Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251109_007
Taming the Aneurysm and Piercing the CTO With a Hybrid Antegrade-Retrograde Approach
By Yu-Hung Tung, Jen-Kuang Lee
Presenter
Yu-Hung Tung
Authors
Yu-Hung Tung1, Jen-Kuang Lee1
Affiliation
National Taiwan University Hospital, Taiwan1
View Study Report
CASE20251109_007
Endovascular - Iliac / SFA Intervention
Taming the Aneurysm and Piercing the CTO With a Hybrid Antegrade-Retrograde Approach
Yu-Hung Tung1, Jen-Kuang Lee1
National Taiwan University Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
An 82-year-old male with chronic Critical Limb Ischemia (CLI) (PAOD Fontaine IV/Rutherford 6) was urgently admitted with an infected, non-healing right ankle wound and tendon exposure. The presentation was complicated by fever, tachycardia, a cold extremity, and nonpalpable pedal pulses, indicating critical infection and ischemia. Management was challenging due to the patient's self-discontinuation of anti-platelets following recent bleeding.

Relevant Test Results Prior to Catheterization
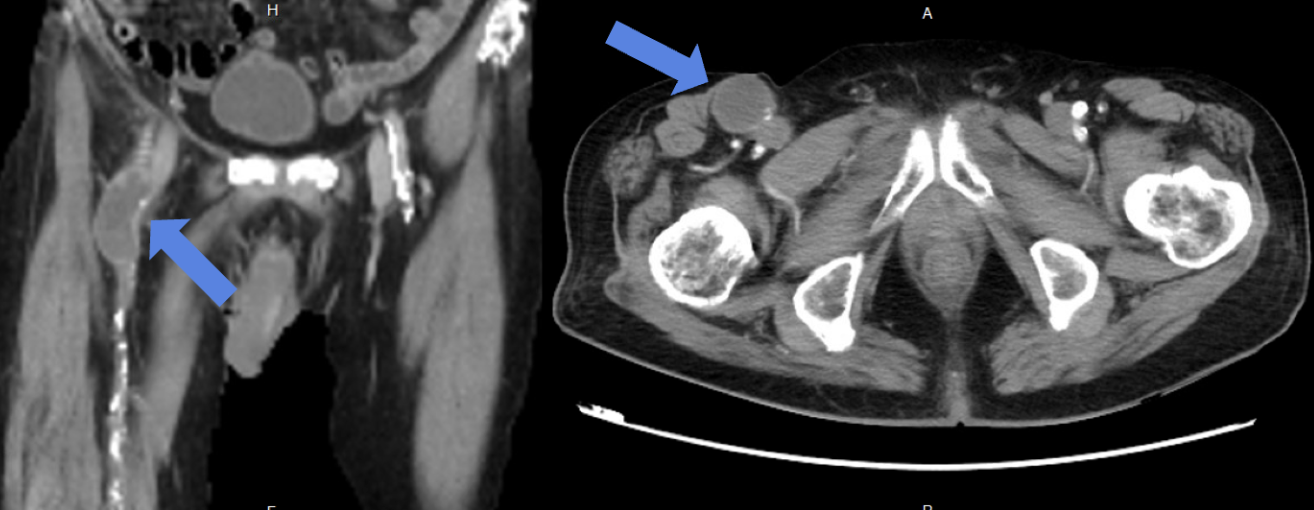
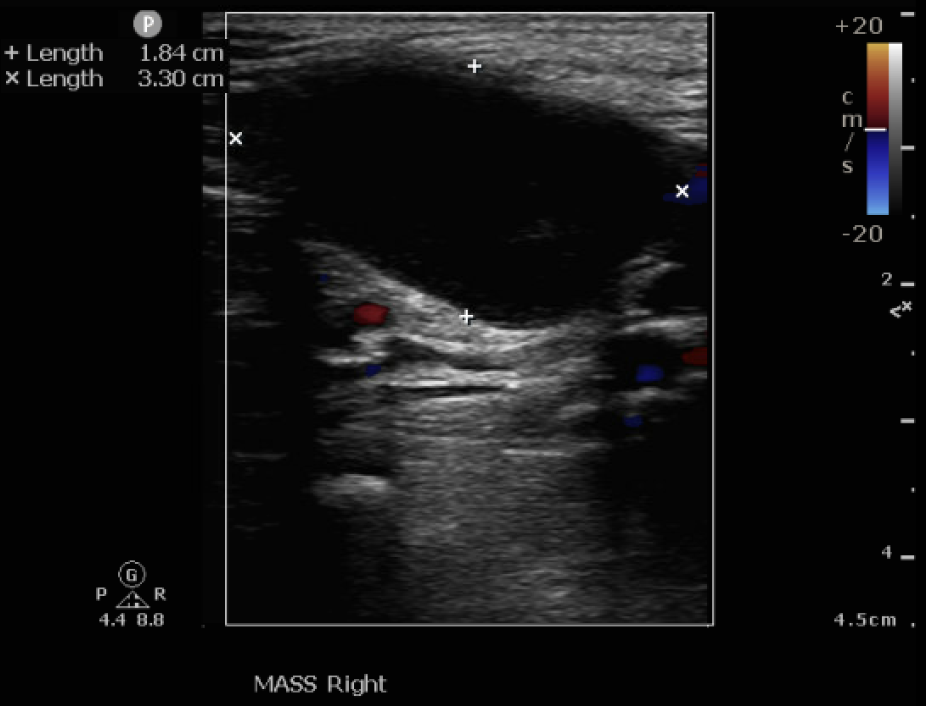
Lab data showed leukocytosis and significantly elevated C-Reactive Protein, alongside deteriorated renal function. Vascular Duplex showed monophasic flow and a hematoma near the Common Femoral Artery (CFA). CTA revealed Severe PAOD via extensive total occlusion from the right right External Iliac Artery (EIA) to the Superficial Femoral Artery (SFA), and a thrombosed aneurysm at the femoral bifurcation, and extensive Deep Venous Thrombosis (DVT) extending from the femoral vein distally.
Relevant Catheterization Findings
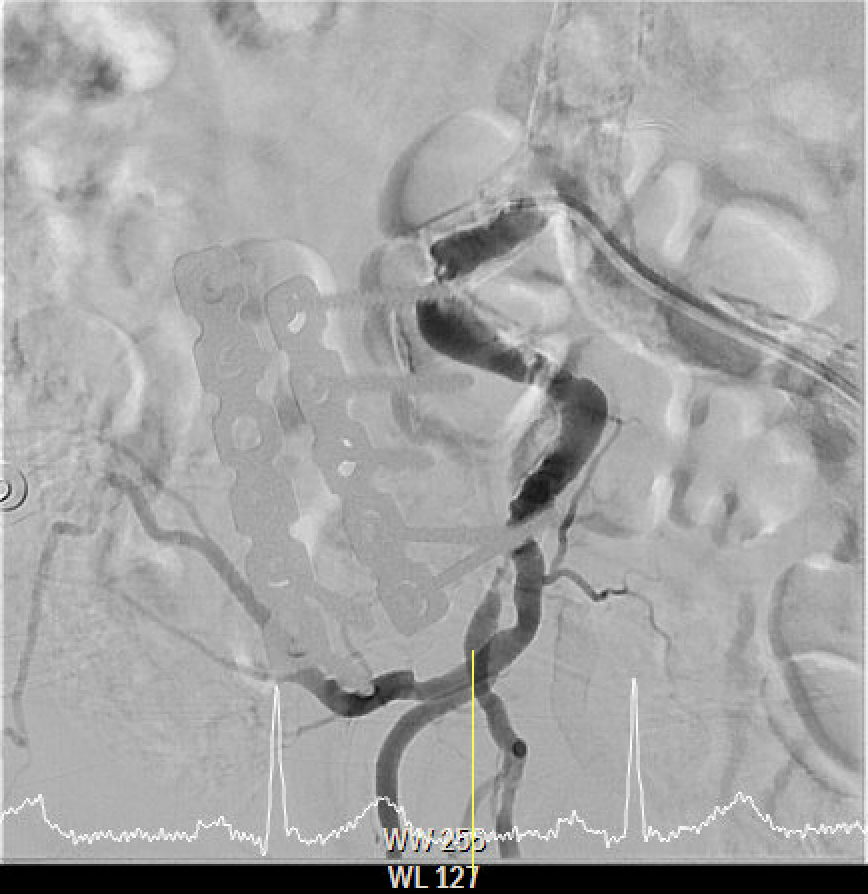
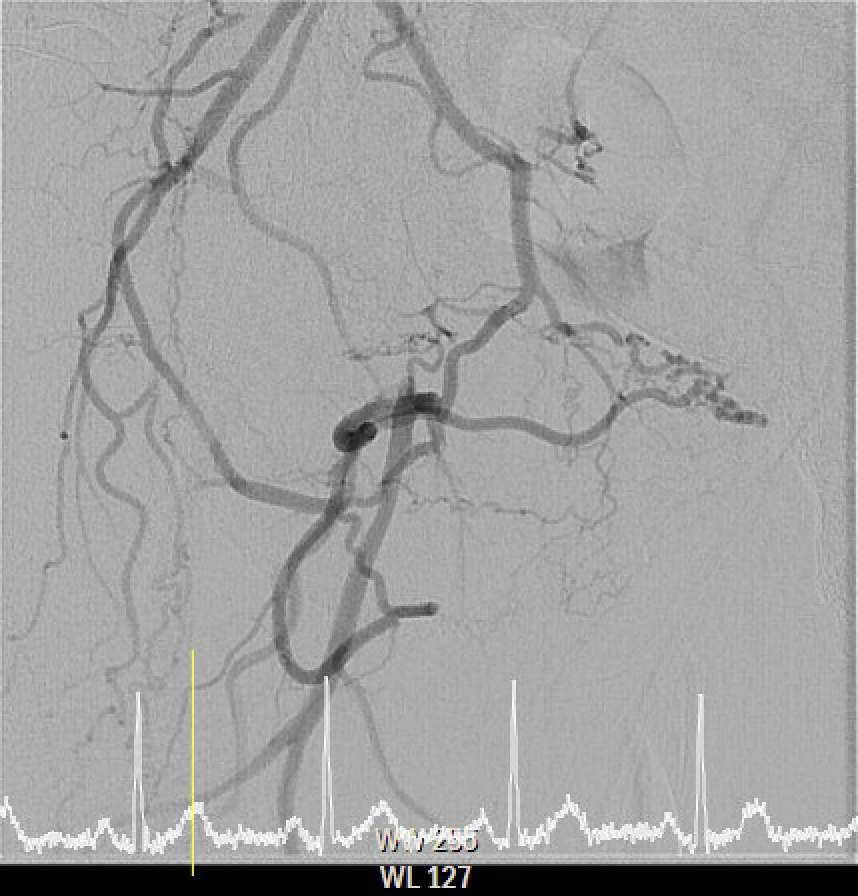
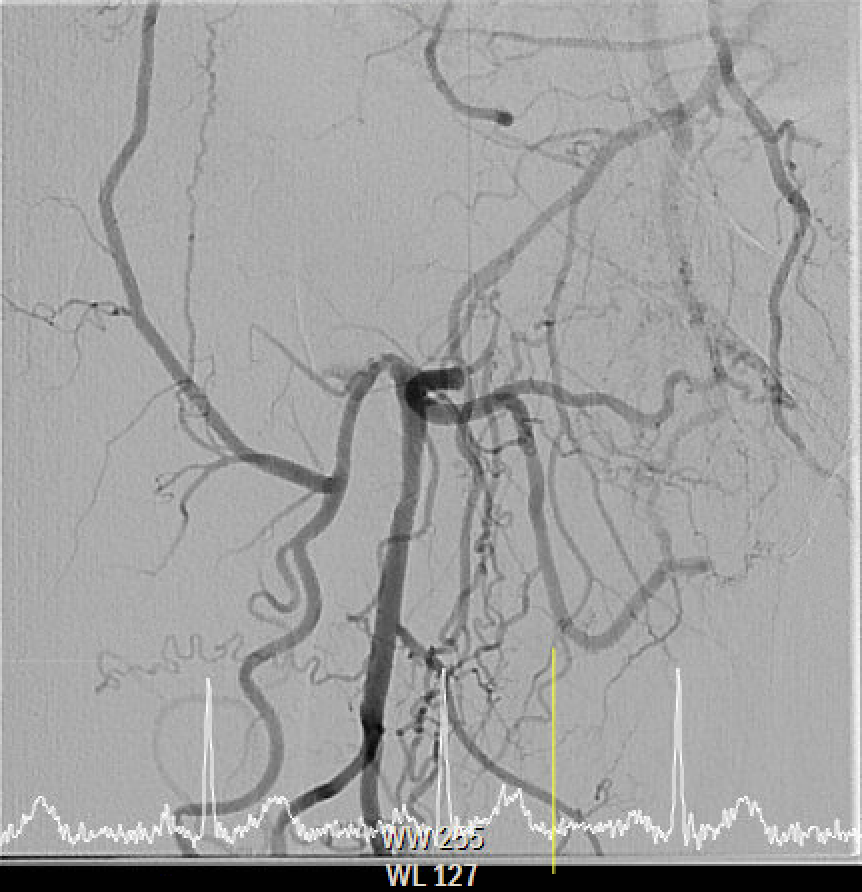
The angiography confirmed extensive Chronic Total Occlusion (CTO) of the right External Iliac Artery (EIA), Common Femoral Artery (CFA), and proximal Superficial Femoral Artery (SFA). The limb's circulation was critically dependent on collateral flow: the Deep Femoral Artery (DFA) was patent and supplying the distal SFA. Distally, a 50% stenosis was noted in the Popliteal Artery, but the Below-the-Knee (BTK) arteries were patent.
Interventional Management
Procedural Step
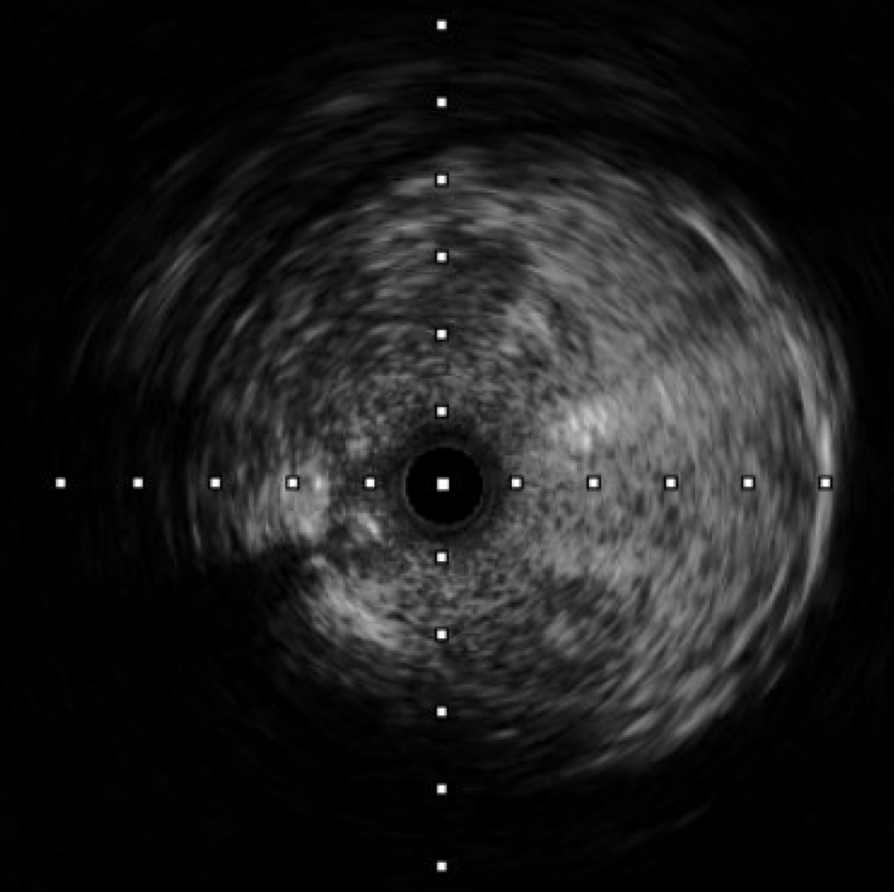
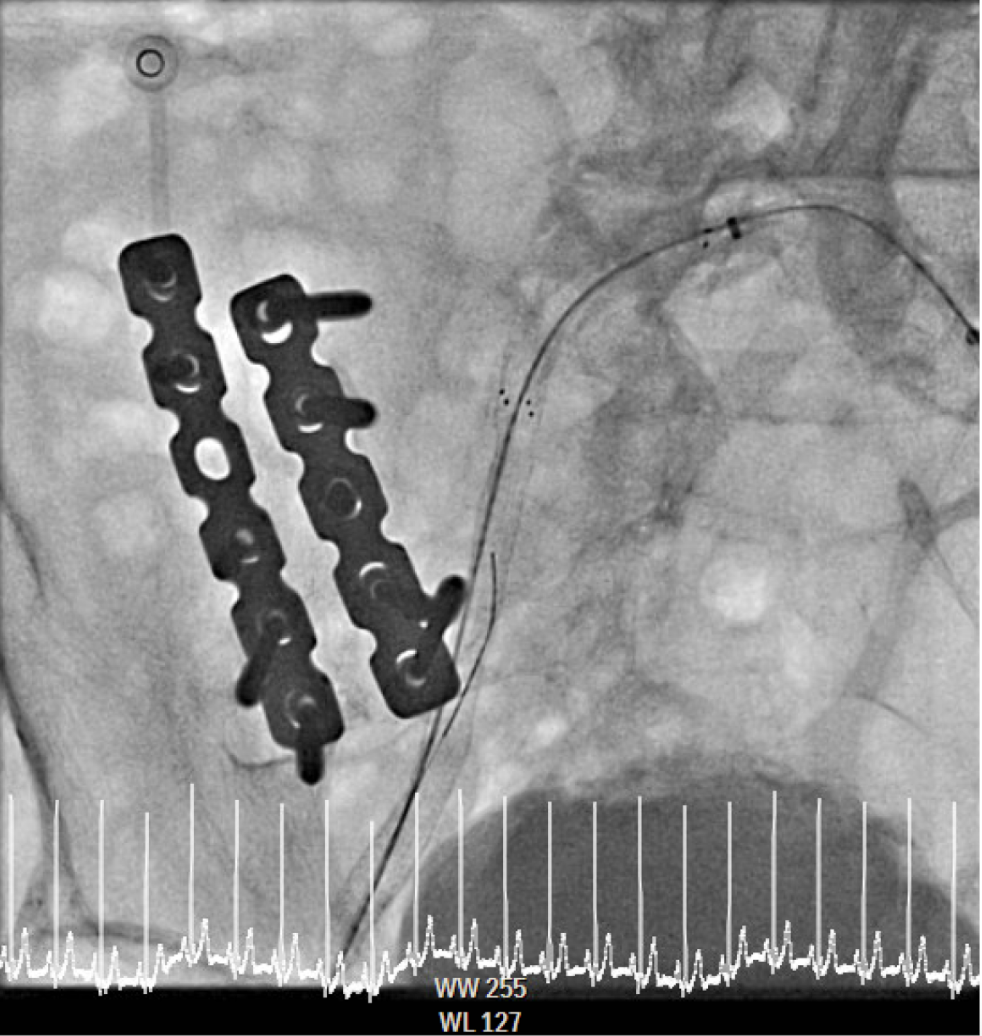
The procedure utilized a hybrid retrograde and antegrade approach. Retrograde access was established via a micropuncture kit under angiography guidance into the distal Superficial Femoral Artery (dSFA), but wiring attempts failed due to an intervening aneurysm, necessitating a switch to the antegrade route from the left brachial artery. A wire escalation technique, assisted by a microcatheter, successfully crossed the extensive CTO, and was met with retrograde microcatheter and externalized via the dSFA puncture site (retrograde access), establishing through-and-through wire access. Following initial balloon predilation and IVUS confirmation of diffuse thrombus, extensive angioplasty was performed. Definitive treatment involved deploying multiple overlapping GORE® VIABAHN® Endoprosthesis diameters (from 6mm to 8mm) from the dSFA proximally to the pEIA via left femoral access, effectively treating the long occlusion and excluding the aneurysm. A COOK Zilver Flex iliac stent reinforced the proximal landing zone. The stented segment was rigorously post-dilated up to 12 atm. The procedure concluded with a Drug-Eluting Balloon (DEB) PTA (BOSTON Ranger Paclitaxel-Coated PTA Balloon Catheter) to the dSFA to mitigate restenosis in the non-stented region. Final angiography confirmed good flow without distal embolization.

Case Summary
This case demonstrates the efficacy of a hybrid retrograde/antegrade approach to overcome a challenging CTO and a thrombosed femoral aneurysm. This standard relies on deploying multiple overlapping stent-grafts to effectively treat long lesions and simultaneously exclude the aneurysm, minimizing the need for high-risk open surgery. A key advanced technique used was the final application of the DEB to the distal SFA, which is proven to significantly reduce the risk of restenosis. The stable patient outcome and positive angiography confirm that advanced percutaneous interventions are the preferred limb-saving option for complex, high-risk PAOD patients.