Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251109_008
Acute Stent Thrombosis Secondary to Hypersensitivity Reaction to Contrast Dye: A Rare Case of Type 3 Kounis Syndrome in a Filipino Patient
By Raymond Banquirigo, Celedonio Principe, Maria Tala Jovellanos, Christian Masaga, Jim Albert Perlas
Presenter
Jim Albert Perlas
Authors
Raymond Banquirigo1, Celedonio Principe1, Maria Tala Jovellanos1, Christian Masaga1, Jim Albert Perlas1
Affiliation
Cardinal Santos Medical Center, Philippines1
View Study Report
CASE20251109_008
Coronary - Complication Management
Acute Stent Thrombosis Secondary to Hypersensitivity Reaction to Contrast Dye: A Rare Case of Type 3 Kounis Syndrome in a Filipino Patient
Raymond Banquirigo1, Celedonio Principe1, Maria Tala Jovellanos1, Christian Masaga1, Jim Albert Perlas1
Cardinal Santos Medical Center, Philippines1
Clinical Information
Relevant Clinical History and Physical Exam
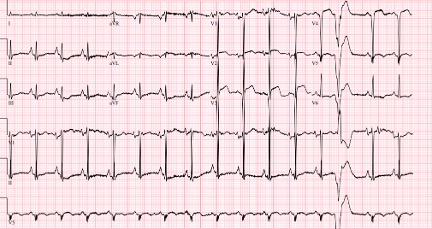
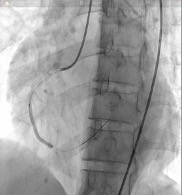
A case of a late 50's Filipino with no comorbidities who presented with chest pain. ECG done showed ST elevation of the inferior lead with elevated troponin. Patient was unstable prior to angiogram and intubated due to cardiac arrest with return of spontaneous circulation. Upon angiogram with injection of contrast, patient had eruption of maculopapular rash with hemodynamic instability and arrhythmias. Following angioplasty, patient had recurrence of ST elevation with stent thrombosis.


Relevant Test Results Prior to Catheterization
ECG was done which showed ST elevation at leads II,III,avF. Chest Xray showed cardiomegaly. Troponin I was elevated at 1310pg/ml. CBC showed leukocytosis (24.22 x 109/L) with neutrophilic predemoninance. 2D echo showed global hypokinesia with ejection fraction of 35%. Creatinine was elevated 208 umol/L with eGFR of 24mL/min.

Relevant Catheterization Findings
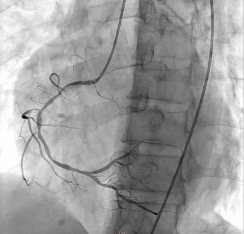
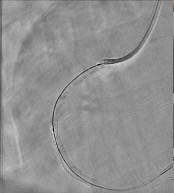
Left main artery is a 3.0 mm vessel without disease. Left anterior descending artery is a 2.5 mm vessel with tightest lesion of 70-80% tubular stenosis at the mid segment and left circumflex artery is a 2.5 mm vessel with a 80-90% tubular stenosis at the midsegment. Right coronary artery is a is a 2.5 mm diffusely diseased vessel with tightest lesion of 80-90% at the proximal. The AV continuation is a 2.0 mm vessel with luminal irregularities.

 RCA LAO CRA.mp4
RCA LAO CRA.mp4
Post stent.mp4
Stent thrombosis.mp4
Interventional Management
Procedural Step
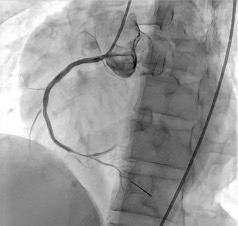
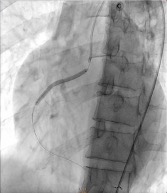
Percutaneous coronary intervention was initiated. A Xience Alpine 3.0 x 38mm drug-eluting stent (DES) was positioned at the mid to distal RCA and deployed at 16 atm and post-dilated using the same stent balloon inflated at 18 atm. Another Evermine 3.5 x 48mm drug-eluting stent (DES) was positioned at the proximal RCA and deployed at 18 atm and post-dilated using the same stent balloon inflated at 18 atm. Further dilation of the distal RCA was done using a Mini Trek 2.0 x 15mm balloon and inflated at 12 atm. However, j
manual displacement.mp4
angiogram post displacement.mp4
Case Summary
This case underscores the extraordinary risk and devastating consequences of the rarely encountered Type III Kounis Syndrome (KS), particularly when timely recognition is missed. The striking temporal relationship between allergic manifestations and sudden stent thrombosis reinforces the need to consider KS in patients with coronary events following exposure to potential allergens.