Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251111_001
A Case of LAD CTO With Full Moon-Like Heavy Calcified Plaque
By Tomohiro Yamasaki, Atsunori Okamura, Kota Tanaka, Kiwamu Sudo, Mutsumi Iwamoto, Satoshi Watanabe, Yuta Nishimura, Yoshitomo Tsutsui, Heitaro Watanabe
Presenter
Tomohiro Yamasaki
Authors
Tomohiro Yamasaki1, Atsunori Okamura1, Kota Tanaka1, Kiwamu Sudo1, Mutsumi Iwamoto1, Satoshi Watanabe1, Yuta Nishimura1, Yoshitomo Tsutsui1, Heitaro Watanabe1
Affiliation
Sakurabashi Watanabe Advanced Healthcare Hospital, Japan1
View Study Report
CASE20251111_001
Coronary - Complex PCI - CTO
A Case of LAD CTO With Full Moon-Like Heavy Calcified Plaque
Tomohiro Yamasaki1, Atsunori Okamura1, Kota Tanaka1, Kiwamu Sudo1, Mutsumi Iwamoto1, Satoshi Watanabe1, Yuta Nishimura1, Yoshitomo Tsutsui1, Heitaro Watanabe1
Sakurabashi Watanabe Advanced Healthcare Hospital, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
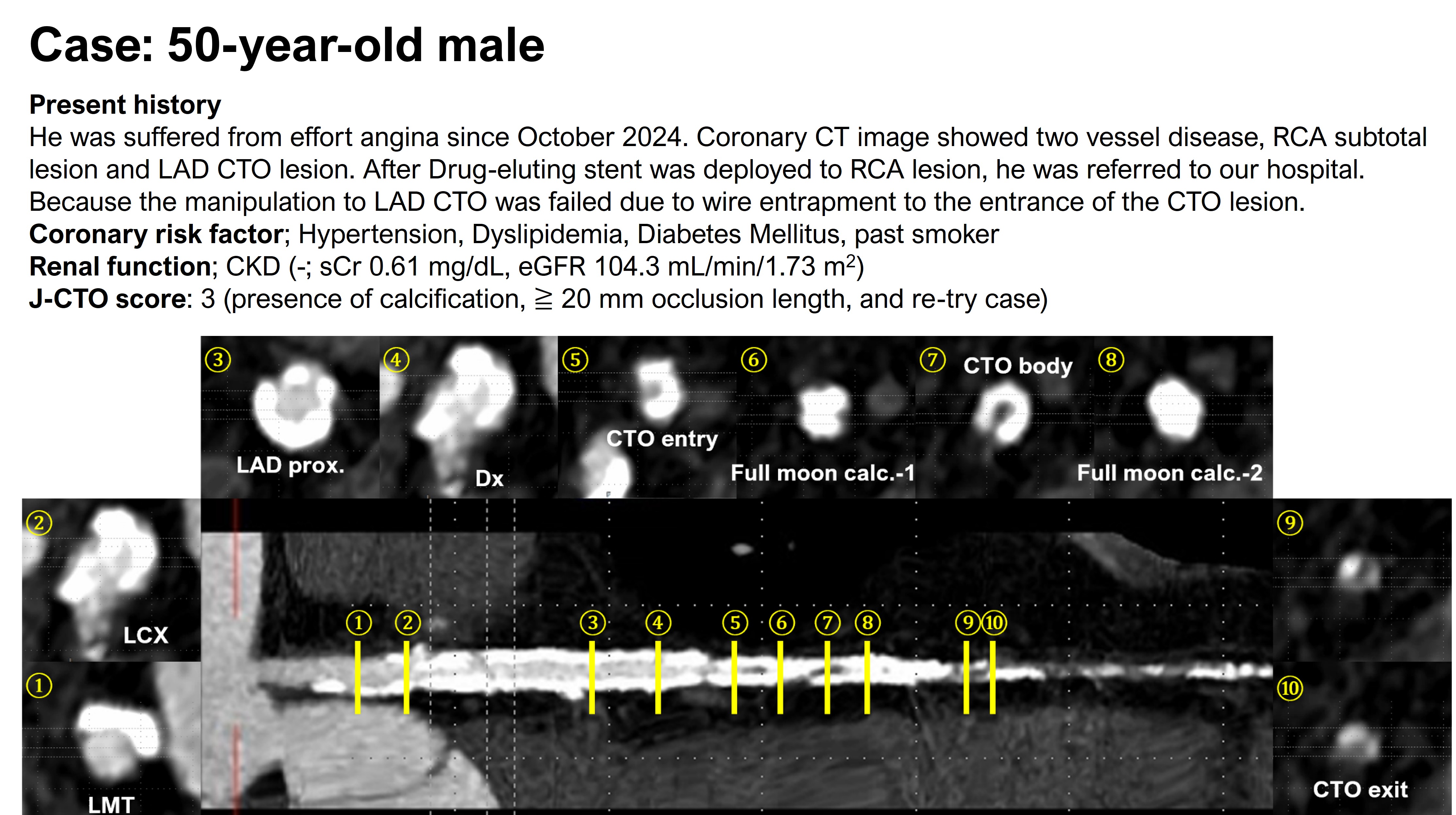
A 57-year-old man with long-standing diabetes had exertional angina and two-vessel calcified disease on CT. CABG was avoided due to high graft occlusion risk, and staged PCI was chosen. After successful RCA PCI, LAD CTO PCI using Gaia and Conquest Pro 8-20 failed; the wire fractured and was retrieved with two guidewires. He was then referred to our hospital for LAD CTO PCI.
Relevant Test Results Prior to Catheterization
The exercise stress test was positive, and cardiac MRI revealed delayed contrast enhancement in the LAD territory.
Relevant Catheterization Findings
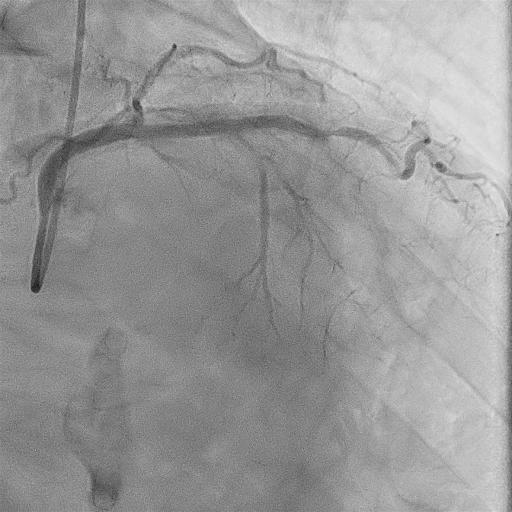
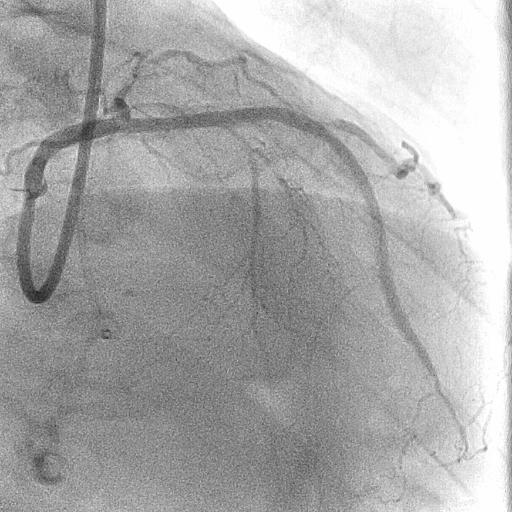
The left coronary artery had a severely calcified CTO from LAD segment 7, with no interventional collaterals, including from the right coronary artery.
Interventional Management
Procedural Step
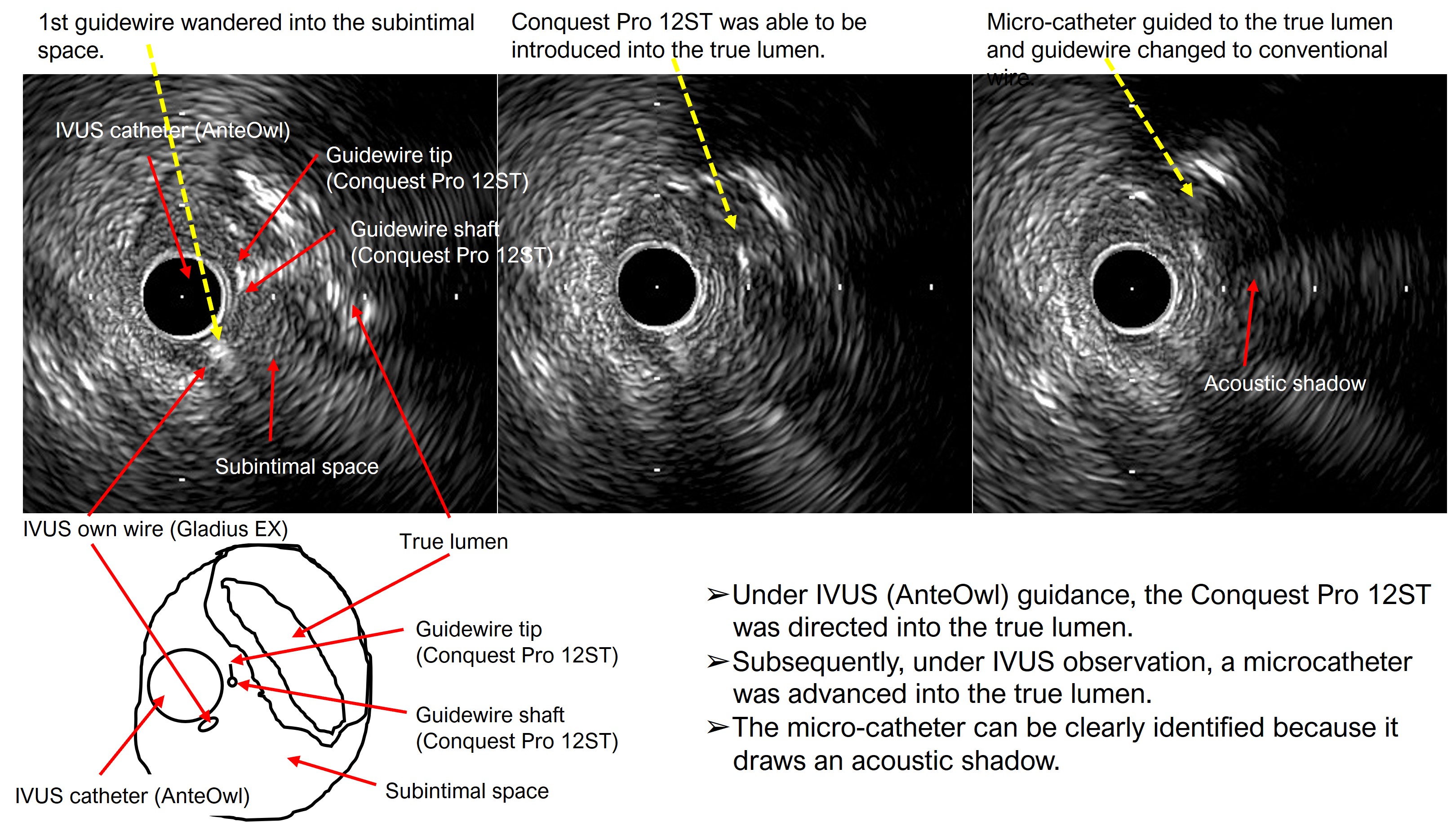
The procedure began via right and left femoral arteries using Launcher 8F EBU3.5SH and 7F SAL0.75SH guiding catheters. Zizai 150 cm and Corsair Pro 135 cm microcatheters were used. An antegrade approach with wire escalation from SION to XT-A and Conquest Pro 8-20 was attempted. SION and a 2.5×15 mm Ryurei balloon were used as anchors, but a heavily calcified “full moon-like” distal LAD lesion could not be crossed. GUIDEPLUS 5F with a 2.5×15 mm Ryurei enabled guide extension lock, though attempts with Ryurei 1.0×5 mm and Mogul SP Thinner 1.5F failed. Using SASUKE 145 cm, Gladius EX was redirected into the subintimal space via Corsair Pro and a 2.25×15 mm Ryurei. ELCA (0.9 mm) and PTCRA with FINECROSS MG and Mogul SP Thinner were unsuccessful as the RotaWire could not cross. Subsequent ballooning with Ryurei 2.25×15 mm and Hiryu Plus 2.5 mm was performed. ADR using Caravel MC and Conquest Pro 12ST achieved true lumen re-entry, followed by stenting with GUIDEPLUS II ST 6F and DESs.
Case Summary
It was one effective option for CTO PCI with severely calcified lesions accompanied by full moon-like calcification using HydroDynamic contrast Recanalization followed by Tip-detection Antegrade Dissection Re-entry method.