Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251109_002
Coronary Guide Wire Failure: Percutaneous Retrieval of an Unraveled Wire Mimicking a Trapped Foreign Body
By Nurul Syifaa Najwa Ahmad Nadzri, Chai Yih Tan, Kai Soon Liew , Prabahkar Subramaniam , Christian Sunur , Mohd Khairi Othman, Mohammad Anis Abdul Aziz, Muhammad Noor Azalizam Abdullah, Kantha Rao Narasamuloo, Saravanan Krishinan, Dharmaraj Karthikesan
Presenter
Nurul Syifaa Najwa Ahmad Nadzri
Authors
Nurul Syifaa Najwa Ahmad Nadzri1, Chai Yih Tan1, Kai Soon Liew 1, Prabahkar Subramaniam 1, Christian Sunur 1, Mohd Khairi Othman1, Mohammad Anis Abdul Aziz1, Muhammad Noor Azalizam Abdullah1, Kantha Rao Narasamuloo1, Saravanan Krishinan1, Dharmaraj Karthikesan1
Affiliation
Hospital Sultanah Bahiyah, Malaysia1
View Study Report
CASE20251109_002
Coronary - Complication Management
Coronary Guide Wire Failure: Percutaneous Retrieval of an Unraveled Wire Mimicking a Trapped Foreign Body
Nurul Syifaa Najwa Ahmad Nadzri1, Chai Yih Tan1, Kai Soon Liew 1, Prabahkar Subramaniam 1, Christian Sunur 1, Mohd Khairi Othman1, Mohammad Anis Abdul Aziz1, Muhammad Noor Azalizam Abdullah1, Kantha Rao Narasamuloo1, Saravanan Krishinan1, Dharmaraj Karthikesan1
Hospital Sultanah Bahiyah, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
The patient is a 32-years-old gentleman who has no comorbidity & cardiovascular risk factor. He was never admitted for acute coronary syndrome but had been experiencing disabling stable angina for a year. The angina was disabling & refractory to standard medical treatment. Otherwise he had no heart failure symptoms.
Relevant Test Results Prior to Catheterization
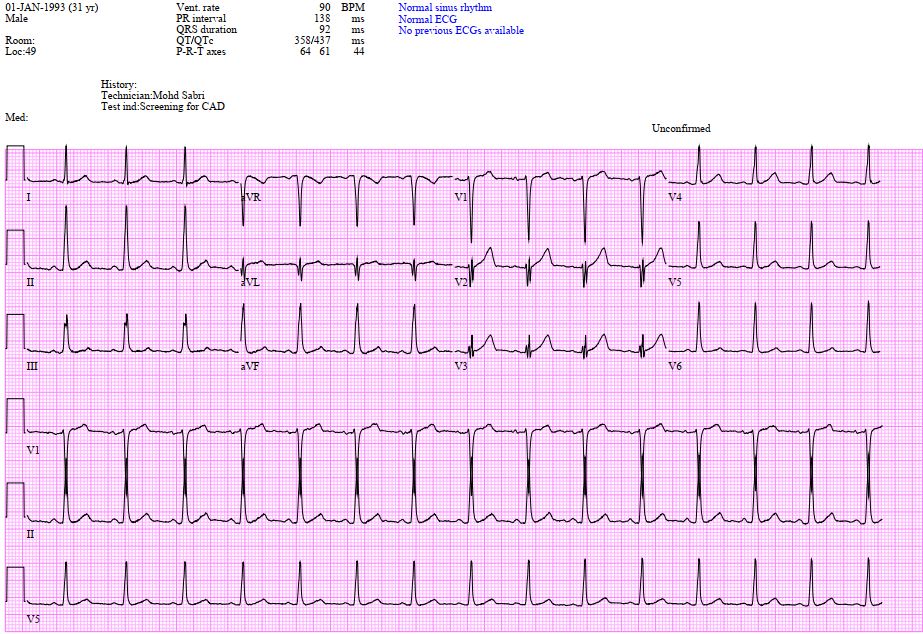
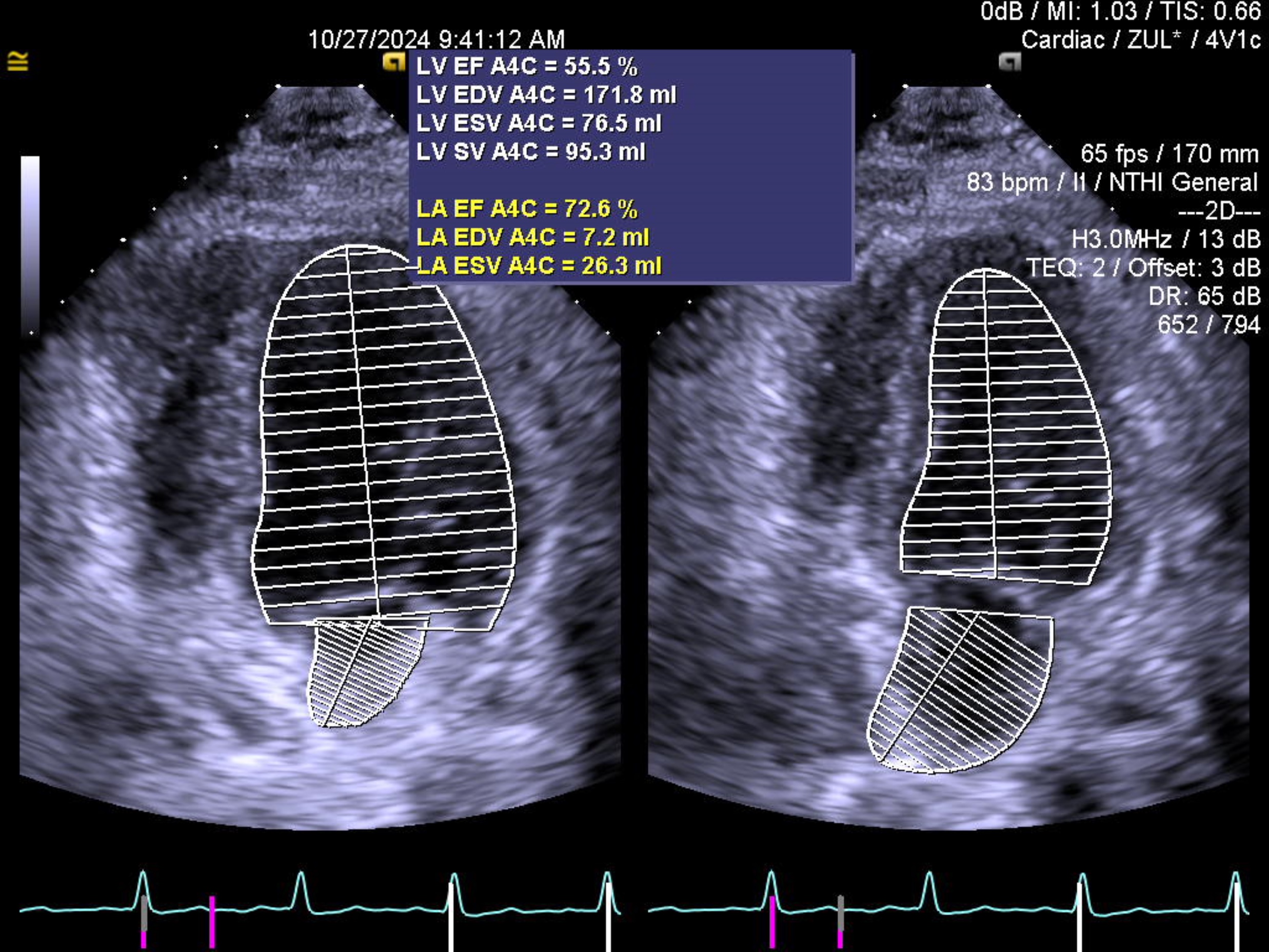
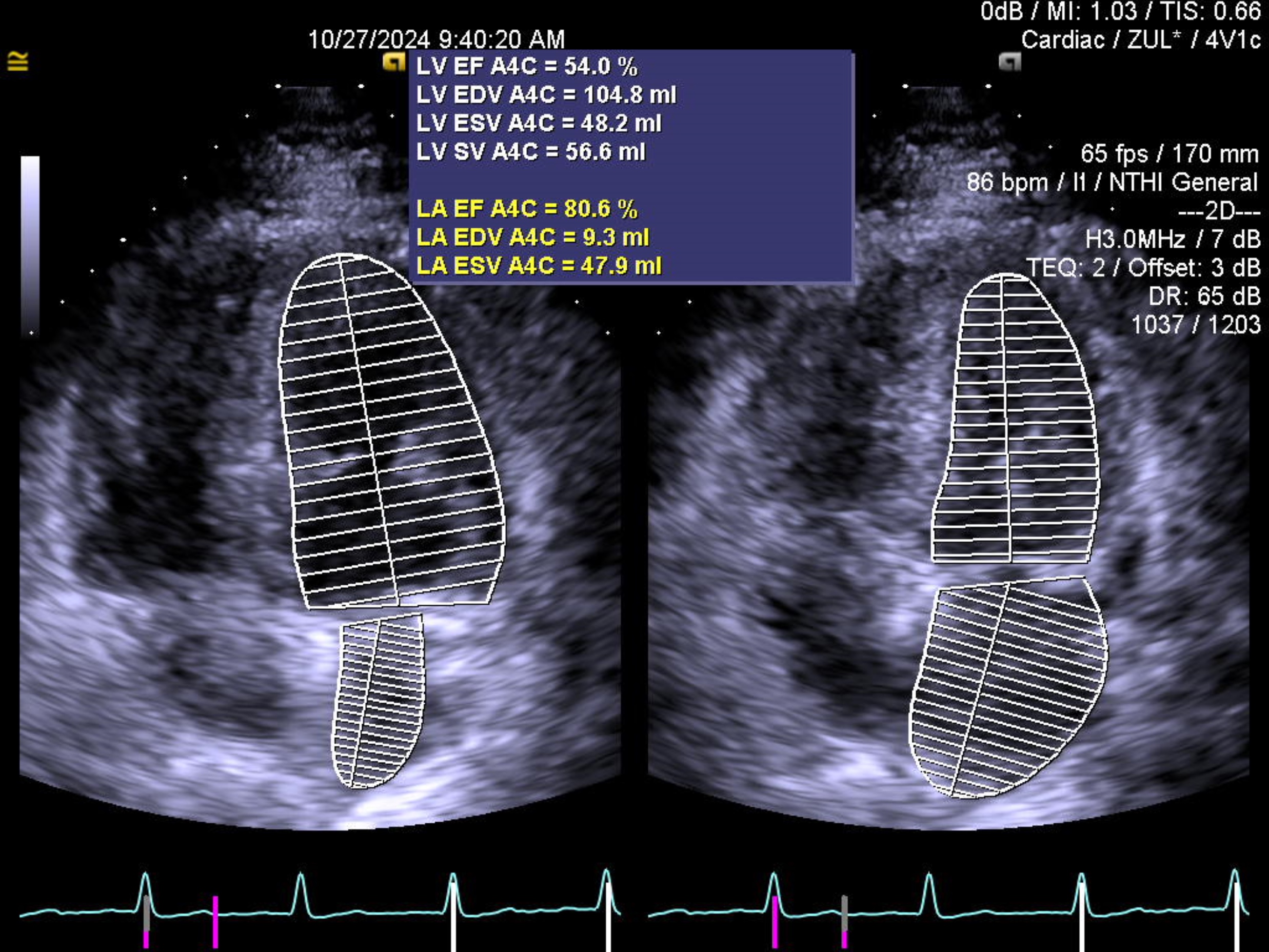
His blood investigations were unremarkable with a normal troponin reading. The electrocardiography shows sinus rhythm with normal axis, absence of left ventricular hypertrophy, Q wave, ST deviation or T wave inversion. The echocardiography showed no regional wall motion abnormality with normal left ventricular ejection fraction. A computed tomography of coronary artery revealed a subtotal occlusion over the left anterior descending artery (LAD).
 plax.mp4
plax.mp4
PSAX base.mp4
psax base 2.mp4
Relevant Catheterization Findings
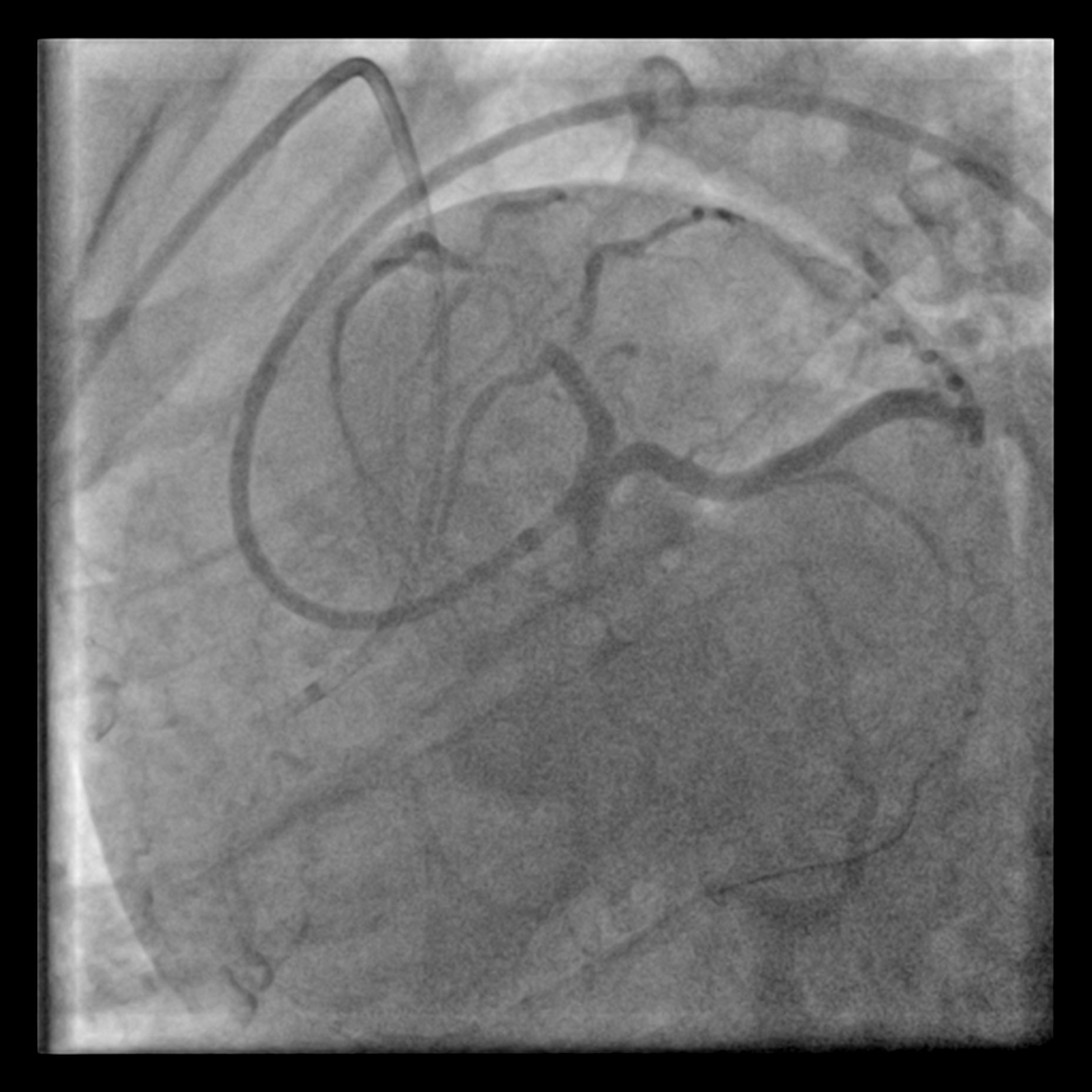
The proximal LAD demonstrates a Chronic Total Occlusion (CTO) with collateral flow from the Right Coronary Artery (RCA) via a septal perforator. The J-CTO score is 2, attributed to a blunt proximal cap and an estimated lesion length of more than 20 mm. The indication for CTO intervention is angina refractory to medical therapy. The procedure was planned using an antegrade approach via a 7 Fr EBU 3.5 catheter, with a contralateral injection from the RCA for visualisation.

LCA pre.mp4
LCA pre 2.mp4
Interventional Management
Procedural Step
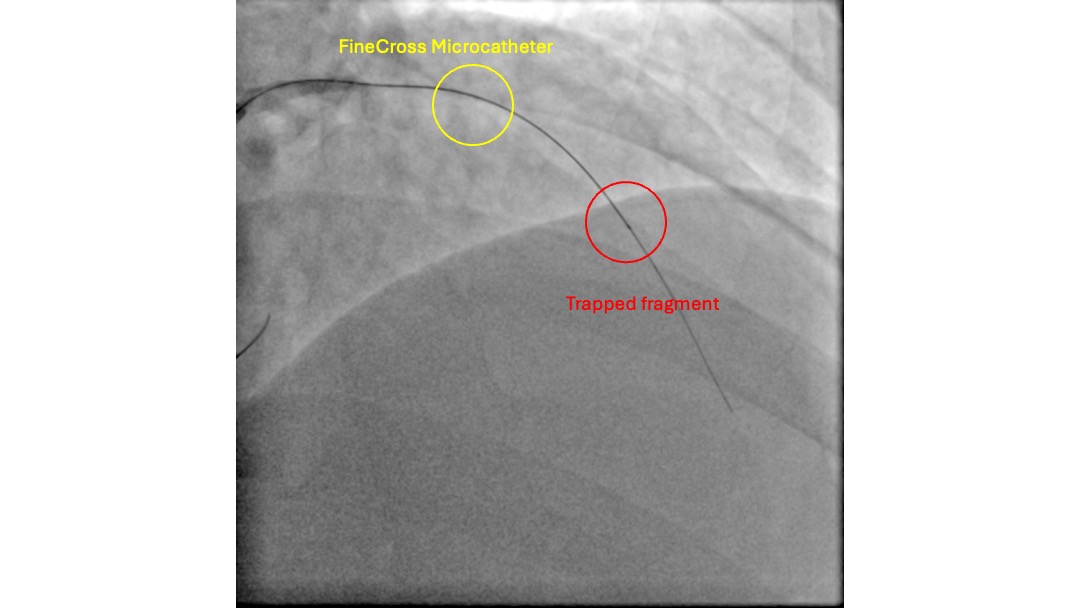
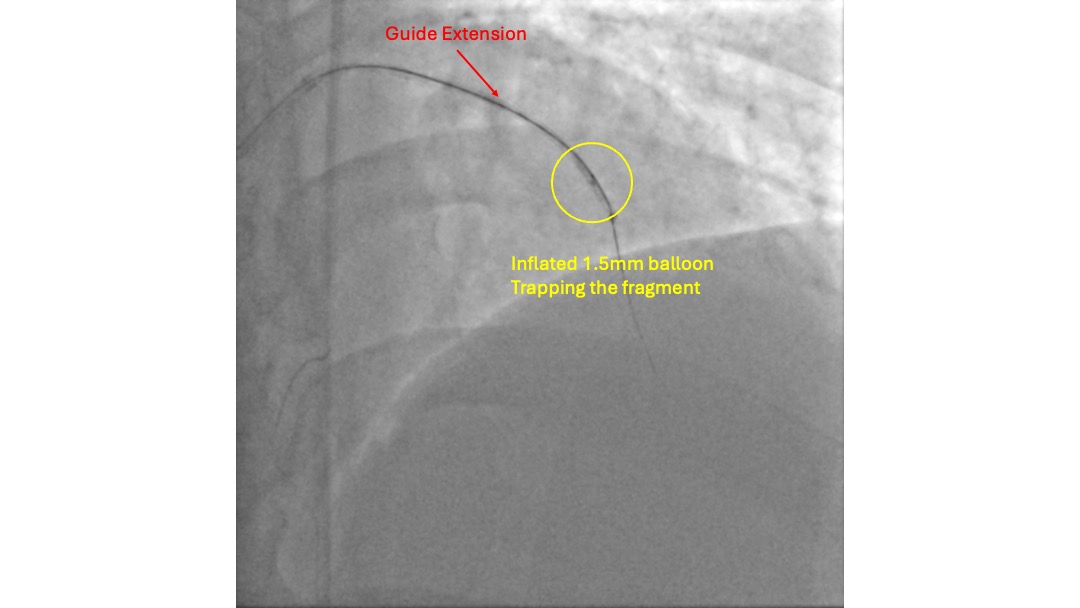
With the support of a FineCross micro-catheter (MC), the proximal CTO cap was punctured with a Gaia First wire. The wire traversed the CTO body through the intra-plaque space without much difficulty, reaching the distal lumen, which was confirmed by contralateral injection. However, the MC could not be delivered to the distal lumen over the Gaia First wire. The CTO lesion was pre-dilated with a 1.0 mm balloon, but it burst during the fourth inflation, and the MC still failed to advance. Subsequently, a trapped foreign body was noted on the distal aspect of the wire that prevented the advancement of the MC. This was initially thought to be a fragment fractured from the 1.0 mm balloon. The intervention was continued over the Gaia First wire to facilitate the removal of the fragment. The lesion was pre-dilated with a 2.5 mm non-compliant (NC) balloon and a 3.5 mm cutting balloon. Two 3.5 mm drug-coated balloons (DCBs) were then used to treat the lesion. With adequate luminal gain, an extension catheter was advanced into the LAD, and the fragment was retrieved inside it. A 1.5 mm balloon was then deployed to trap the fragment inside the extension catheter. The wire, extension catheter, and inflated 1.5 mm balloon were then removed simultaneously from the LAD. Inspection of the wire revealed that the fragment was, in fact, an unraveled coronary wire rather than a fractured balloon.

Case Summary
The intervention was continued to prevent dislodgement of the fragment in the tight lesion during wire removal. However, extra caution was exercised during manipulation of the Gaia First wire to prevent arterial perforation. The method used to remove the fragment was adapted from the balloon trapping technique used for coronary wire fixation in a guiding catheter. Unraveling of a coronary wire is an uncommon complication. This can occur due to aggressive wire manipulation, calcified lesions, or wire entrapment.