Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251110_008
Triple Vessel Disease in Severe Ischemic Cardiomyopathy
By Karen Pui Shan Shek
Presenter
Karen Pui Shan Shek
Authors
Karen Pui Shan Shek1
Affiliation
Tuen Mun Hospital, Hong Kong, China1
View Study Report
CASE20251110_008
Coronary - Complex PCI - Multi-Vessel Disease
Triple Vessel Disease in Severe Ischemic Cardiomyopathy
Karen Pui Shan Shek1
Tuen Mun Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
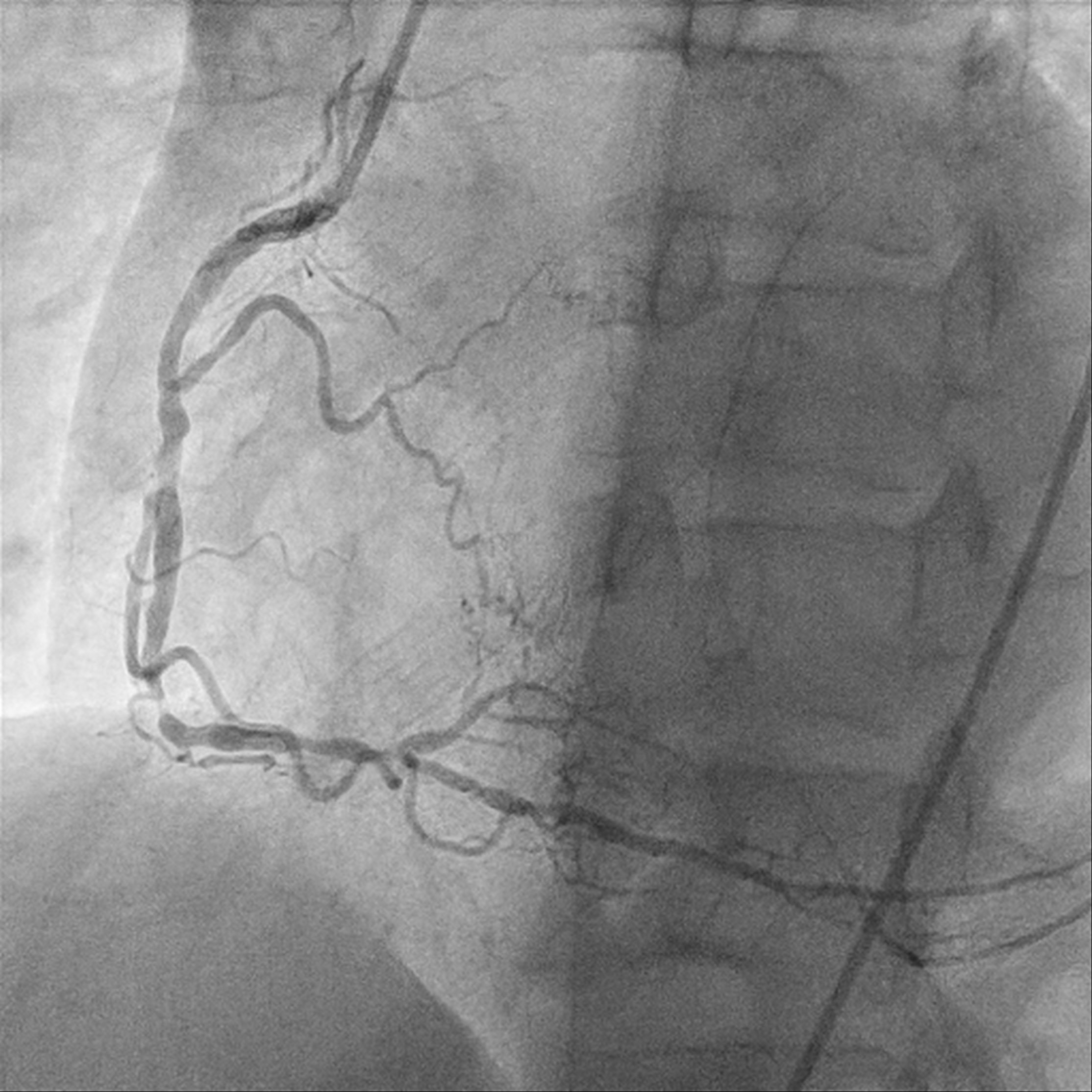
A 49-year-old male who is a chronic smoker and ex-IV drug addict was presented as heart failure and NSTEMI. Severely impaired LV systolic function of 15%, global hypokinesia. Calcified coronary arteries with mRCA severe stenosis, mid to distal RCA critical lesion; retrograde flow from PL branch to mLAD. mLAD CTO with bridging collaterals. LCX diffuse moderate stenosis, with collateral to PL branch. MRI heart confirms viable myocardial over LAD territory, CABG turned down.

Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Interventional Management
Procedural Step
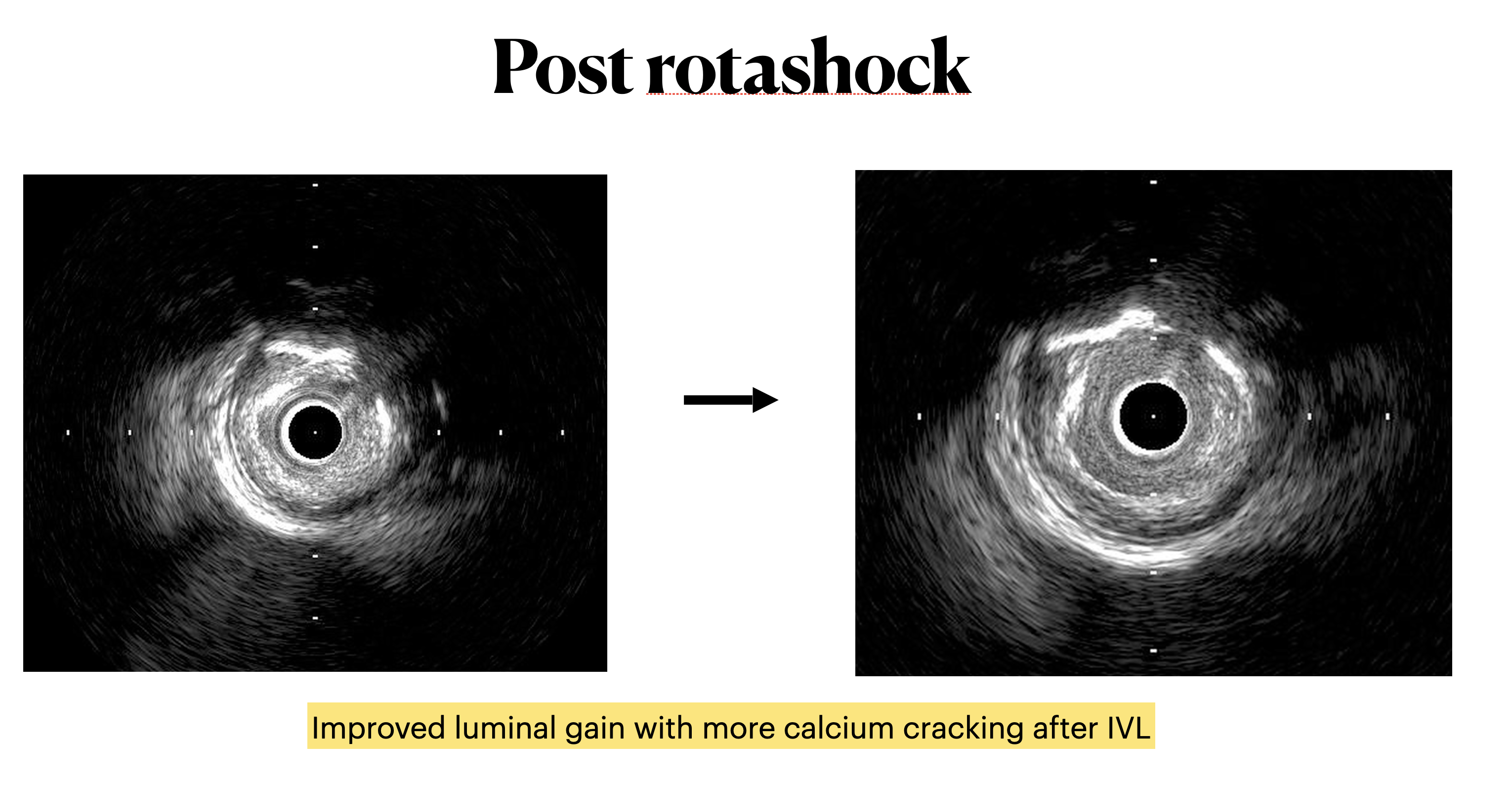
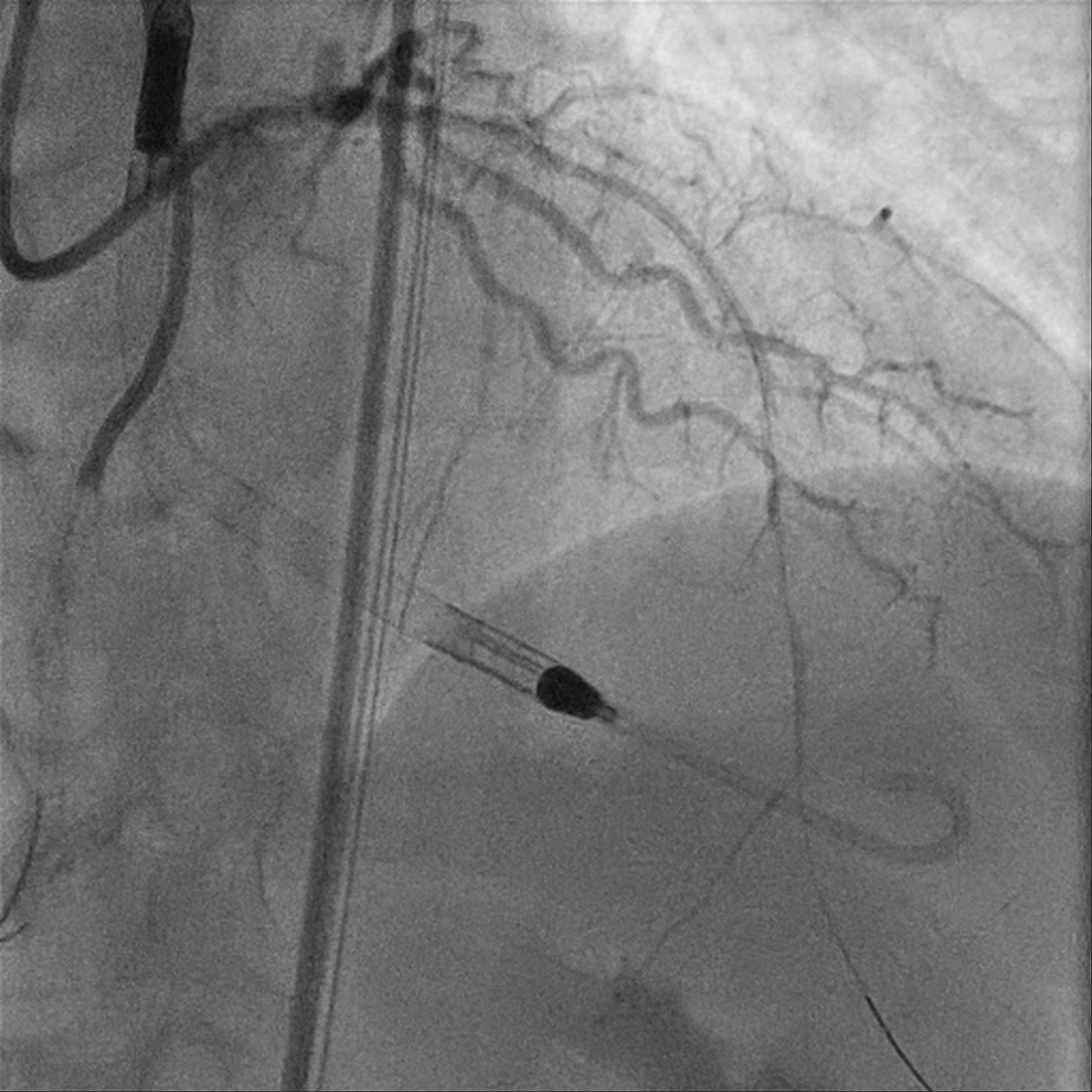
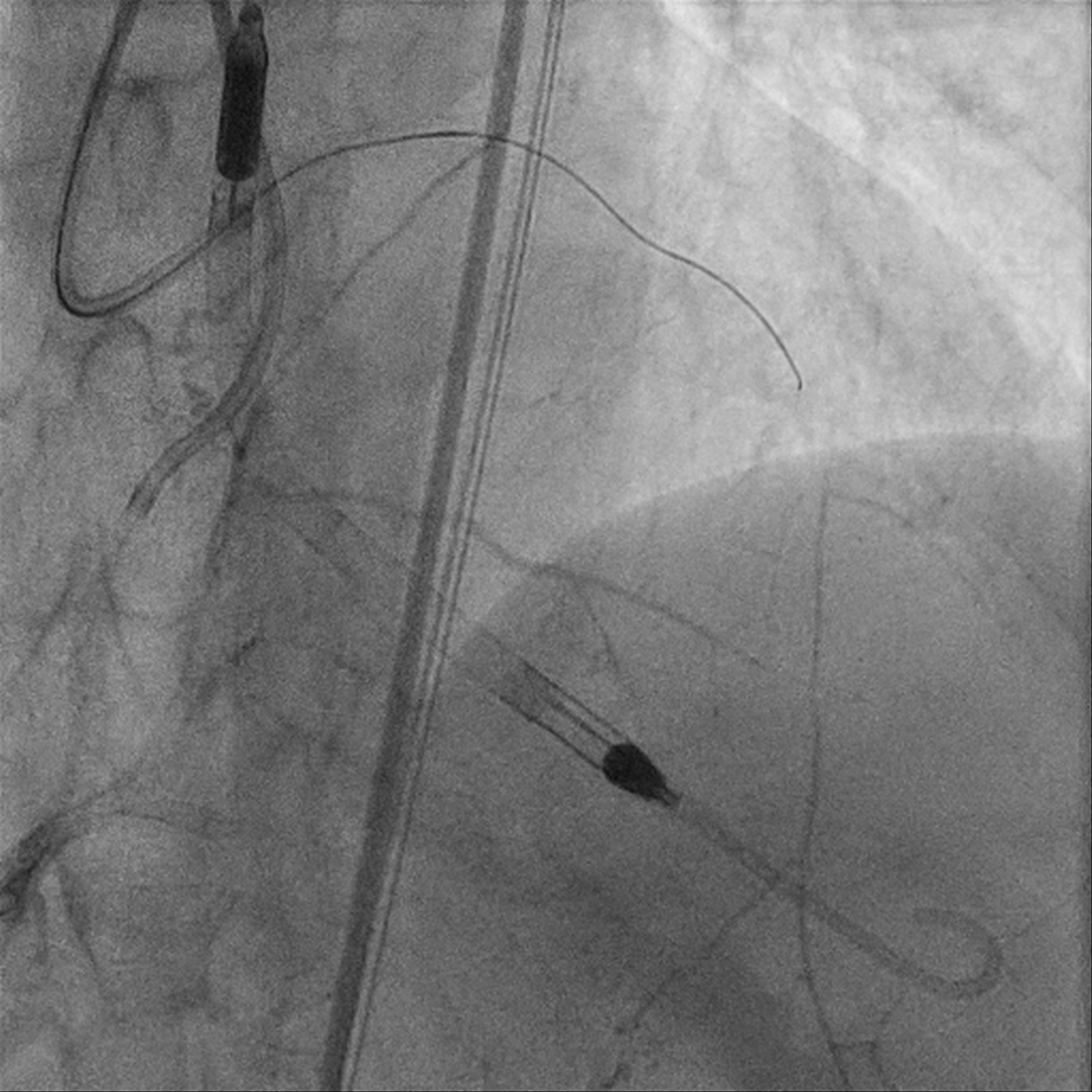
Upfront MCS support using Impella CP via R CFA. Eccentric calcified plaque over m-dRCA, fibrofatty atheroma elsewhere. Initially plan for DCB over dRCA, however developed distal dissection, pRCA to PDA stented with total of 4 stents. Impinged PL branch ostium after stenting, branch rewired then POBA. Final IVUS and angiography shows good results. mLAD CTO crossed with Gaia 2 but Caravel unable to cross. CTO segment then dilated with semi compliant 0.85mm balloon then 1.5mm balloons. IVUS confirmed wire within true lumen throughout with long segments of calcific lesion. Rotational atherectomy with 1.5mm burr for 7 passes then further predilation with NC 2.75mm balloon. However, complicated with no reflow afterwards. Prolonged inflation of long segment compliant balloon followed by adenosine injection improved flow. IVUS showed calcium fracture but inadequate luminal gain, decided for IVL. Total of 8 cycles using 2.5mm shockwave, post IVUS showed improved luminal gain with more calcium cracking. DCB to m-dLAD afterwards for calcified diffuse disease. However developed no reflow after Paclitaxel-coated DCB which complicated with 1 episode of VT requiring cardioversion. Repeated adenosine injection improved flow, patient stabilized.
Case Summary
A few lessons was learnt from this case. First lesson - balloon massaging for treatment of no reflow. Second lesson - combination in calcium modification therapy for better luminal gain and calcium cracking. Third lesson - DCB in CTO after calcium modification. Forth lesson - No reflow after Paclitaxel-coated DCB.