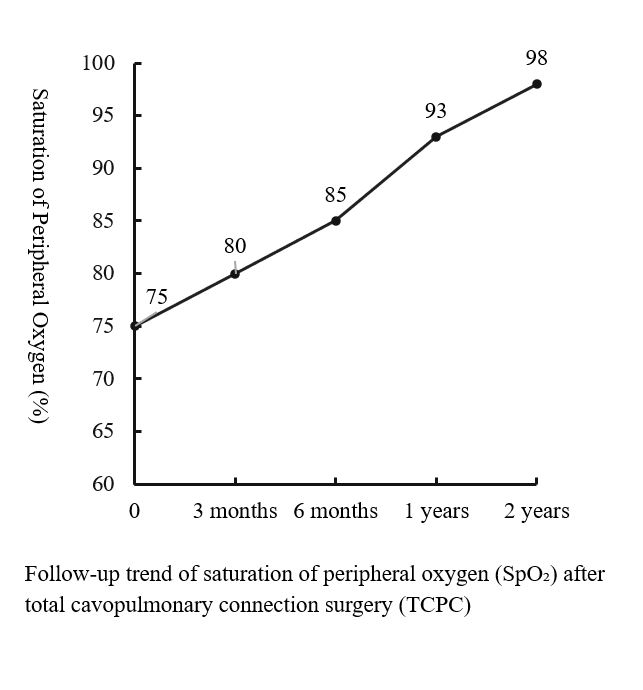
The operation was performed via a median sternotomy. Intraoperative exploration revealed that the ventricular septal defect was located in the inflow tract, distant from the aortic valve, making intracardiac tunnel construction infeasible; therefore, biventricular repair was not feasible. Under general anesthesia with hypothermic cardiopulmonary bypass, a total cavopulmonary connection (TCPC) was performed. The inferior vena cava was transected, and an 18-mm Gore-Tex conduit was anastomosed end-to-side to the right pulmonary artery, establishing a complete cavopulmonary circuit. Immediate postoperative oxygen saturation was approximately 75%. The total operative time was 6 hours and 14 minutes, with an aortic cross-clamp time of 50 minutes. The patient remained in the intensive care unit for 8 days and was discharged on postoperative day 19 after an uneventful recovery and stable hemodynamics. During a 2-year follow-up, peripheral oxygen saturation gradually increased and stabilized at 97–100%, with markedly improved exercise tolerance, resolution of digital clubbing, and normal skin color. Repeat cardiac catheterization confirmed unobstructed conduit flow and well-developed pulmonary vasculature. The previously extensive bilateral pulmonary arteriovenous malformations had completely resolved, pulmonary circulation time normalized, and pulmonary artery pressures measured 13/11/12 mmHg.

Case Summary
Diffuse PAVMs are a rare but serious complication after the Glenn procedure. This case shows that the loss of hepatic venous return contributes to their development, while restoring hepatic flow to the pulmonary circulation through TCPC can reverse PAVMs and normalize oxygenation. Cardiac catheterization plays a pivotal role in diagnosis, hemodynamic evaluation, and management planning. Early interventional assessment and timely completion of TCPC are crucial to improving outcomes in patients with unexplained hypoxemia after Glenn palliation.