Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251109_004
Systematic Management of Acute Ellis-3 Coronary Perforation Caused by Cutting Balloon: Case Report on Rescue With Covered Stenting
By Muhammad Noor Azalizam Abdullah, Chai Yih Tan, Kai Soon Liew, Prabahkar Subramaniam, Christian Sunur, Mohd Khairi Othman, Mohammad Anis Abdul Aziz, Nurul Syifaa Najwa Ahmad Nadzri, Kantha Rao Narasamuloo, Saravanan Krishinan, Dharmaraj Karthikesan
Presenter
Muhammad Noor Azalizam Abdullah
Authors
Muhammad Noor Azalizam Abdullah1, Chai Yih Tan1, Kai Soon Liew1, Prabahkar Subramaniam1, Christian Sunur1, Mohd Khairi Othman1, Mohammad Anis Abdul Aziz1, Nurul Syifaa Najwa Ahmad Nadzri1, Kantha Rao Narasamuloo1, Saravanan Krishinan1, Dharmaraj Karthikesan1
Affiliation
Hospital Sultanah Bahiyah, Malaysia1
View Study Report
CASE20251109_004
Coronary - Complication Management
Systematic Management of Acute Ellis-3 Coronary Perforation Caused by Cutting Balloon: Case Report on Rescue With Covered Stenting
Muhammad Noor Azalizam Abdullah1, Chai Yih Tan1, Kai Soon Liew1, Prabahkar Subramaniam1, Christian Sunur1, Mohd Khairi Othman1, Mohammad Anis Abdul Aziz1, Nurul Syifaa Najwa Ahmad Nadzri1, Kantha Rao Narasamuloo1, Saravanan Krishinan1, Dharmaraj Karthikesan1
Hospital Sultanah Bahiyah, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
The patient is a 71-year-old female with cardiovascular risk factors including hypertension, insulin-dependent diabetes mellitus, and dyslipidemia. She has been on hemodialysis for 5 years due to End-Stage Renal Disease (ESRD). She developed angina and hypotension during hemodialysis. The angina persisted even after its termination; consequently, she was admitted for a Non-ST Elevation Myocardial Infarction (NSTEMI). Otherwise, she did not report symptoms of heart failure or arrhythmia.
Relevant Test Results Prior to Catheterization
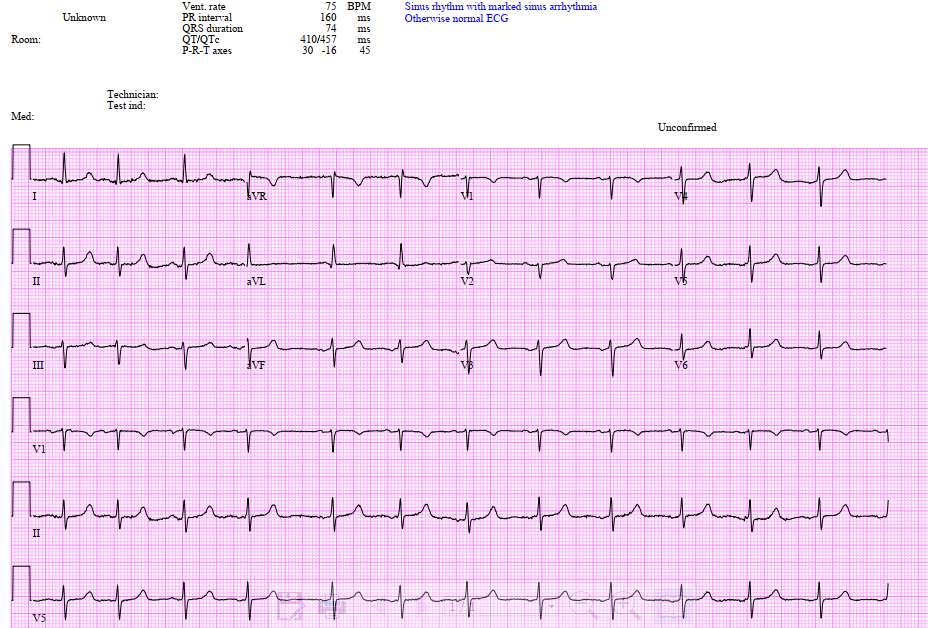
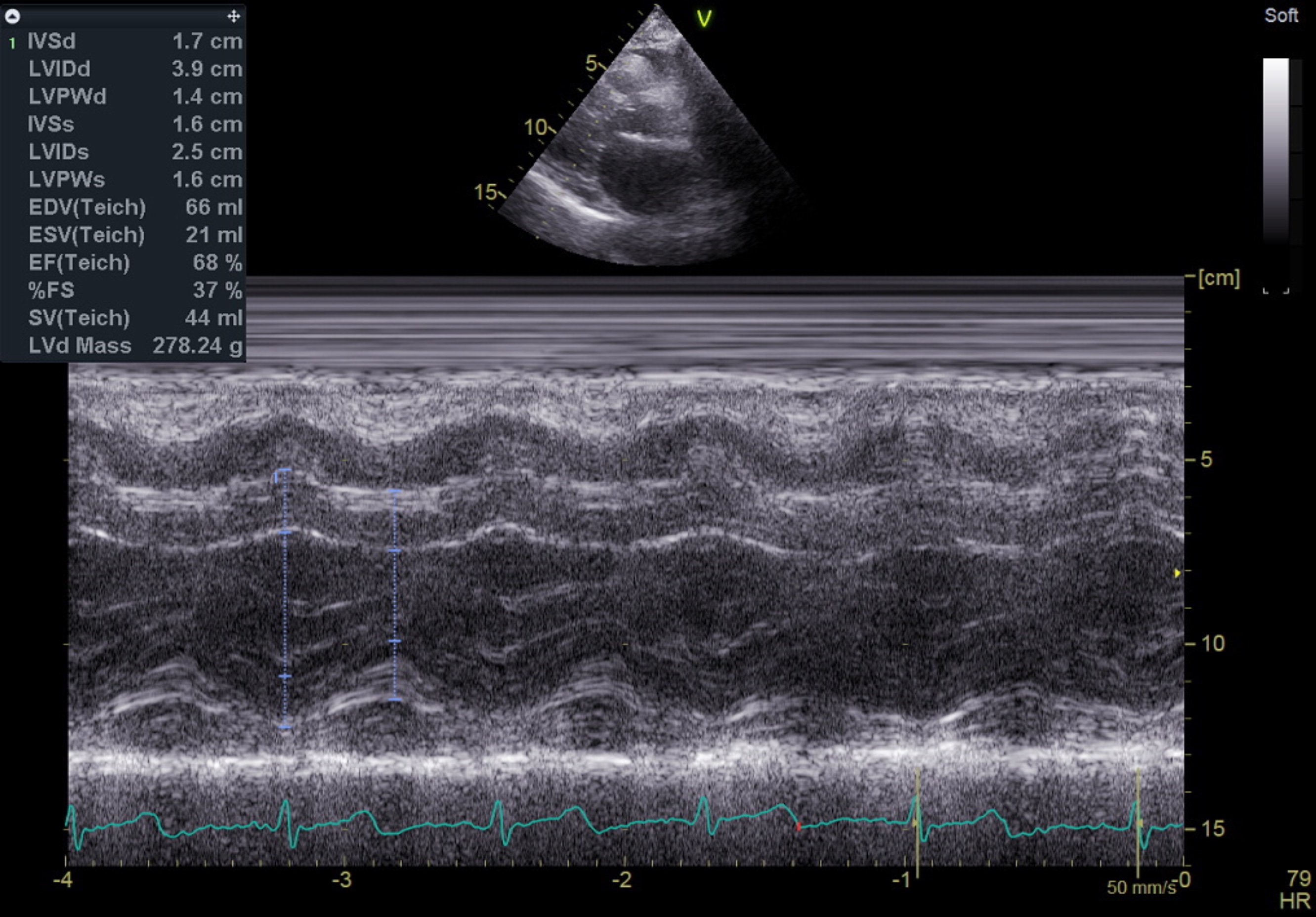
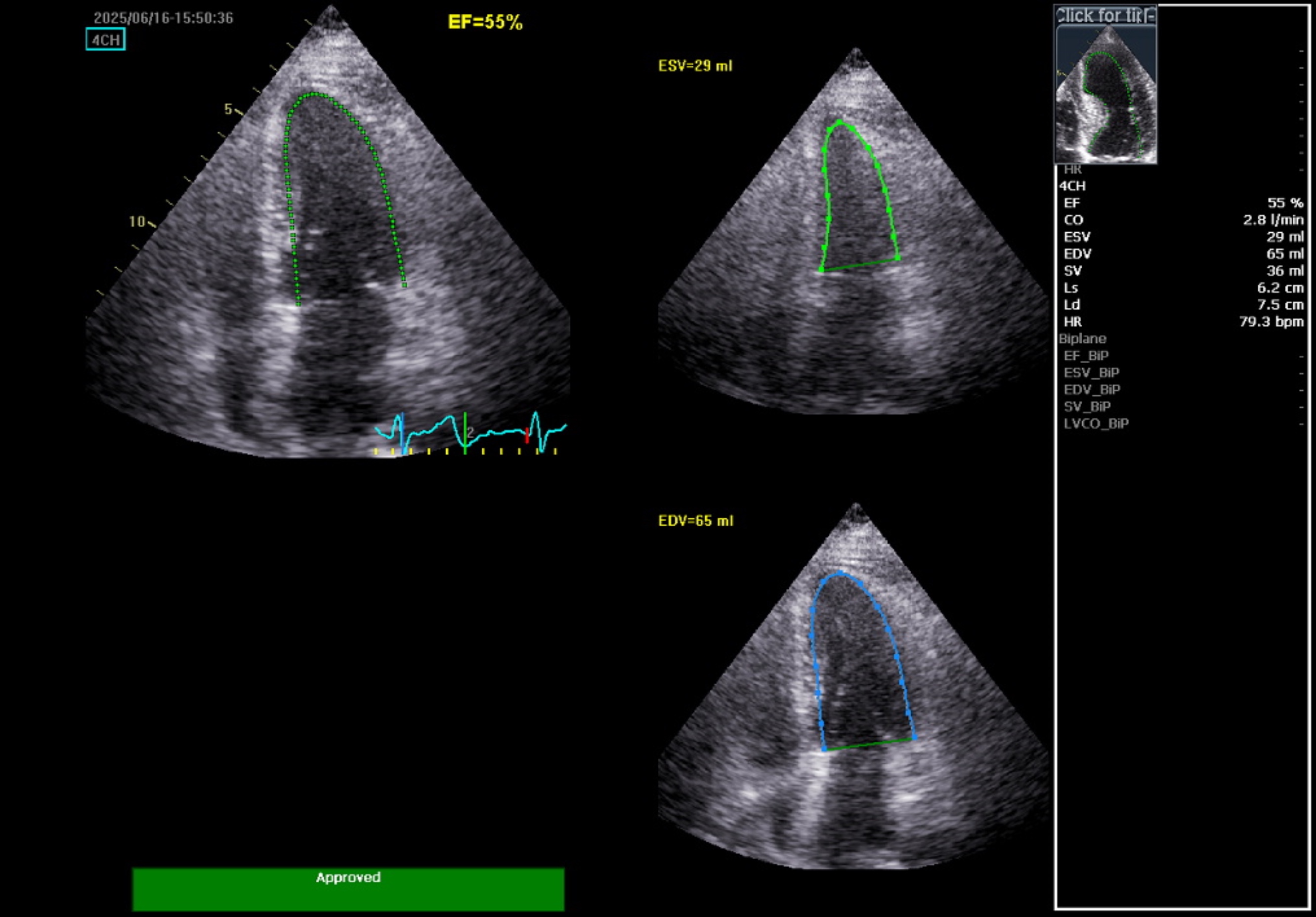
The initial electrocardiogram indicated sinus rhythm and normal axis without Left Ventricular Hypertrophy (LVH). No changes in the ST segment or T wave were noted. High-sensitivity troponin levels were serially elevated, suggesting Myocardial Infarction (MI). The echocardiography, however, showed no regional wall motion abnormality (RWMA) with preserved Left Ventricular systolic function (Ejection Fraction 55%). All cardiac valves were normal with no evidence of stenosis or regurgitation.
 PLAX .mp4
PLAX .mp4
PSAX base 1.mp4
A4C.mp4
Relevant Catheterization Findings
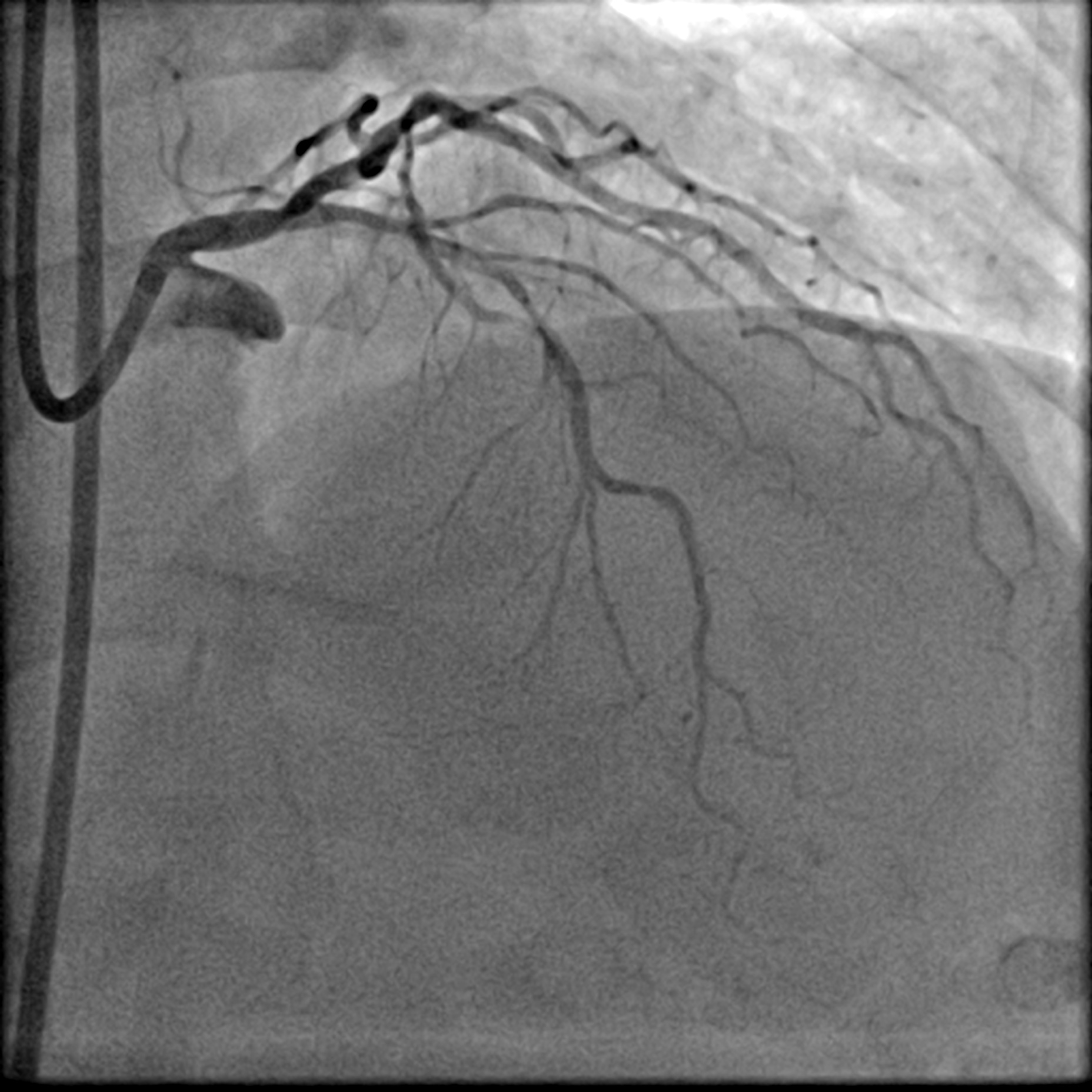
Coronary angiogram showed a Left Main Stem (LMS) bifurcation lesion (Medina 0,1,1) with visible calcification in the proximal left anterior descending artery (LAD). IVUS confirmed severe calcification in the proximal LAD and a calcified nodule causing significant occlusion at the left circumflex artery (LCx) ostium. The right coronary artery (RCA) was spared. Due to severe calcification, a calcium debulking device was required, and the decision was made to proceed with Orbital Atherectomy (OAS).


Interventional Management
Procedural Step
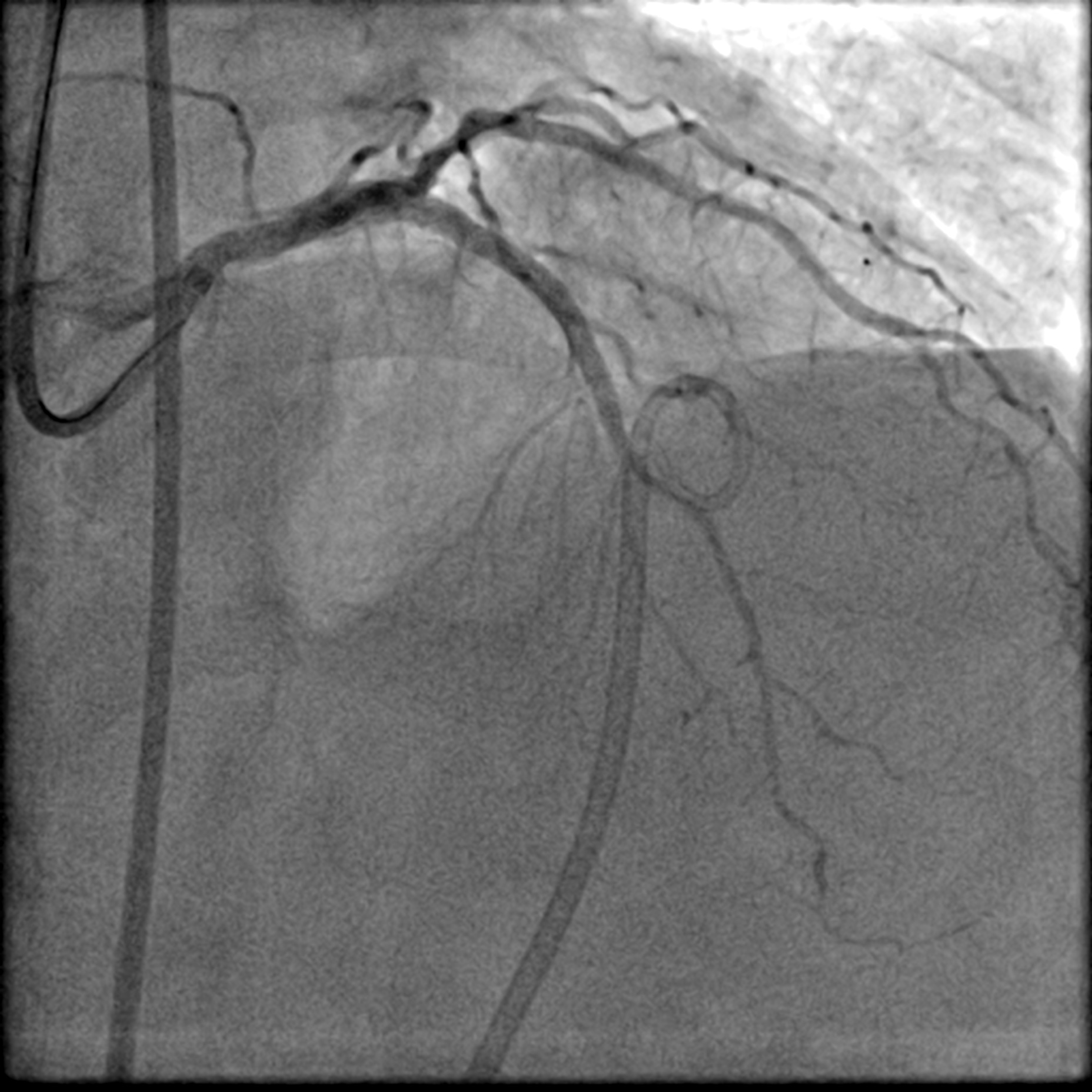
After positioning the ViperWire in the distal LAD, the OAS was delivered, and calcium debulking at low speed was performed safely. Afterward, the LAD was pre-dilated with a 2.5 mm scoring balloon and a 3.5 mm cutting balloon, while the LCx was pre-dilated with a 3.0 mm cutting balloon. A repeat angiogram revealed an Ellis 3 perforation in the proximal LAD, accompanied by a drop in the patient's blood pressure. Expeditiously, a 3.0 mm balloon was inflated at the perforation site, and its location was confirmed with an angiogram, which indicated immediate reduction of the perforation. A pigtail catheter was inserted simultaneously under echocardiographic guidance, and autologous blood transfusion was initiated. The perforation was covered with a 2.5 mm x 20 mm covered stent and post-dilated with a 3.0 mm NC balloon. This reduced the leak, but significant flow persisted. IVUS showed a gap between the stent strut and vessel wall near the LAD carina, allowing for persistent leakage. The covered stent was further post-dilated with a 3.5 mm NC balloon and a hugging balloon technique using two 2.5 mm balloons. These measures failed, as the maximal expansion of the 2.5 mm covered stent is limited to 3.0 mm. A Kissing Balloon Technique (KBT) was attempted at the bifurcation, but it proved futile. Finally, a second 3.5 mm covered stent was placed proximally, which successfully sealed the perforation, leaving only a trivial leak. The hemoperricardium resolved after 24 hours.


Perforated LCA.mp4
FInal LCA AP Cran.mp4
LCA Final LAO Caud.mp4
Case Summary
Severe coronary calcification significantly increases the risk of coronary perforation. It can occur during atherectomy, balloon dilatation, or stenting. Given this risk, operators must be prepared for immediate bailout. Autologous blood transfusion represents a lifesaving procedure, capable of swiftly restoring hemodynamic stability following the enormous blood loss often associated with perforation. The covered stent is among the essential tools for treating coronary perforation. However, achieving successful sealing is highly dependent on correct sizing and ensuring proper post-dilatation. These steps are crucial to guarantee adequate membrane apposition of the stent to the vessel wall.