Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251109_003
From Collapse to Control: A Rescue Voyage in LM Bifurcation Crisis
By Muhammad Anis Abdul Aziz, Chai Yih Tan, Kai Soon Liew, Prabahkar Subramaniam, Christian Sunur, Mohd Khairi Othman, Nurul Syifaa Najwa Ahmad Nadzri, Muhammad Noor Azalizam Abdullah, Kantha Rao Narasamuloo, Saravanan Krishinan, Dharmaraj Karthikesan
Presenter
Muhammad Anis Abdul Aziz
Authors
Muhammad Anis Abdul Aziz1, Chai Yih Tan1, Kai Soon Liew1, Prabahkar Subramaniam1, Christian Sunur1, Mohd Khairi Othman1, Nurul Syifaa Najwa Ahmad Nadzri1, Muhammad Noor Azalizam Abdullah1, Kantha Rao Narasamuloo1, Saravanan Krishinan1, Dharmaraj Karthikesan1
Affiliation
Hospital Sultanah Bahiyah, Malaysia1
View Study Report
CASE20251109_003
Coronary - Complex PCI - Left Main
From Collapse to Control: A Rescue Voyage in LM Bifurcation Crisis
Muhammad Anis Abdul Aziz1, Chai Yih Tan1, Kai Soon Liew1, Prabahkar Subramaniam1, Christian Sunur1, Mohd Khairi Othman1, Nurul Syifaa Najwa Ahmad Nadzri1, Muhammad Noor Azalizam Abdullah1, Kantha Rao Narasamuloo1, Saravanan Krishinan1, Dharmaraj Karthikesan1
Hospital Sultanah Bahiyah, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
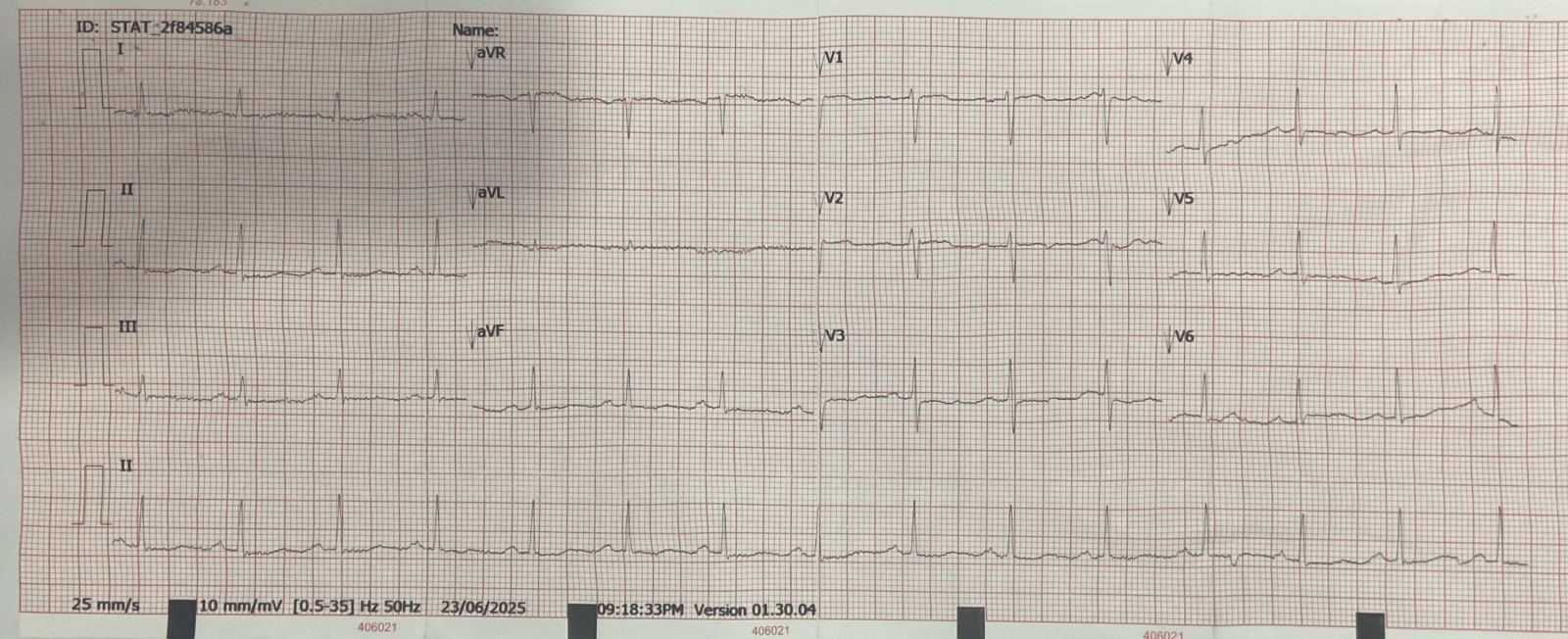
The patient is a 62-year-old female with cardiovascular risk factors including hypertension, Type 2 Diabetes Mellitus requiring oral medication, dyslipidemia, and well-controlled bronchial asthma. She presented with three days of angina, associated with diaphoresis and palpitations. She did not report symptoms of heart failure. During the initial presentation, she was not in shock. Her initial electrocardiogram (ECG) showed subtle generalised ST depression with reciprocal ST elevation over AVR.
Relevant Test Results Prior to Catheterization
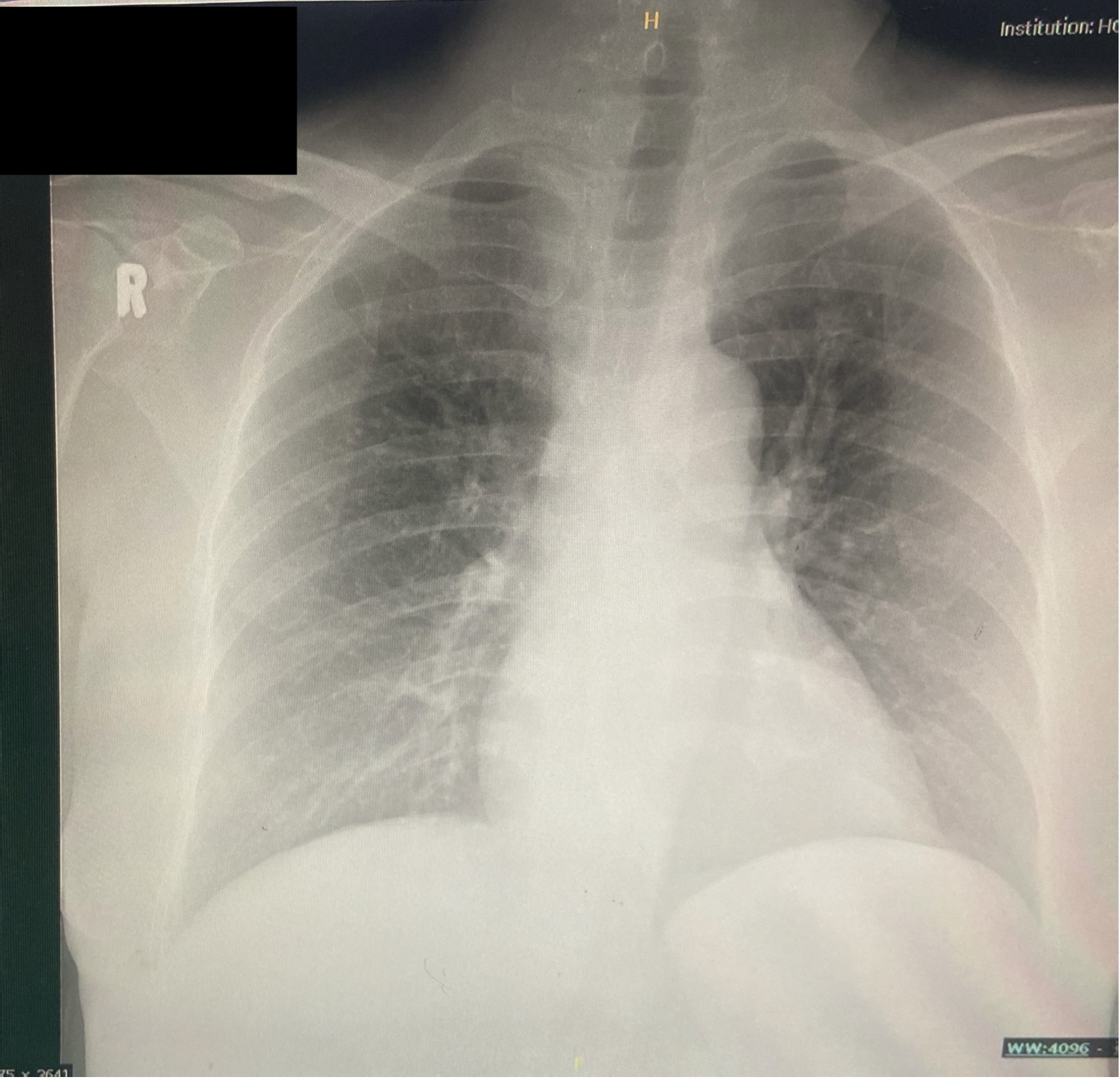
Her initial serum troponin reading was normal, and other blood investigations were unremarkable. The chest x-ray showed no cardiomegaly with clear lung fields. The transthoracic echocardiography revealed hypokinesia involving the base to mid anterior, anteroseptal, and anterolateral walls, extending to the apical anterior wall. The Left Ventricular (LV) Ejection Fraction (EF) was estimated at 41% using Simpson's biplane method, indicating moderately reduced LV systolic function.
Relevant Catheterization Findings
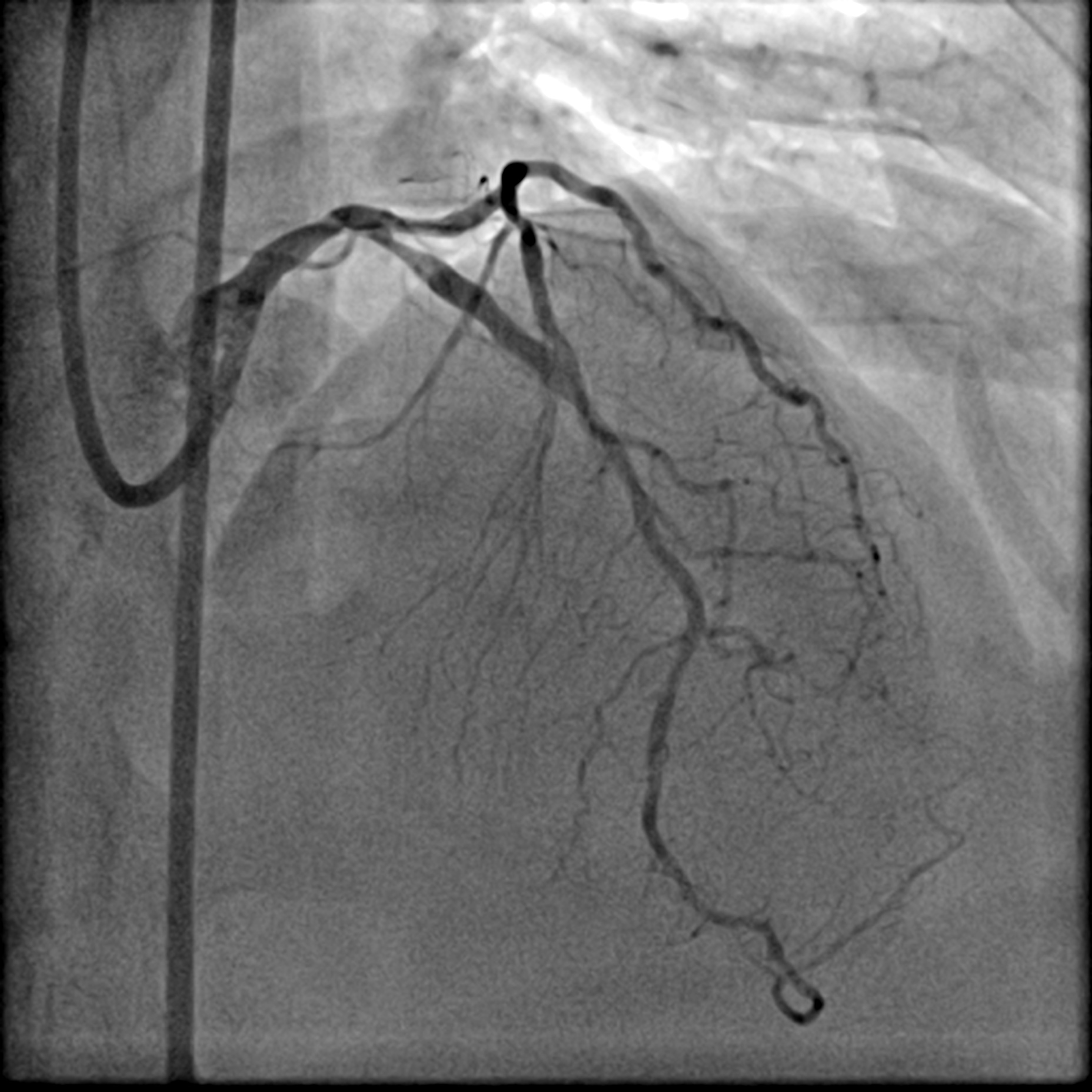
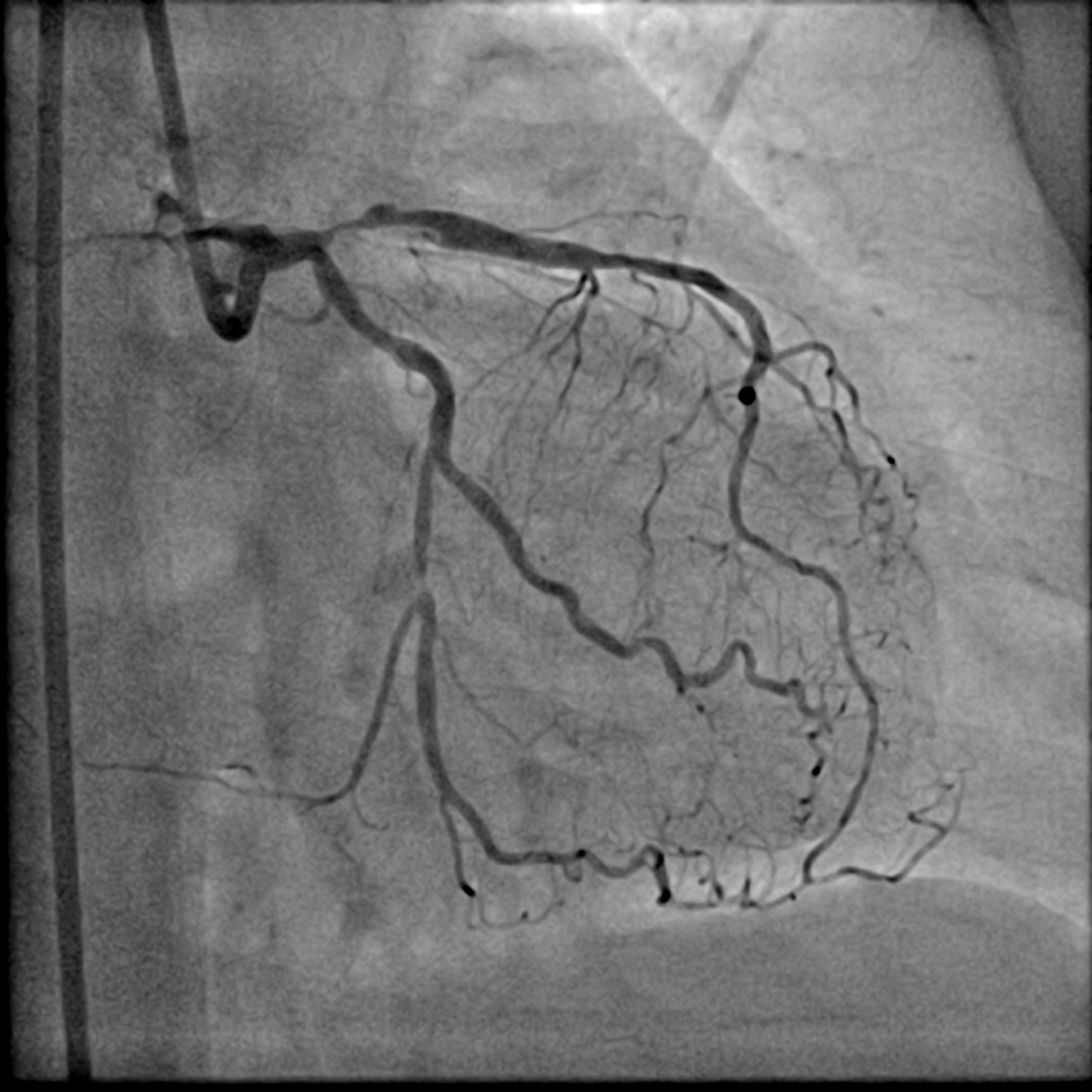
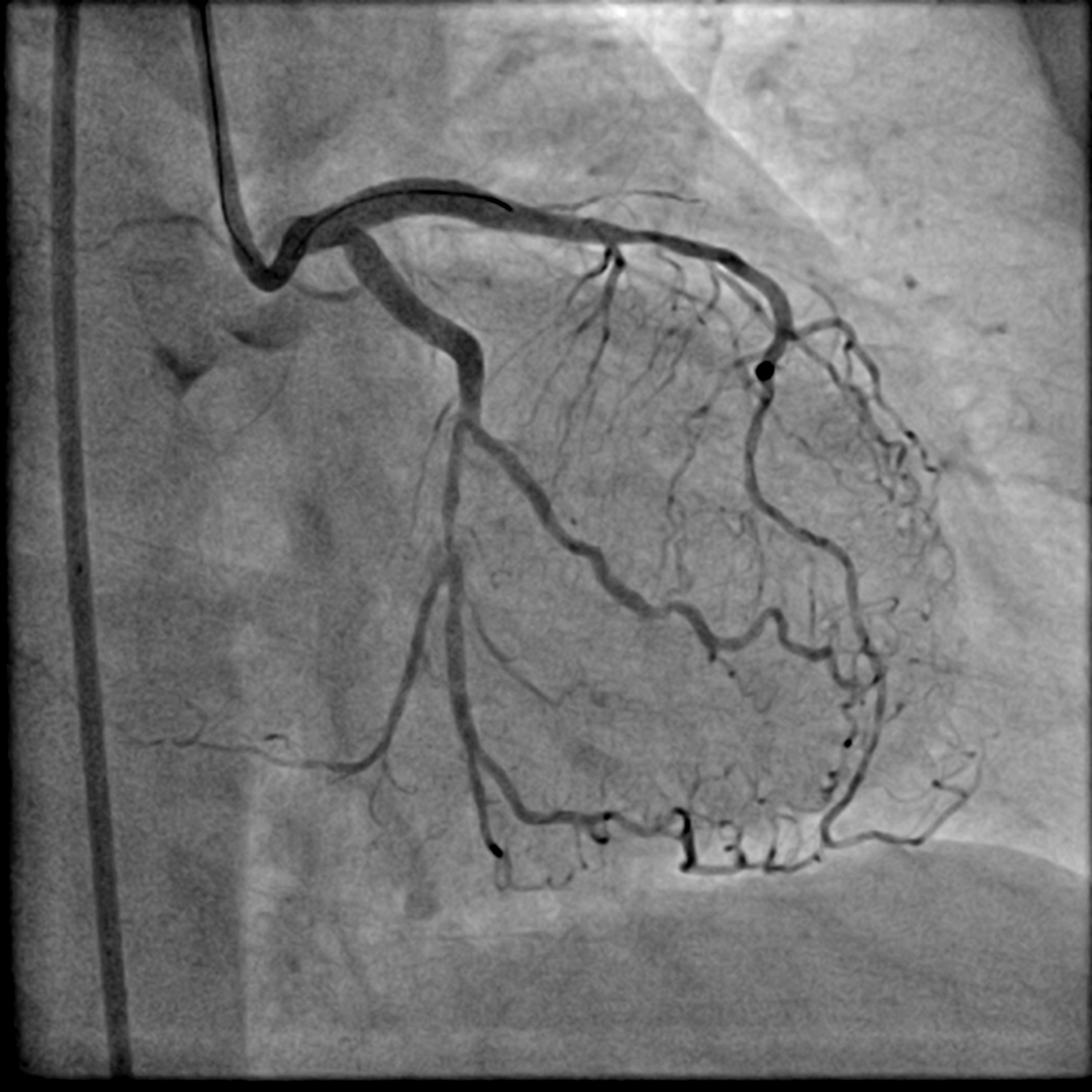
The Right Coronary Artery only had mild disease. There was a Left Main Stem (LMS) bifurcation lesion involving the ostium of the Left Anterior Descending (LAD) artery and the Left Circumflex (LCx) artery (Medina 1,1,1). A conspicuous calcification was visible on fluoroscopy. Intravascular Ultrasound (IVUS) was utilized to further assess the lesion. Its findings correlated with those from fluoroscopy. Specifically, a calcium nodule was identified at the ostium of the LCx in the anti-carina area.

 LCA AP Cran 1.mp4
LCA AP Cran 1.mp4
LCA LAO Caud 1.mp4
LCA AP caudal.mp4
Interventional Management
Procedural Step
A LMS hybrid therapy was planned. A 7 Fr EBU 3.5 catheter was engaged to the LMS. Two workhorse wires were placed in the distal LAD and LCx. The LAD was pre-dilated with a 3.5 mm cutting balloon without facing significant difficulty. However, pre-dilatation of the LCx with a 3.5 mm cutting balloon was unsatisfactory due to the calcium nodule. This was overcome with lesion preparation using a 3.5 mm Lithix balloon. Adequate lesion preparation was confirmed with repeated angiography and IVUS assessment. The ostial LCx was treated with a 3.5 x 20 mm Drug-Coated Balloon (DCB), while the LMS-LAD segment was stented with a 4.0 x 22 mm Drug-Eluting Stent (DES). Proximal Optimization Technique (POT) was performed using a 4.5 mm NC balloon, and the stent in the LAD segment was post-dilated with a 4.0 mm NC balloon. Repeated angiography revealed a Type B dissection with a narrowed lumen in the LCx, necessitating stenting. The LCx was re-wired using a dual-lumen catheter from the inner frame of the LMS stent. The stent strut was opened with a 2.0 mm balloon and a 3.5 mm NC balloon. T-stenting of the ostial LCx was performed with a 3.0 x 26 mm DES, utilizing a balloon catheter in the LAD wire as a marker. The LCx stent was first post-dilated with a 3.5 mm NC balloon. Subsequently, the Kissing Balloon Technique (KBT) was performed with a 4.0 mm NC balloon in the LAD and a 3.5 mm NC balloon in the LCx. Finally, repeated POT was completed with a 4.5 mm NC balloon in the LMS.


Dissected LCx.mp4
LCA final AP cran.mp4
LCA final AP Caud.mp4
Case Summary
The novel hybrid therapy for complex bifurcation lesions, combining a DES in the main branch and a Drug-Coated Balloon DCB in the side branch, is an attractive alternative strategy. This approach effectively reduces the burden of metallic stent struts around the coronary bifurcation, thereby mitigating the risk of long-term lesion failure. Crucially, bailout stenting iof the side branch must be thoroughly prepared beforehand. In scenarios of unsatisfactory lesion preparation or a flow-limiting dissection in the side branch. Given the 90 degree angulation of the side branch, T-stenting is often selected as the most mechanically appropriate bailout method to achieve optimal sealing.