Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251110_002
Navigating the Unexpected: Managing Asymptomatic Severe Triple-Vessel Disease in a Young Patient
By Iskandar Mirza Amran
Presenter
Iskandar Mirza Amran
Authors
Iskandar Mirza Amran1
Affiliation
National Heart Institute, Malaysia1
View Study Report
CASE20251110_002
Coronary - Complex PCI - Multi-Vessel Disease
Navigating the Unexpected: Managing Asymptomatic Severe Triple-Vessel Disease in a Young Patient
Iskandar Mirza Amran1
National Heart Institute, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
A48-year-old gentleman with no known medical illness presented to our center for a routine medical check-up. He was asymptomatic and classified as NYHA Class I. During evaluation, his lipid profile revealed significantly elevated levels, with total cholesterol of 7.6 mmol/L and LDL-C of 5.5 mmol/L.
 1.avi
1.avi
Relevant Test Results Prior to Catheterization
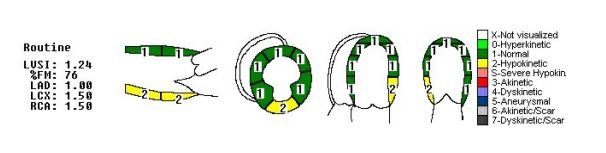
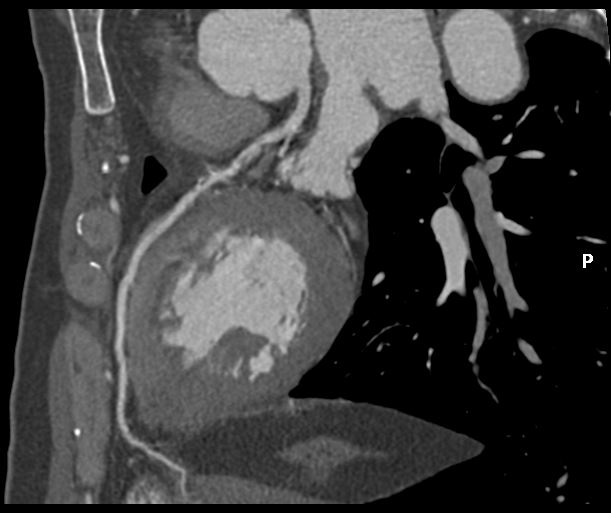
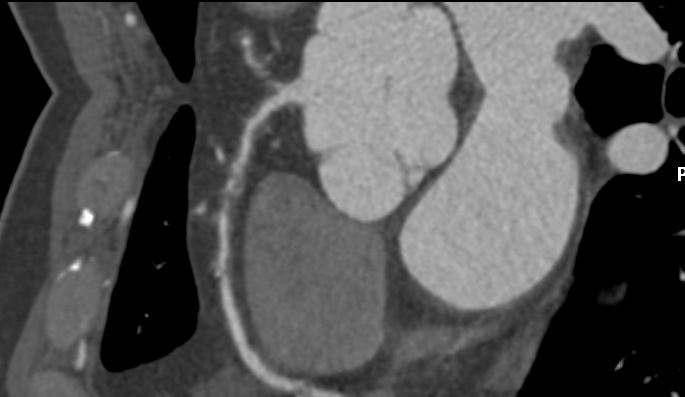
Echocardiogram showed good left ventricular ejection fraction of 53%. A multislice computed tomography coronary angiogram (MSCT-Coronary) demonstrated severe stenosis involving the proximal left anterior descending (LAD),proximal left circumflex (LCx),and proximal right coronary artery(RCA).The patient was subsequently admitted electively for diagnostic coronary angiography and possible percutaneous coronary intervention (PCI).

Relevant Catheterization Findings
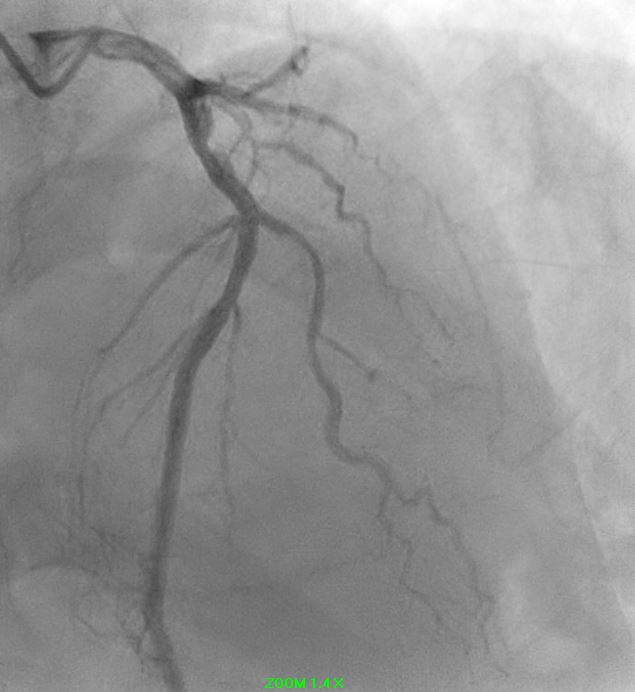
Angiographic assessment showed a normal left main stem, with severe proximal LAD disease exhibiting moderate calcification and providing retrograde collateral supply to both RCA and LCx. The LCx demonstrated severe mid-segment disease with subtotal occlusion of the obtuse marginal 1 (OM1) branch. The RCA showed severe proximal disease and total occlusion of the posterolateral(PL) branch.


1.avi
2.avi
3.avi
Interventional Management
Procedural Step
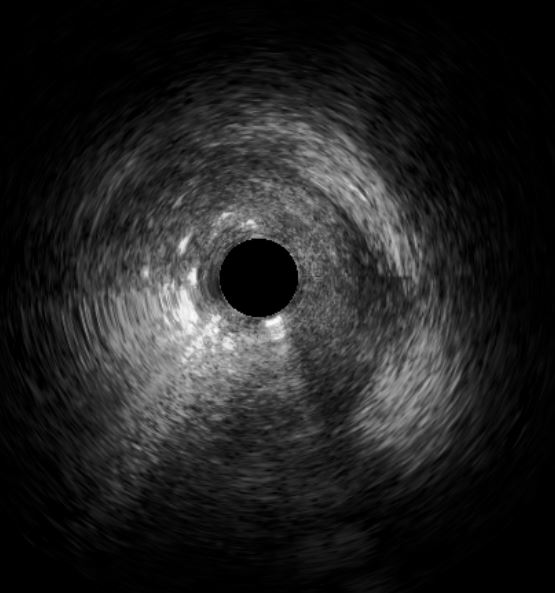
Initial engagement with a JR3.5/6Fr guiding catheter provided suboptimal support; this was switched to a SAL 0.75/6Fr guide, which offered only modest improvement. Lesion predilatation was performed with non-compliant balloons (0.85/15 mm and 1.5/15 mm) assisted by a guide extension catheter. Intravascular ultrasound (IVUS)revealed a distal reference vessel diameter of 3.0 mm and proximal reference of 3.5 mm, with evidence of white thrombus at the mid RCA. Further lesion preparation was performed using Naviscore balloons (3.0/15 mm distally and 3.5/15 mm proximally),achieving satisfactory luminal gain. A repeat IVUS run confirmed resolution of the white thrombus. Based on this, a drug-coated balloon(DCB)-only strategy was chosen. EssentialPro DCBs (2.0/40 mm for distal-mid segment, and 3.5/40 mm for mid-proximal segment) were successfully delivered and deployed. Post-procedure IVUS demonstrated significant improvement in minimum lumen area (MLA)—from 2.91 mm²to 4.07 mm² (distal) and 1.60mm² to 6.93 mm² (proximal).

postangioplasty.avi
preangioplasty.avi
1.avi
Case Summary
This case underscore severe important learning points. Firstly, intravascular imaging is invaluable in guiding interventional strategy — from assessing thrombus burden and vessel size to confirming adequate lesion preparation and luminal gain. Second, with careful lesion preparation and confirmed thrombus clearance, a DCB-only PCI strategy can be considered a feasible alternative to DES implantation in selected cases. Finally, early recognition and aggressive lipid-lowering therapy are critical in suspected familial hypercholesterolemia to prevent further atherosclerotic progression.