Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251109_006
A ‘Running Naked’ Procedure: A Case of Transradial Subclavian Artery Stenosis Stenting Without Guiding Catheter
By Devie Caroline, Ye Cheng
Presenter
Devie Caroline
Authors
Devie Caroline1, Ye Cheng2
Affiliation
Husada Utama Hospital, Indonesia1, Xiamen Cardiovascular Hospital Xiamen University, China2
View Study Report
CASE20251109_006
Endovascular - Other Endovascular Interventions
A ‘Running Naked’ Procedure: A Case of Transradial Subclavian Artery Stenosis Stenting Without Guiding Catheter
Devie Caroline1, Ye Cheng2
Husada Utama Hospital, Indonesia1, Xiamen Cardiovascular Hospital Xiamen University, China2
Clinical Information
Relevant Clinical History and Physical Exam
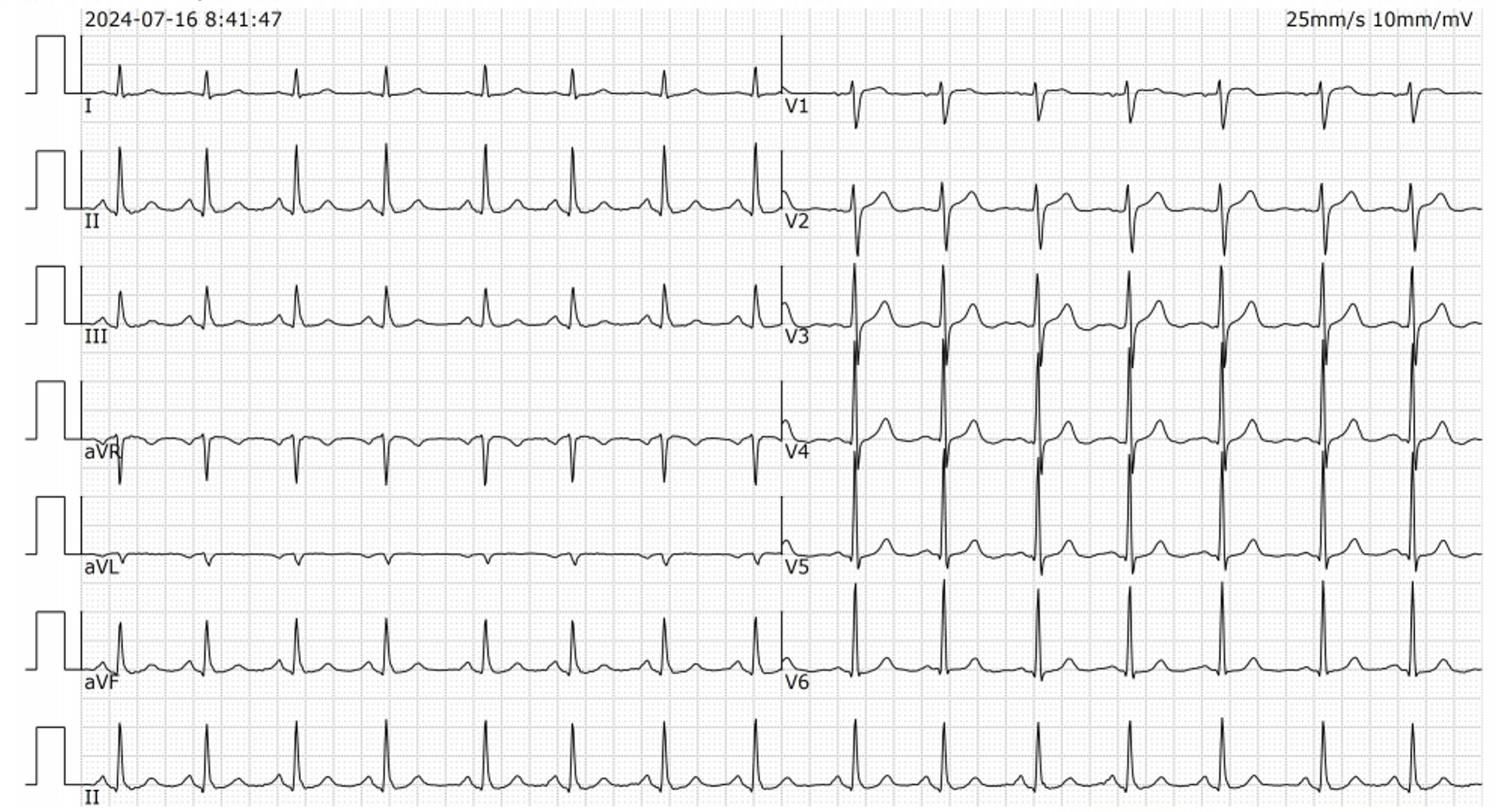
A 68-year-old gentleman has had dizziness and neck discomfort for about one year. His past medical history were cerebral infarction, PTA stent of right internal carotid, and PTCA Stent of LM-LAD.His risk factors were hypertension and smoker for more than 40 years. Left arm BP was 135/65 mmHg, right arm BP was 147/79 mmHg, no remarkable findings on thorax. ECG shows normal sinus rhythm.
Relevant Test Results Prior to Catheterization
His CT angiography of the abdominal aorta and lower extremity arteries showed atherosclerosis of the abdominal aorta and no contrast enhancement distal of the left renal artery and in the mid-distal common iliac arteries, suggesting occlusion. There were multiple tortuous and widened collateral vessels in the abdominal wall and pelvis.His complete blood count was within the normal limit; the others are shown in the table.
Relevant Catheterization Findings
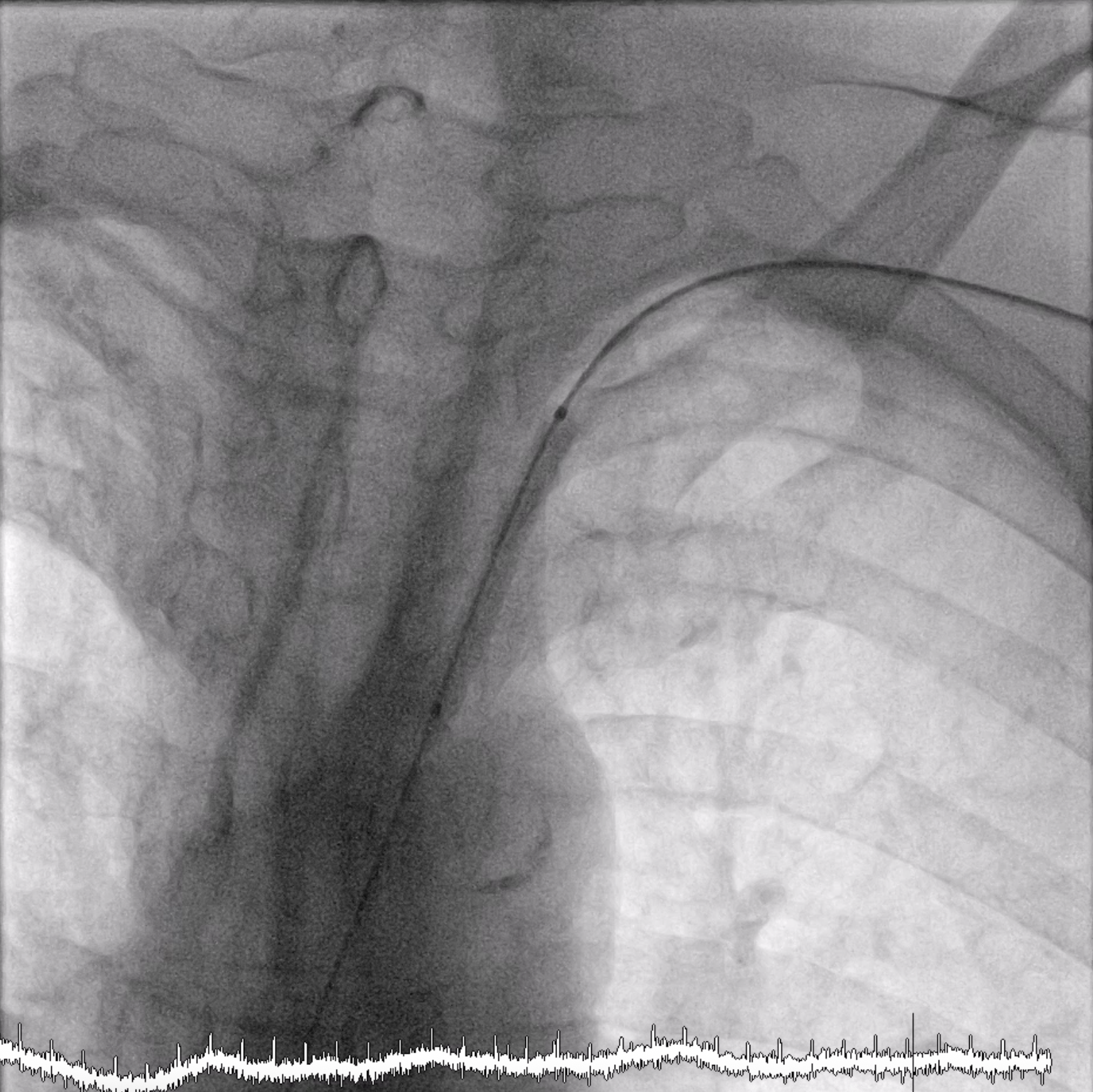
The subclavian angiography was performed by left radial approach (6 Fr sheath) and using a diagnostic catheter JR 4.0. There was 90% stenosis of the left subclavian artery near the aortic arch (black arrow).

 Stenosis subclavian.png
Stenosis subclavian.png
01.mp4
Interventional Management
Procedural Step
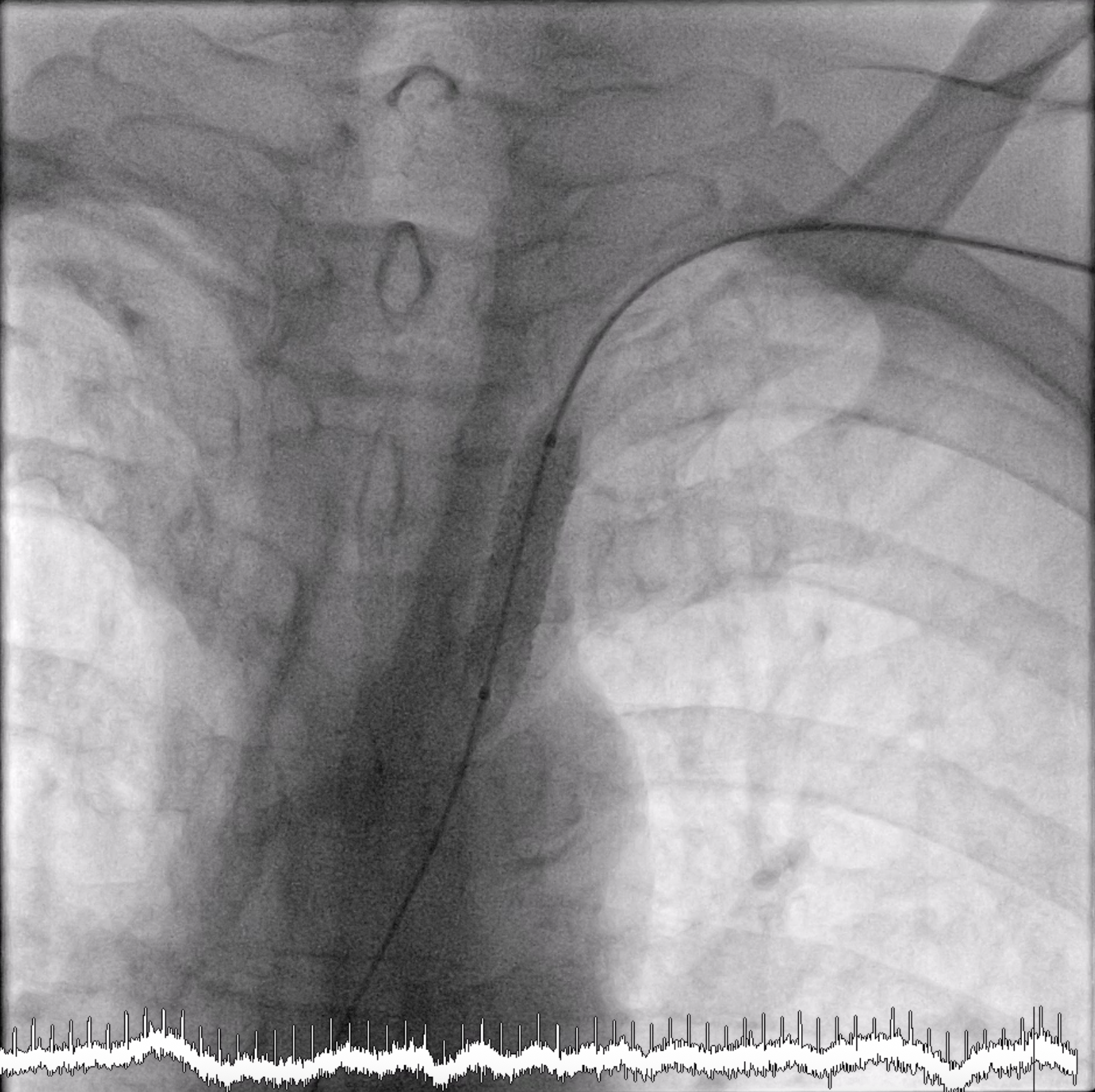
After we performed cine-angiography of the left subclavian artery using AP view, we drew the upper and lower border of the stenosis location with permanent marker on the machine’s screen. We decided not to use a guiding catheter to intervene the left subclavian stenosis. Using JR 4.0 diagnostic catheter, we inserted 0.035” PTFE J tip guide wire 150 cm into the left subclavian artery, crossed the lesion, and secured distally into the aorta.We pulled out the JR 4.0 diagnostic catheter, then we delivered a MustangTM Balloon Dilatation Catheter (Boston Scientific) 5.0 x 40 mm into the lesion. We positioned the Mustang balloon according to the ‘mark’ that we made in the screen, then inflated it.After pre-dilating with the balloon, next we delivered ExpressTM Vascular LD Stent (Boston Scientific) 8.0 x 27 mm into the lesion (according to the ‘mark’) and deployed the stent. After that, we advanced the balloon stent about 3-4 mm further and post-dilated the stent.The final result was good with no residual stenosis and no dissection.

03.mp4
04.mp4
06.mp4
Case Summary
We successfully performed PTA stent placement in the subclavian artery via left radial artery access without a guiding catheter. This "running naked" procedure was possible as long as we could maintain a stable position during balloon dilatation and stent deployment. There would be a risk of plaque embolization in this procedure, but this complication did not occur in this patient.