Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251109_005
Fulminant Typhoid Myocarditis Presenting With Cardiogenic Shock Mimicking STEMI
By Samuel Kristanto, Edwin Sukmadja, Roy Christian, Intan Muthia Rani
Presenter
Samuel Kristanto
Authors
Samuel Kristanto1, Edwin Sukmadja1, Roy Christian1, Intan Muthia Rani1
Affiliation
Primaya Hospital Tangerang, Indonesia1
View Study Report
CASE20251109_005
Heart Failure - Cardiogenic Shock
Fulminant Typhoid Myocarditis Presenting With Cardiogenic Shock Mimicking STEMI
Samuel Kristanto1, Edwin Sukmadja1, Roy Christian1, Intan Muthia Rani1
Primaya Hospital Tangerang, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
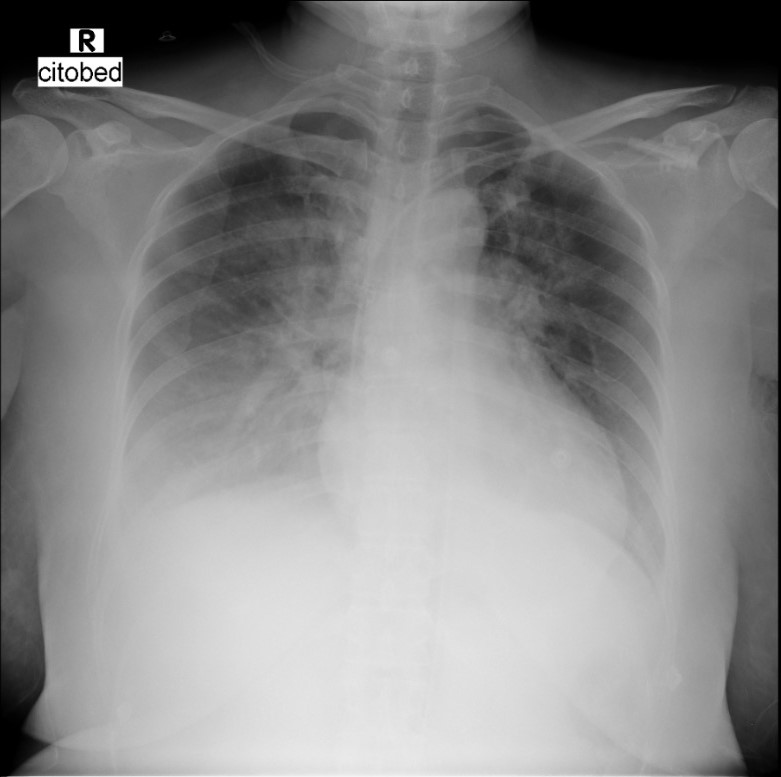
A 51-year-old woman with a history of type 2 DM was referred to our hospital with sudden onset of chest pain and shortness of breath. She had been hospitalized the day before with fever, nausea, and diarrhea. Prior to transfer, her condition deteriorated into cardiogenic shock with acute heart failure for which norepinephrine, dopamine, furosemide, and oxygen via NRM was administered. Upon arrival, her blood pressure was 80/40 mmHg, CRT > 3 seconds, and bilateral crackles were heard.

Relevant Test Results Prior to Catheterization
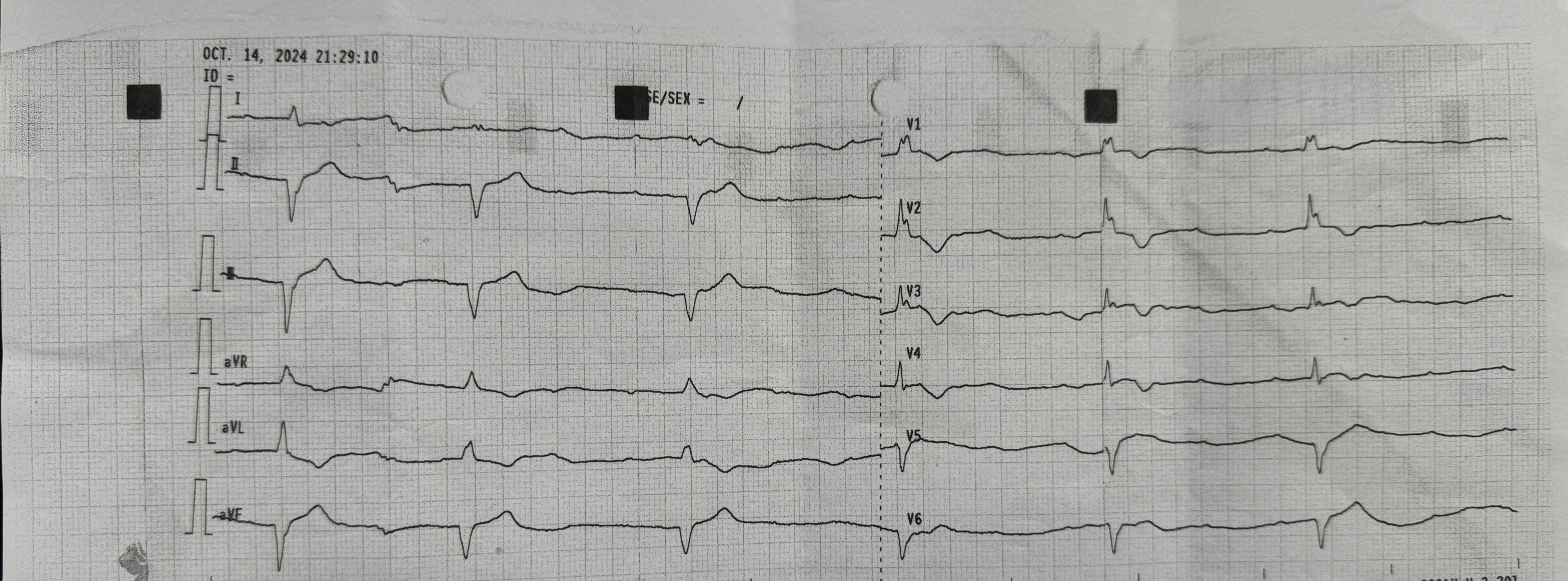
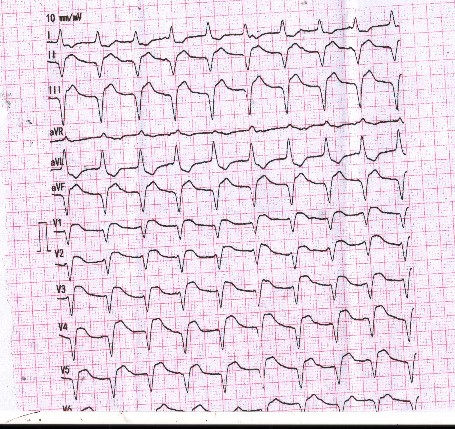
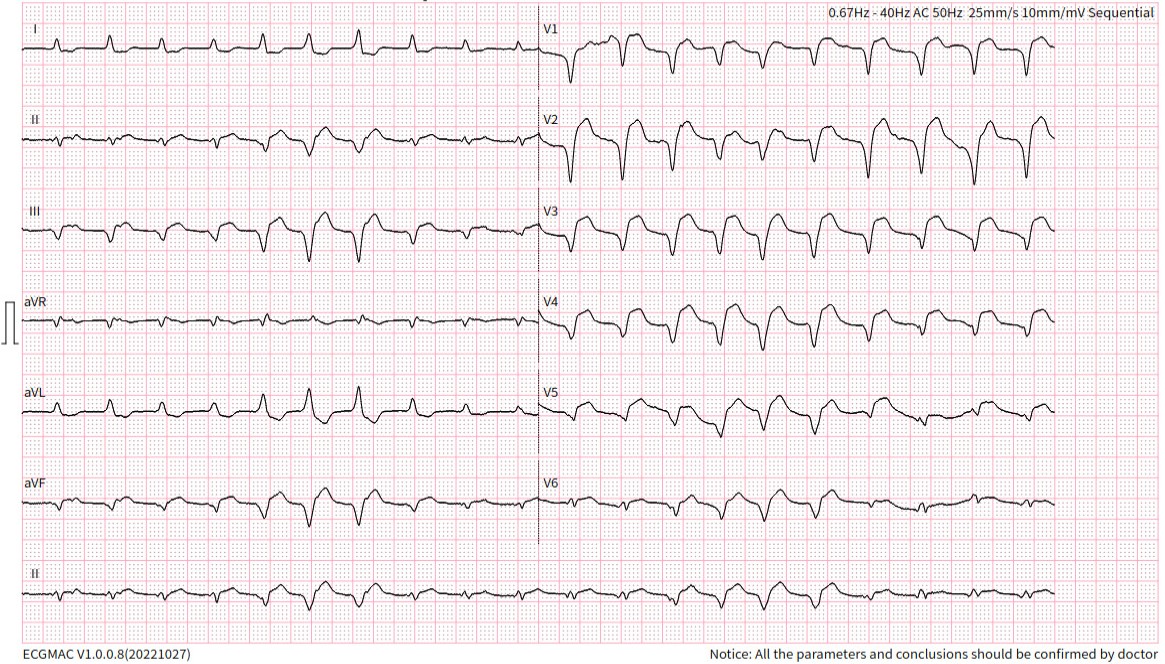
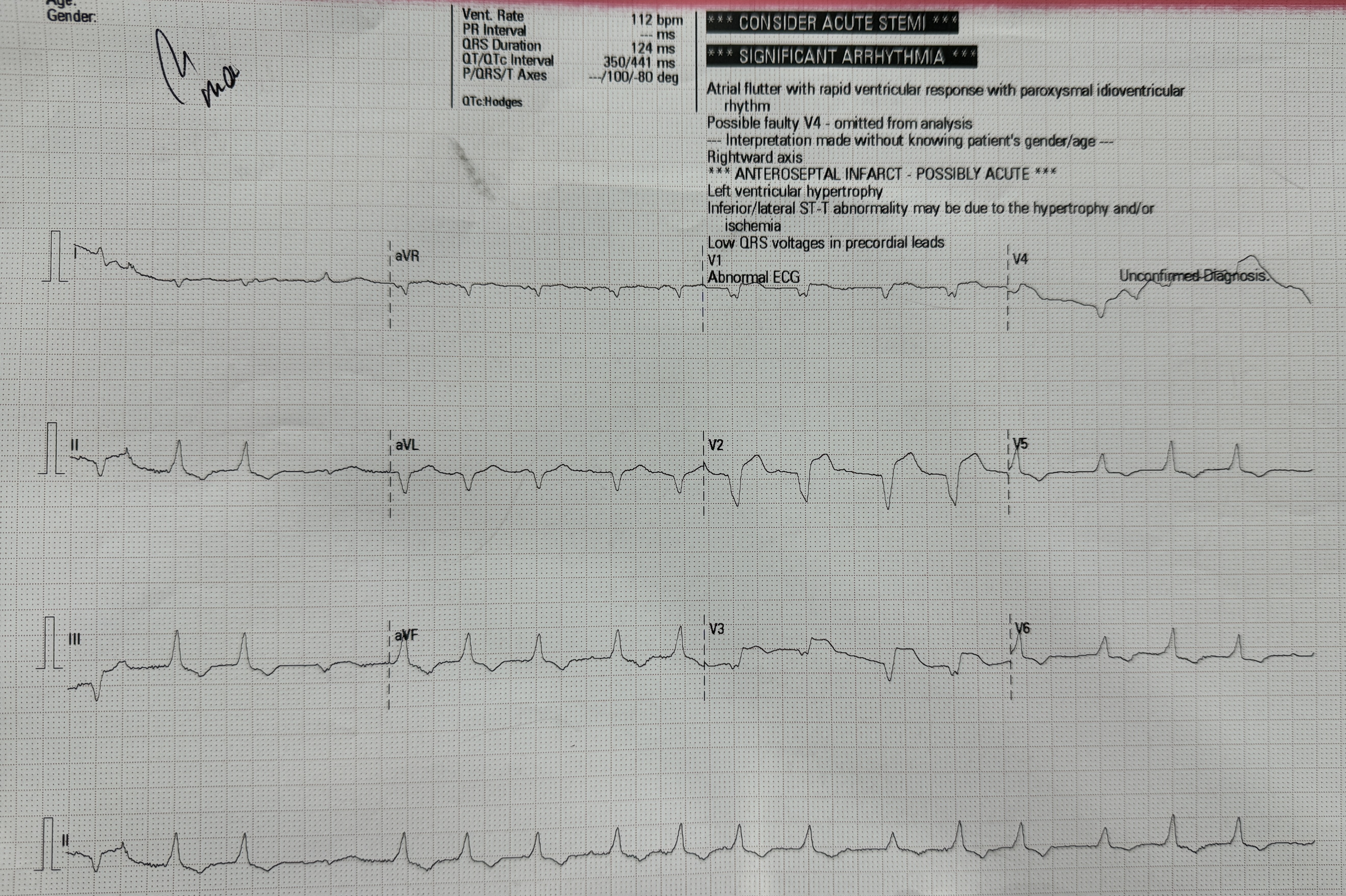
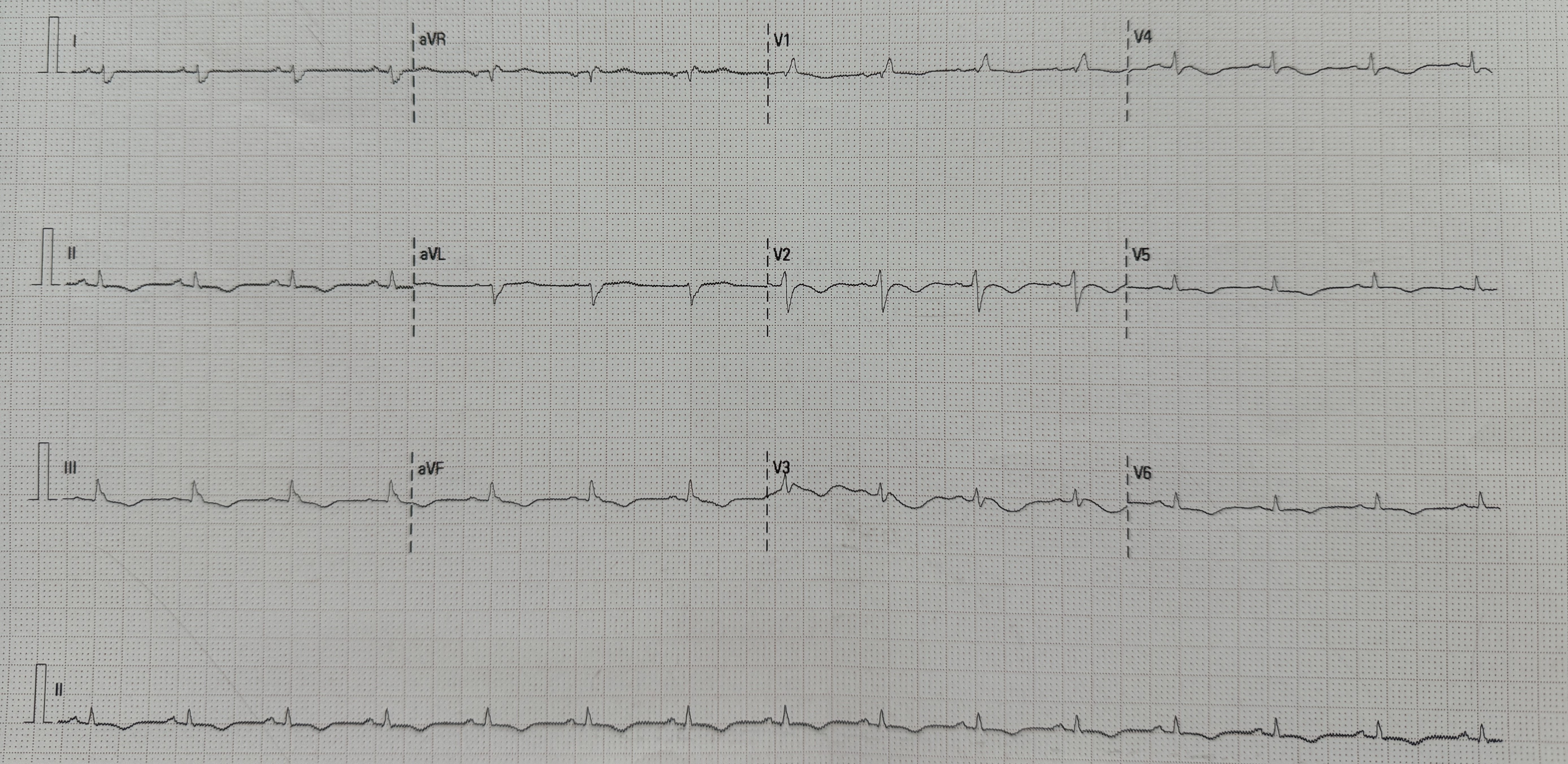
At the onset of chest pain, her electrocardiogram (ECG) showed total AV block and serial ECG showed QRS and ST-T changes. New onset Left Bundle Branch Block (LBBB) and ST-elevation was found in the inferior and anterior leads. Laboratory tests revealed elevated troponin levels consistent with acute STEMI and a positive IgM Salmonella Typhi (TUBEX) test.She had received a loading dose of dual antiplatelet therapy, fondaparinux, and ceftriaxone in the previous hospital.
Relevant Catheterization Findings
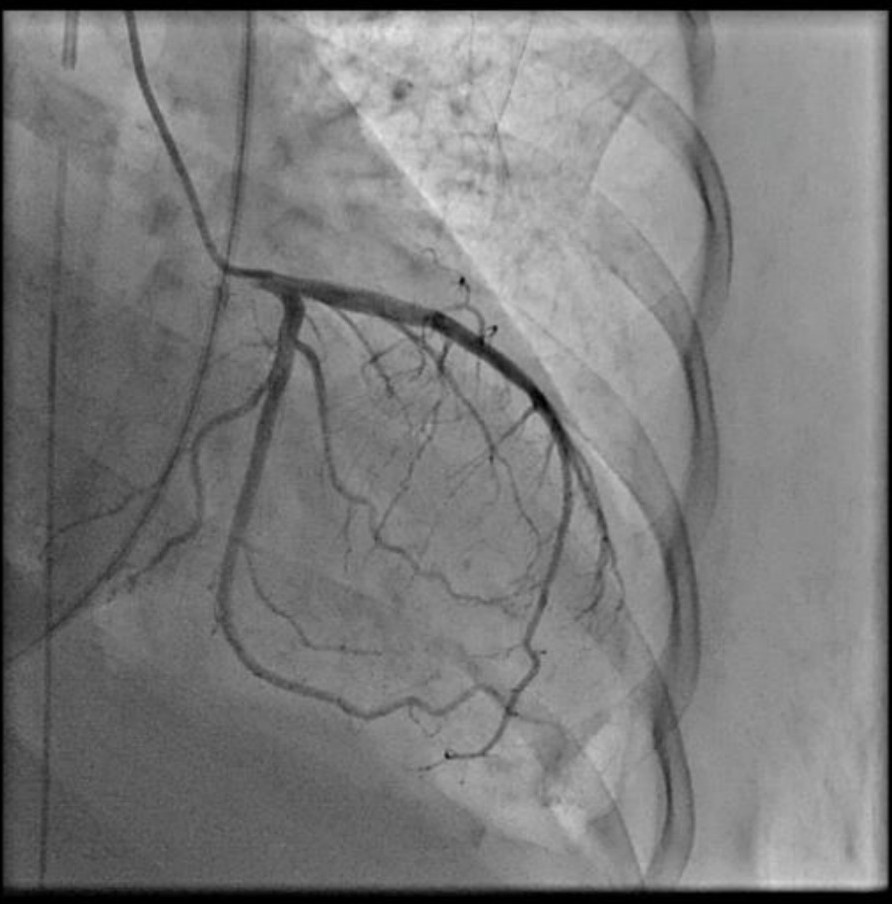
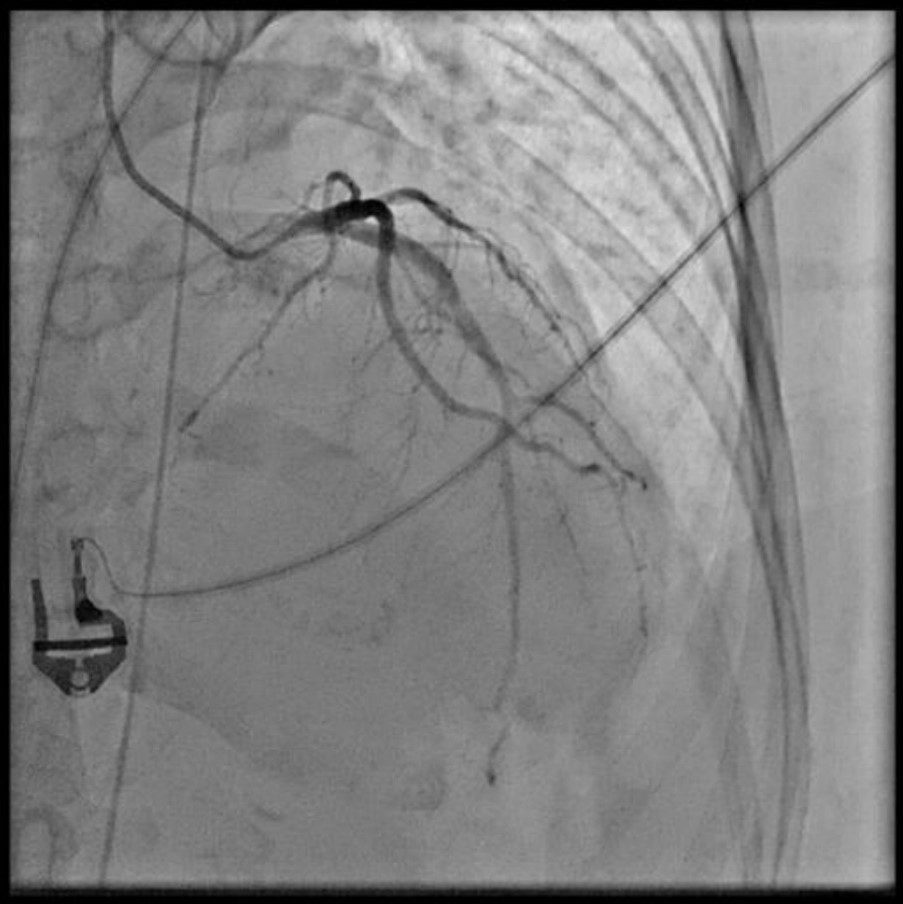
As STEMI could not be ruled out, immediate coronary angiography (CAG) was performed, revealing no significant coronary arteries stenosis. Despite optimal inotropes, cardiogenic shock persisted, prompting intra-aortic balloon pump (IABP) insertion during CAG

 cag ladlcx.mov
cag ladlcx.mov
cag rca.mov
Interventional Management
Procedural Step
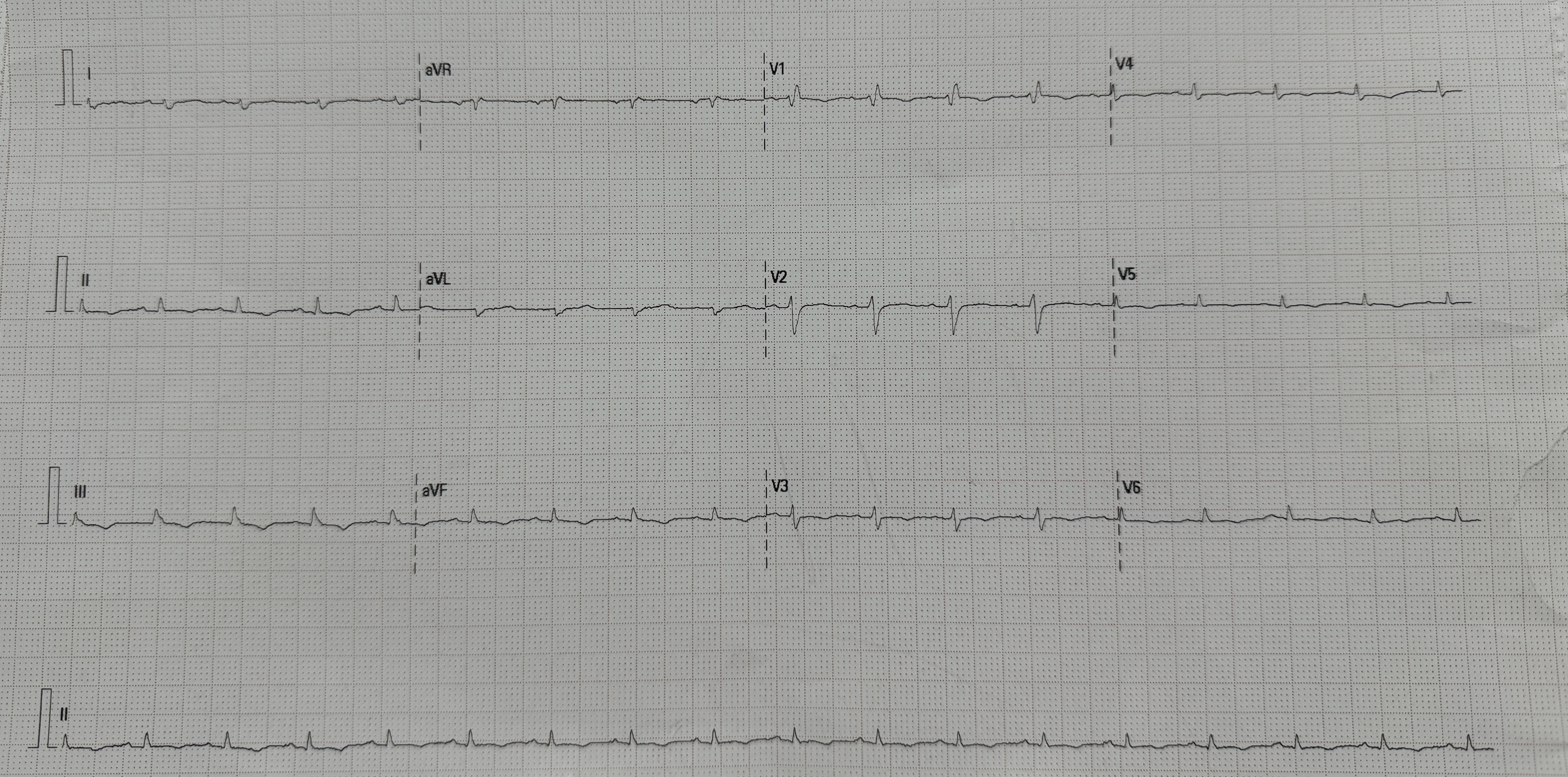
Based on the clinical presentation, ECG, and laboratory results, the initial working diagnosis was Anterior STEMI with KILLIP Class IV. CAG was then performed via radial artery using a 6-French introducer sheath, revealing no significant stenosis in the coronary arteries. As the cardiogenic shock still persisted despite optimal inotrope and vasopressor, an IABP was then inserted via femoral artery with the initial setting of 1:2 assist ratio. She was then transferred to the intensive care unit (ICU) where bedside echocardiography revealed a left ventricular ejection fraction (LVEF) of 48% without regional wall motion abnormalities, supporting a non-ischemic etiology. During hospitalization the patient developed acute kidney injury (AKI) with anuria. Further workup for myocarditis showed elevated C-reactive protein (CRP), high procalcitonin levels, and metabolic acidosis. Blood culture was sterile as she had been given antibiotic before. Given rapid clinical deterioration, broad-spectrum antibiotics (meropenem and cefoperazone) were initiated, and hemodialysis was performed. Her condition steadily improved throughout treatment. The IABP was successfully weaned off after four days, and inotropes were gradually tapered off. Serial ECGs also showed gradual resolution of the ST segment elevation and LBBB. After ten days of optimal antibiotics treatment, she continued to improve and was safely discharged from the hospital.
Case Summary
Myocarditis secondary to Salmonella typhi is an uncommon but serious complications and should be considered particularly in endemic regions or those with a history of recent infection. ECG findings may mimic STEMI and fulminant myocarditis may mask itself as cardiogenic shock from an acute coronary syndrome (ACS) origin. Normal CAG with elevated inflammatory markers and cardiac enzymes may support the suspicion of myocarditis when endomyocardial biopsy or cardiac MRI couldn't be performed. Early diagnosis is essential for appropriate management and improved patient outcomes. Heightened clinician awareness of this rare presentation can prevent diagnostic delays and reduce morbidity.