Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251108_004
Early Restoration of Sinus Rhythm by Thoracoscopic Left Atrial Appendage Resection in a Patient With Atrial Fibrillation, Left Atrial Appendage Thrombus, and Heart Failure With Reduced Ejection Fraction
By Shota Kawabata, Akinori Matsumoto
Presenter
Shota Kawabata
Authors
Shota Kawabata1, Akinori Matsumoto1
Affiliation
Sumitomo Hospital, Japan1
View Study Report
CASE20251108_004
Structural - LAAO
Early Restoration of Sinus Rhythm by Thoracoscopic Left Atrial Appendage Resection in a Patient With Atrial Fibrillation, Left Atrial Appendage Thrombus, and Heart Failure With Reduced Ejection Fraction
Shota Kawabata1, Akinori Matsumoto1
Sumitomo Hospital, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
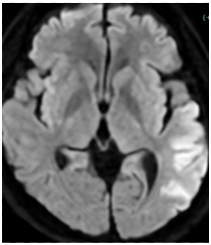
A 53-year-old man was admitted to our hospital with a diagnosis of cardioembolic stroke after the sudden onset of aphasia and conjugate deviation of the eyes. On admission, his blood pressure was 111/73 mmHg, and his heart rate was 111 beats per minute with an irregular rhythm. The respiratory rate was 20 breaths per minute, and oxygen saturation was within the normal range. Physical examination revealed no cardiac murmurs, with only mild bilateral leg edema noted.
Relevant Test Results Prior to Catheterization
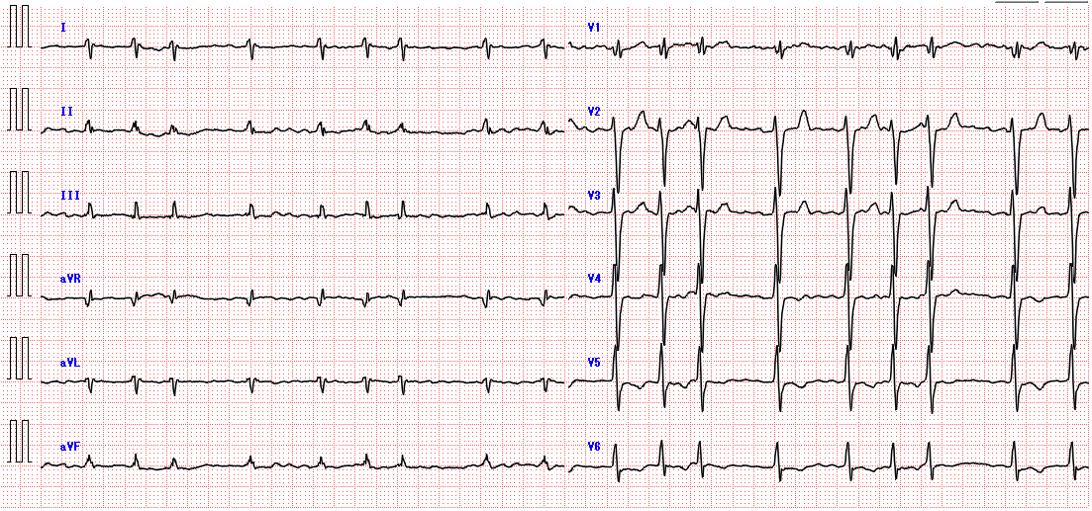
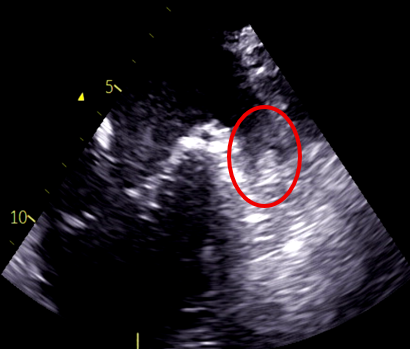
Electrocardiogram showed atrial fibrillation with a heart rate of 116 bpm and no significant ST-segment changes. Chest radiography showed cardiomegaly. Laboratory analysis showed an elevated NT-proBNP of 6103pg/mL. Transthoracic echocardiography demonstrated an ejection fraction of 15%, left atrial diameter of 60mm, global wall motion abnormalities. Transesophageal echocardiography confirmed the presence of a thrombus in the LAA.
 Transthoracic echocardiography.mp4
Transthoracic echocardiography.mp4
Relevant Catheterization Findings
Coronary angiography revealed no significant stenosis, suggesting tachycardia-induced cardiomyopathy or dilated cardiomyopathy. On hospital day 27, the results of the right heart catheterization showed a mean pulmonary artery wedge pressure of 23 mmHg, a mean pulmonary artery pressure of 27 mmHg, a right atrial pressure of 9 mmHg, and a cardiac index of 1.4 L/min (by Fick). We adjusted the diuretics and cardioprotective agents while also considering the addition of inotropic agents.
Interventional Management
Procedural Step
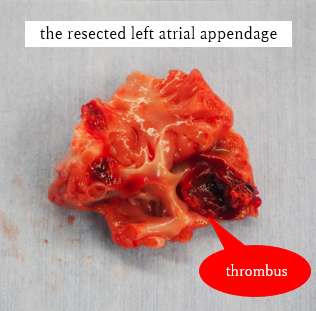
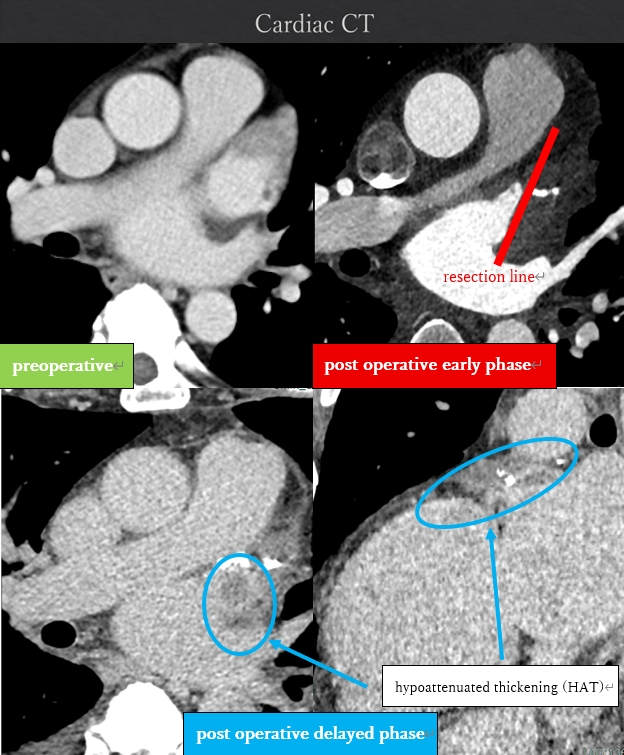
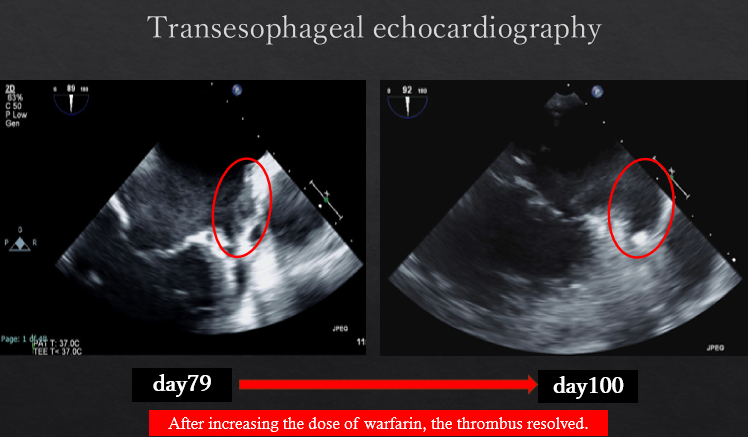
The patient had reduced left ventricular function, and tachycardia-induced cardiomyopathy was initially suspected. We therefore aimed for early restoration of sinus rhythm. Despite treatment with rivaroxaban, the patient developed a cardioembolic stroke, and a thrombus persisted in the LAA. Anticoagulation was switched to warfarin. During stroke rehabilitation and optimization of cardioprotective therapy, we monitored the thrombus for resolution, but it remained unchanged. Because an LAA occlusion device cannot be used in the presence of an existing thrombus, and thoracoscopic LAA resection is feasible when the thrombus does not extend to the LAA base, we decided to perform thoracoscopic LAA resection on hospital day 70. Intraoperative transesophageal echocardiography confirmed the absence of thrombus at the LAA base before resection. A thrombus was found within resected LAA specimen. However, postoperative computed tomography on hospital day 79 revealed hypoattenuated thickening (HAT) at the resection stump, suggestive of thrombus formation. Transesophageal echocardiography confirmed this finding. After intensifying warfarin management, the thrombus resolved approximately 20 days later. Catheter ablation was subsequently performed on hospital day 115, and the patient has since maintained sinus rhythm.
LAA resection.mp4
Case Summary
Thoracoscopic LAA resection enabled early rhythm control even in the presence of an LAA thrombus. However, postoperative thrombus formation at the resection site remains a risk, and careful follow-up is essential.